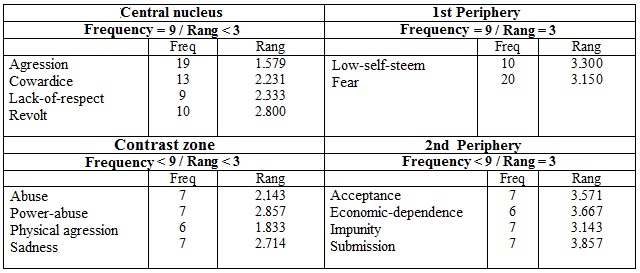
Figure 1: Four-quadrant chart of the representations of domestic violence against women of nursing professionals acting in Family Health Units in the municipality of Rio Grande, RS, Brazil, 2013.
ORIGINAL RESEARCH
Nursing personnel's social representations of domestic violence against women: a structural approach
Cristiane Lopes AmarijoI; Vera Lúcia de Oliveira Gomes II; Antonio Marcos Tosoli GomesIII; Adriana Dora da FonsecaIV; Camila Daiane SilvaV
I
PhD student in nursing, Federal University of Rio Grande. Rio Grande, Rio
Grande do Sul, Brazil. E-mail:
cristianeamarijo@yahoo.com.br
II
PhD in Nursing.Professor at the Federal University of Rio Grande. Rio
Grande, Rio Grande do Sul, Brazil. E-mail: vlog1952@gmail.com
III
PhD in Nursing. Full Professor at the State University of Rio de Janeiro.
Nursing school. Rio de Janeiro, Rio de Janeiro, Brazil. E-mail: mtosoli@gmail.com
IV
PhD in nursing Professor at the Federal University of Rio Grande. Rio
Grande, Rio Grande do Sul, Brazil. E-mail: adriana@vetorial.net
V
PhD in nursing Federal University of Rio Grande. Rio Grande, Rio Grande do
Sul, Brazil. E-mail: Camilad.silva@yahoo.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2017.23648
ABSTRACT
Objective: to analyze the social representations of domestic violence against women held among nurses and nursing technicians working in family health centers in the municipality of Rio Grande (RS). Methodology: this exploratory, descriptive, qualitative social study was based on the structural and procedural approaches of Social Representations Theory. Data were collected through evocations and interviews conducted between July and November 2013. The evocations were treated using EVOC 2005 software. The interviews were subjected to content analysis and manipulated using NVivo 10 software. The study project was approved by the research ethics committee of Rio Grande Federal University (Opinion No. 020/2013). Results: the terms found in the central core of the representation among nurses and nursing technicians were aggression, cowardice, disrespect and revolt. Conclusion: the informants' representation was found to be structured and with negative connotations.
Keywords: Domestic violence; battered women; family health strategy; nursing.
INTRODUCTION
Violence against women is a global historical, multifactorial and complex phenomenon, linked to power, privileges, and male control. This phenomenon presents different levels of severity1-3 and constitutes a serious public health problem, due to its magnitude, severity, recurrence and negative consequences on the quality of life of the victims 1-5.
Women in situations of violence frequently attend health services, especially those focused on primary care6. In this context, the family health units (FHUs) stand out for the early detection of the cases, since, due to the proximity with the community, the professionals have knowledge of the problems that affect the people,7 including domestic violence against women (DVAW).
However, victim care can be influenced by the representation that professionals involved in care have about the DVAW8. Social representation (SR) consists of a set of thoughts, ideas and beliefs resulting from social interactions, common to a given group of individuals 9-11.
To generate SR, the object to be studied needs to present "cultural relevance or social consistence" 12:45, that is, the group to be searched must have a representation of the object to be investigated. The object also needs to be present in some practice of the group12. Issues of social relevance, such as health and illness, require individuals to formulate theories based on their experiences, information and values, whether at the individual or collective level13.
It is the duty of the professional to provide care in a humanized and integral manner, from a holistic view, in order to meet the biopsychosocial needs of the users that seek the health service. In this sense, professionals who work directly providing care for victims should be able to receive them effectively and detect cases of DVAW4. This requires them to get rid of prejudices and judgments.
Not only the measures aimed at curbing and preventing DVAW constitute a major challenge, but also providing a humanized treatment for the victims. The transformation of culturally based beliefs and values, transmitted through many generations, thus reproducing and trivializing violence in gender relations, deserves discussions7.
By believing that SRs of nursing professionals about DVAW are built from the intertwining of personal and professional experiences and that cultural aspects can influence their construction, and also believing that SRs about DVAW influence care practices to victims, as well as the planning of actions and interventions for prevention and combat of the DVAW, we opted to analyze the SRs about domestic violence against women among nurses and nursing technicians working in the FHUs of the Municipality of Rio Grande/RS.
THEORETICAL-METHODOLOGICAL REFERENCE
Social, exploratory, descriptive, and qualitative research conducted according to structural and procedural approaches. The study was developed in 12 FHUs located in the urban zone and seven in the rural zone of the Municipality of Rio Grande/RS, Brazil. The structural approach was used because it allows knowing the structure of the SR. As for the procedural approach, this was chosen because it allows knowing the processes of construction of the SRs, the social practices that generate and justify them14, besides their constituent aspects like information, images, opinions, among others15.
Data collection took place from July to November 2013, through the technique of Free Evocations and interviews. In each unit, a room was made available away from the circulation area to avoid distractions during collection.
Sixty-five nursing professionals participated in the evocations; they were asked to verbalize the first five words or expressions that came to mind before the inducing term domestic violence against women. Afterwards, we interviewed 25 informants using a semi-structured script, with a view to highlight the constituent elements of the SRs, such as information, images, beliefs, values, cultural and ideological elements, among others.
To determine the number of interviews, the FHUs were grouped by proximity, giving rise to four areas in the urban zone, and six in the rural zone. One FHU was chosen from each area to conduct the interviews, with at least one nurse and one nursing technician being invited. Nursing professionals who refused to participate in the survey, as well as those who were away from the FHU due to vacation, day off, or on leave, were excluded.
The analysis of the evocations was carried out in the Ensemble of Permettant Programs L'analyze des Evocations Software - EVOC 2005. This computer resource adopts the criteria of frequency and order of appearance of the terms evoked for the elaboration of a four-quadrant chart, through which the central nucleus (CN), the contrast elements and the peripheral system are specified16,17. This construction makes possible the structural and procedural analysis of the representation. For the treatment of interview data, we used the technique of content analysis 18, and selected excerpts from the interviews to contextualize the terms presented in the four-quadrant chart.
The speeches were identified by the letters N (nurse) and NT (nursing technician) followed by the Arabic numeral corresponding to the order of collection of the evocations, in order to assure anonymity. The project was approved by the Research Ethics Committee of the Federal University of Rio Grande, under Opinion nº 020/2013.
RESULTS AND DISCUSSION
Sixty-five professionals participated in the evocations; of these, 26 were N and 39, NT. The informants of the interviews were 13 N and 12 NT. Forty-four professionals worked in the urban zone, 18 N and 26 NT, while in the rural zone there were eight N and 13 NT. The age ranged from 27 to 60 years, predominantly from 40 to 49 years, with 31 participants. As for the marital status, 33 participants lived with a partner, a situation that can prompt the experience of domestic violence.
The Corpus formed by the evocations before the inducing term domestic violence against women resulted in 136 different words mentioned in a total of 325 times. On a scale of one to five, the average of the mean order of evocation (MOE) was three, the minimum frequency six, and the mean frequency, nine. Data analysis resulted in a four-quadrant chart. See Figure 1.
Figure 1:
Four-quadrant chart of the representations of domestic violence against
women of nursing professionals acting in Family Health Units in the
municipality of Rio Grande, RS, Brazil, 2013.
The most relevant and significant terms for the subjects are placed in the upper left quadrant, thus constituting the CN of the social representation 17. The terms present in the CN are those more readily evoked and quoted more frequently by informants11,19.
The combination of frequency and mean order of evocation of words makes it possible to survey the terms that are likely to compose the CN 11. These are in limited numbers and are not equivalent to each other, being some more important than others, thus conferring a hierarchy to the central system9 "to seek the central nucleus, then, to seek the root, the social foundation of the representation [...]" 9:40.
The SRs are structured from three dimensions20: concept/information, attitude/judgment and image/field of representation. The concept consists of the information, that is, the knowledge that a certain group has about an object. The attitude is the opinion, the judgment that the group has on the object in question. Thus, the opinion "is, on the one hand, a socially valued formula to which a subject adheres and, on the other hand, a position on a controversial [discussed] problem of society"20:43. The image, or mental sensations, represents the impressions that people or objects leave in our brain. Therefore, we sought to identify the dimensions cited in the constituent terms of the CN of the representation of N and NT about the DVAW. In order to contextualize the probable elements of the CN, we present excerpts extracted from the interviews.
It is noticed that the elements of the CN contemplate the conceptual, imaginary and attitudinal dimensions. The term aggression, the more frequent and more readily evoked, constitutes the information that the professionals had about violence. It also assumes the imagery dimension, portraying the distinct forms of DVAW, as well as the marks left by physical violence. Traditionally, violence is closely related to physical aggression. It is the most recognized, and the socially considered the most dangerous, and with higher prevalence21.
When you think about domestic violence against women, the first thing you think about is physical aggression, but I think domestic violence is not just about physical violence. Physical violence happens a lot because it's the form of violence that people see the most, that we listen to on the radio, see on TV, in the newspaper, that goes to the media, that appears with the artists, that ends up generating the scandals. Besides physical violence, there is a hidden violence also, behind it, which is the psychological violence, which I think happens much more often; so, I think it is every form of abuse [...] (N-144)
Domestic violence against women consists in all kinds of verbal, physical, mental aggression. Every kind of aggression is violence [...] (NT-54)
The terms cowardice and lack of respect refer to the judgment that the practitioners issued on violence against women. In a study1, the word disrespect associated with alcohol appeared as one of the triggers of aggressive acts against women living in rural areas of the southern half of the state of Rio Grande do Sul.
Domestic violence against women is cowardice [...] (N-11)
Domestic violence against women means a disregard, a lack of respect for the woman at home [...] (N-103)
The word revolt represents the feeling of nurses and nursing technicians before the reconciliation of the victim with the aggressor. The complex nature of violence can generate feelings of insecurity, frustration, anger, indignation, fear and anguish in professionals for not being able to solve it, for not visualizing a response and the effective results of care provided22.
Sometimes the person comes on the other day totally different, it's another version, although we know of what happened... that she was attacked... in the other day, the version changed, that is revolting! (NT-138)
The words aggression, cowardice and lack of respect also integrated the CN of the SR of health professionals participating in another study on domestic violence against women, in which the informants were nurses, nursing technicians, physicians and community health agents working at FHUs. This finding provided evidence that these professionals have a SR with negative and structured connotation, because their CN is formed by elements that integrate the conceptual, imagery and attitudinal dimensions23.The CN of the SR of community health agents and technicians aged less than 41 years before the inducing termdomestic violence against women was formed by the words aggression, cowardice and lack of respect, characterizing, also, a representation with negative connotation 24.
Around the CN is the peripheral system, whose function is to protect the core. This system allows the integration of individual experiences, is flexible and sensitive to the immediate context9. The periphery of a social representation is considered to be a bumper between the reality and the CN, which is more resistant to changes25.
In the upper and lower right quadrants, the elements of the first and second peripheries, respectively, are located. The first periphery includes words with high frequency and average order of evocation equal to or greater than three. In the second periphery, the elements were frequently low and evoked later11,16,19. The peripheral system constitutes the "most accessible and liveliest part of the representation"9:38; one of its functions is to prescribe a behavior 9.
In the first periphery, it can be observed that nursing professionals highlighted the terms low self-esteem and fear, signaling a sentimental field where the fear can refer to the fear of the victim of denouncing the aggressor and, because of this, to be target of new and more intense aggressions. It may also reveal the fear of the professionals to suffer reprisals on the part of the aggressors. Fear was also present in the CN of the representation of municipal managers and professionals responsible for women's health from eight municipalities in the state of Rio Grande do Sul. For them, fear can lead the woman to remain in a violent marital relationship by fearing the consequences of a separation1.
I think that violence against women is an abuse, an aggression, it is lack of love. On the part of the woman, it is low self-esteem [...] (N-141)
We talk a lot with them and guide them, but generally they do not want to report, they do nothing, out of fear [...] (N-11)
This feminine passivity illustrated by the term fear can reveal a mixture of feelings that the victim feeds towards the aggressor. These acts may lead women to subordination and consequent victimization, may take on forms of bodily emotions such as shame, shyness, and guilt; or of passions and feelings, such as love, admiration and respect for the aggressor 26.
The contextualization of the term fear in the speeches of the professionals also expresses that they fear to suffer reprisals from the aggressors, thus limiting their action. This situation was also found in another study1, where fear and the feeling of powerlessness reflect male domination. Fear paralyzes them and restricts their intervention to physical damage22,27.
I know cases of colleagues, of having their cars scratched outside, because they denounced it. I think it was done with a nail, some tool, something [...] She parked the car in front of the station and then it came up with all the surface ruined as pushed to the inside. The impression we had is that they took a tool and stuck it in the metal surface and ripped it like a sardine can. This colleague was very scared [...] (N-94)
It's that thing, you're afraid to get involved, to guide, because we know it happens once, and it's gone. The couple fights, and then returns the next day to normal. When you see, you are bothering the husband because you gave guidance to the woman. It is wrong, a lot of things we hide, a lot things we listen we keep to ourselves, but we are also afraid to expose ourselves because we know that suddenly something can happen [...] In other units that I worked you had to see and be quiet, because otherwise, when you left, you would get shot in the face [...] Sadly, there are things that you see and pretend you saw nothing, to avoid exposing yourself [ ...] (NT-95)
The word fear was also included in the CN of the representation on violence against rural women. In this context, fear was associated with aspects based on gender and the subaltern position of the woman. It also revealed the feeling of impotence of the professionals before the aggressors1.
In the second periphery, the word acceptance may be related to both the professional and the victim. This acceptance can result from the naturalization of the violence, which is part of the routine of domestic life. It is as if gender violence were constitutive of marital and socially acceptable relations1.
With so much bureaucracy, in the end the patient ends up resting, accepting the situation [...] (NT-145)
It seems that when women enter into a marital relationship, women give their companions body, soul and identity, they lose their autonomy and the right to decide28, showing submissive to them. The word submission reinforces the fact that women blame themselves for the violence suffered, as well as deem it as natural1.
The culture of the community I serve is quite different. They do not report. But we note that men have that culture of the patriarch [...] men consider themselves superior to women who end up becoming more submissive. But as soon as they came and told us..., we had no case of aggression that we had to report or tell the woman to come and talk to us, no. (N-141)
Gender violence, most of the times, is naturalized by common sense, and accepted as part of the daily life of health professionals and this can interfere in the care given to women in this situation7. In certain situations, the professionals themselves encourage female passivity in the face of male dominance, emphasizing that they should have patience and avoid openly resisting the situation 22. This situation may arise from the socially constructed male and female roles that induce the naturalization of the DVAW. In this sense, when the feminine thinking and its perceptions meet the ideals of a patriarchal, chauvinist society, "their acts of knowledge are, inevitably, acts of recognition, submission"28:22.
I talked to the patient a good deal. [...] I felt a little incapacitated. I was unable to guide her, to make her understand that she had to come back... that her children were waiting for her and that they would be very happy if she came back to them. I felt incapable. (NT-6).
This form of social thinking, of nurses and nursing technicians, can partially explain the professionals' behavior towards DVAW. Avoiding to openly resist the situation represents a behavior that can lead to the perpetuation of violence, because although discouraging the confrontation, there is the feeling that they have done something for the victim. Such professional conduct can be an incentive for submission and impunity. In this sense, the term impunity may refer both to the cases in which the victim does not denounce and to the underestimation of the criminal nature of the act of the aggressors by the withdrawal of the complaint. Many of the women give up the denunciation before the judge, losing this way the opportunity to point the guilt of the aggressor 29. The shame of being a victim of gender violence is also an impediment to denunciation, especially among women with higher schooling and income30.
I think it is a gross impunity that happens, that we experience. (NT-194)
The words located in the lower left quadrant, abuse, power abuse, physical aggression and sadness, constitute the contrasting elements of the representation 11,16,19. They cover terms that were evoked by a few participants, but in the first evocations, which shows the greater importance that the group gives them. Such terms may "reveal elements that reinforce the notions present in the first periphery or the existence of a minority subgroup bearing a different representation" 17: 582. They can also complement and discuss the CN31.
In this study the presence of a subgroup with differentiated representation was not detected among the professionals investigated. Thus, the contrast zone may be complementing or even reinforcing the central nucleus. In this sense, the concept and the image, expressed in the CN by the term aggression, are reinforced by physical aggression, present in the contrast zone. The attitudinal dimension in the CN is composed of the words cowardice and lack of respect, and reinforced by abuse and power abuse in the contrast zone. It can also be inferred that the feeling expressed in the CN by the term revolt is complemented by sadness in the contrast zone.
CONCLUSION
The analysis of the probable elements that integrate the CN made it possible to perceive that the representation of domestic violence against women in the view of nursing professionals presents a negative connotation. It is a structured representation, because violence was represented with terms that expressed concept, image and attitude. It was observed in the speeches that nursing professionals distinguished the forms of domestic violence against the woman, not restricting it to the conceptualization of physical aggression.
The peripheral elements, more related to the reality experienced by the investigated subjects, reveal that, in addition to the feelings that gender violence triggers, providing support for the victims is part of the routine of some of the nursing professionals. The content of the interviews revealed that the fear of reprisals limits the performance of the professionals, as well as prevent the exposure of the reality of violence against women, as the victims do not denounce their aggressors out of fear.
Acceptance may negatively interfere with the care given to the victims, as well as influence intervention strategies and combat violence. The apprehension of the social representations of nursing technicians and nurses can contribute to the fomentation of discussions about domestic violence against women with professionals involved in the care of the victims, as well as facilitate the design of strategies to combat and prevent violence.
It is recognized that one of the limitations of the study was the reduced number of nursing professionals, which made it impossible to compare the representations of nursing technicians with those of nurses. Furthermore, the reduced scientific production on SR of nursing professionals working in FHUs about the DVAW made it difficult to expand the discussions.
REFERENCES
1.Costa MC , Lopes MJM, Soares JSF. Representações sociais da violência contra mulheres rurais: desvelando sentidos em múltiplos olhares. Rev esc enferm USP. 2014; 48(2):214-22.
2.Guedes RN, Fonseca RMGS. A autonomia como necessidade estruturante para o enfrentamento da violência de gênero. Rev esc enferm USP. 2011, 45(esp. 2):1731-5.
3.Organização Mundial da Saúde. Preventing intimate partner and sexual violence against women: taking action and generating evidence. New York (USA):World Hearth Organization, 2010.
4.Almeida LR , Silva ATMC , Machado LDS. Jogos para capacitação de profissionais de saúde na atenção à violência de gênero. Rev Bras Educ Médica. 2013; 37 (1): 110 – 9.
5.Silva EB da, Padoin SMM, Vianna LAC. Violência contra a mulher: limites e potencialidades da prática assistencial. Acta Paul Enferm. 2013; 26(6):608-13.
6.Gonzáles GC, Bejarano CR. La violencia de género: evolución, impacto y claves para su abordaje. Enfermería Global. 2014;(33): 424-39.
7.Leal SMC, Lopes MJM, Gaspar MFM. Social representations of violence against women in the nursing perspective. Interface-Comunic Saude,Educ. 2011; 15(37):409-24.
8.Silva CD, Gomes VLO, Oliveira DC , Marques SC, Fonseca AD , Martins SR. Social representation of domestic violence against women among nursing technicians and community agents. Rev esc enferm USP . 2015; 49: 22-9.
9.Abric JC. Abordagem estrutural das representações sociais: desenvolvimentos recentes. In: Campos PHF, Loureiro MCS, Organizadores. Representações sociais e práticas educativas. Goiânia (GO): Ed. da UCG. 2003. p. 37-57.
10.Moscovici S. Representações sociais: investigações em psicologia social. Traduzido do inglês por Pedrinho A. Guareschi.3ª.ed. Petrópolis, Editora Vozes;2005.
11.Sá CP Núcleo central das representações sociais. Petrópolis (RJ): Vozes; 2002.
12.Sá CP. A identificação dos fenômenos de representação social. Rio de Janeiro: EdUERJ; 1998.
13. Spink MJP. O conhecimento no cotidiano: as representações sociais na perspectiva da psicologia social. São Paulo: Editora brasiliense; 2004.
14.Magalhães EMM, Maia H. O trabalho docente por professores de Curso de Pedagogia. Revista Múltiplas Leituras. 2009. 2(1): 189-206.
15.Arruda A. Teoria das representações Sociais e teorias de gênero. Cadernos de Pesquisa. 2002. 117: 127-47.
16.Abric JC. A abordagem estrutural das representações sociais. In: Moreira ASP, Oliveira DC. Estudos interdisciplinares em representação social. Goiânia (GO): AB Editora; 2000.p.27-38.
17.Oliveira DC, Marques S, Gomes AMT. Análise das evocações livres: uma técnica de análise estrutural das representações sociais. In: Moreira ASP, Camargo BV, Jesuíno JC, Nóbrega SM; organizadores.Perspectivas teórico-metodológicas em representações sociais. João Pessoa (PB): Ed. Universitária; 2005.
18.Bardin L. Análise de conteúdo. São Paulo: Edições 70; 2011.
19.Machado LB, Aniceto RA. Núcleo central e periferia das representações sociais de ciclos de aprendizagem entre professores. Ensaio: aval pol públ Educ. 2010; 18(67): 345-64.
20.Moscovici S. A psicanálise, sua imagem e seu público. Traduzido do inglês por Sofia Fuhrmann. Petrópolis (RJ):Editora Vozes;2012.
21.Acosta DF, Gomes VLO, Barlem ELD. Perfil das ocorrências policiais de violência contra a mulher. Acta Paul Enferm. 2013;26(6):547-53.
22.Kind L, Orsini MLP, Nepomuceno V, Gonçalves L, Souza GA de, Ferreira MFF. Subnotificação e (in)visibilidade da violência contra mulheres na atenção primária à saúde. Cad Saúde Pública. 2013; 29(9):1805-15.
23.Gomes VLO, Silva CD, Oliveira DC, Acosta DF, Amarijo CL. Violência doméstica contra a mulher: representações de profissionais de saúde. Rev Latino-Am Enfermagem. 2015;23(4):718-24.
24. Silva CD, Gomes VLO, Oliveira DC, Amarijo CL, Acosta DF, Mota MS. Representação da violência doméstica contra mulheres entre profissionais de saúde: idade como atributo de diferenciação. Rev enferm UERJ, 2016; 24(3):e13212.
25.Flament C. Estrutura e dinâmica das representações sociais. In: Odelet D, organizadora. Representações sociais. Rio de Janeiro: EdUERJ; 2001.
26.Bourdieu P. A dominação masculina. 12ª ed. Rio de Janeiro: Bertrand Brasil;2014.
27.Almeida LR , Silva ATMC , Machado LDS. O objeto, a finalidade e os instrumentos do processo de trabalho em saúde na atenção à violência de gênero em um serviço de atenção básica. Interface-Comunic.Saude,Educ. 2014; 18(48): 47-59.
28.Hesler LZ, Costa MC , Resta DG, Colomé ICS. Violência contra as mulheres na perspectiva dos agentes comunitários de saúde. Rev Gaúcha de Enferm. 2013;34(1):180-6.
29.Souza MC , Mendes GFR, Lima SDLM, Santana JMAMP, Oliveira MBB , Silva JS da. A Convenção Interamericana para Prevenir, Punir e Erradicar a Violência Contra a Mulher [...] Revista Âmbito Jurídico/Caderno Internacional. 2014. [citado em 11 nov 2015]. Disponível em: http://www.ambito-juridico.com.br/site/index.php?n_link=revista_artigos_leitura&artigo_id=7874
30.Data Senado.(Br) Violência doméstica e familiar contra a mulher. Brasília(DF): Secretaria de Transparência;2013.
31.Nascimento KC, Gomes AMT, Erdmann AL. A estrutura representacional do cuidado intensivo para profissionais de unidade de terapia intensiva móvel. Rev esc enferm USP. 2013; 47(1):176-84.