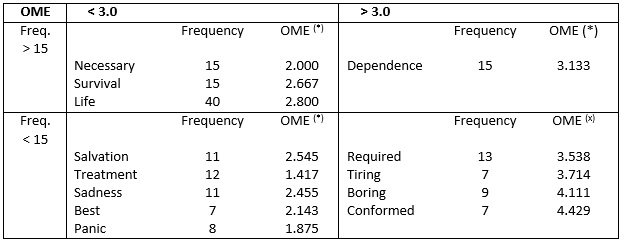
Figure 1: Table of four slots referring to patient evocations for the term hemodialysis inducer, Rio de Janeiro, 2016 (n = 100 subjects, Fmin = 3, Mean Rang = 3.0, Favg = 10)
(*) Average Order of Evocation
ORIGINAL RESEARCH
Social representations of hemodialysis among patients with chronic kidney disease
Felipe Kaezer dos SantosI; Antonio Marcos Tosoli Gomes II; Ricardo de Mattos Russo RafaelIII; Frances Valéria Costa e SilvaIV; Luciana Guimarães AssadV ; Lidiane Passos CunhaVI
I
PhD in Nursing. Professor of the Nursing Fundamentals Department at the
State University of Rio de Janeiro. Rio de Janeiro, RJ, Brazil. E-mail: felipe.santos@uerj.br
II
Post Doctor in Nursing Full Professor at the Medical-Surgical Nursing
Department at the State University of Rio de Janeiro. Rio de Janeiro, RJ,
Brazil. E-mail: mtosoli@gmail.com
III
PhD in Sciences. Professor of the Nursing Department of Public Health at
the State University of Rio de Janeiro. Rio de Janeiro, RJ, Brazil. E-mail:
prof.ricardomattos@gmail.com
IV
PhD student in Collective Health. Professor of the Nursing Fundamentals
Department at the State University of Rio de Janeiro. Rio de Janeiro, RJ,
Brazil. E-mail: francesvcs@gmail.com
V
PhD in Nursing. Professor of the Nursing Fundamentals Department at the
State University of Rio de Janeiro. Rio de Janeiro, RJ, Brazil. E-mail: lgassad@gmail.com
VI
PhD student in Nursing, Department of Medical-Surgical Nursing, Federal
University of Rio de Janeiro. Rio de Janeiro, RJ, Brazil. E-mail:
lidiane_passos_cunha@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2018.23125
ABSTRACT
Objective: to analyze the social representations of patients on hemodialysis in the terminal phase of chronic renal disease. Methodology: the theoretical methodological framework used was Social Representations Theory. The study scenarios were two dialysis centers in Rio de Janeiro, where 100 patients undergoing hemodialysis were included. Data were produced, from October to December 2015, using the free evocation technique, from the stimulus-term "hemodialysis". Results: 434 words were obtained, which were reduced to 173 terms after standardization, and submitted to EVOC software to construct the four-box charts and analyze for similarity. Conclusion: the term most strongly evoked was life, associated with the terms dependence, salvation and survival. Moreover, hemodialysis also prompted images of sadness, panic, tiring, obligation and resigned.
Descriptors: Nursing; nursing care; hemodialysis units hospital; renal dialysis.
INTRODUCTION
The context of a hemodialysis (HD) service is marked by characteristics that are quite peculiar to it, both as regards the need to monitor the performance of a technically complex treatment and the characteristics of the chronic patients, who survive in a condition of dependence for the maintenance of one's life.1
This scenario is the scene of the meeting of two subjects involved in the ongoing performance of renal replacement therapy. At first, nursing professionals (upper and middle level), with the attribution of collaborating with patients' survival and with the progression of their clinical condition.2 In addition to the complexity of this activity, marked by repetition and time pressure, there is also the need to build long-term coexistence with patients in situations of physical and emotional frailty.2
Coexisting in this same scenario are the patients themselves, many of whom deny the disease due to the need for a therapy that brings together pain, uncertainty, a series of short-, medium- and long-term complications and limitations of diverse orders (including social, physical and affective). 3
Although it is in the context of a HD center, professionals and patients have different dimensions and perspectives about this event, which is a substitutive renal therapy for the maintenance of life.4 Moreover, individual differences on both sides are capable of interfering in interpersonal relations by acting on the dynamics of the groups inserted in these spaces, and yet generating conflicts.5
In Brazil, it is estimated that about 100,000 patients have chronic renal disease (CKD) in dialysis treatment.6 These data corroborate the need to deepen the studies that promote the quality nursing care to this part of the population. In addition, attention is drawn to the overvaluation of the technical dimension of care, to the detriment of the relational and interactive aspect observed in the health areas and in nursing.7 Considering that nursing care is, above all, relational in nature, that is, marked by the meeting of the caregiver and the caregiver, this dimension must be valued as a way for the construction of an ethical, plural and capable of transforming human existence for both involved.8
In the area of nephrology, and especially in HD, the use of equipment and specific technical knowledge is very common. This phenomenon sometimes relegates to the background the individualized and welcoming attention that is expected of the nursing team, in order to maintain the health of the body, without losing human dignity.9 This results in the commitment of communication and, consequently, the interaction between professionals and patients, users of HD centers.
With the intention of seeking to know the representations that permeate the experience of the users in HD centers, the present discussion arises, which emerges from a doctoral thesis under construction; being one of the reflections that integrate the study. Thus, the purpose of this article is to analyze the social representations of patients with end-stage CKD about HD.
THEORETICAL REFERENCE
In view of the proposed objective, the Theory of Social Representations (TRS) was chosen to guide the present study.
The TRS is being used more and more widely, since its applicability allows the constructive dialogue with several areas of knowledge. Regarding health, studies carried out with social representations allow the social knowledge that guides the orientation of a population for a given practice. Thus, it allows to highlight the knowledge used by a social group to interpret a given reality and justify the consequent actions.10 Thus, it is expected to give greater emphasis to the structuring of the cognitive contents of the representations, as well as of their transformations from the social practices.11
In this study, TRS will be used through its structural approach, which considers social representation from two interrelated segments: the central nucleus and the peripheral system. The central nucleus is linked to some cognitive elements, the collective memory and the history of the group that constitutes a certain representation. The periphery, otherwise, is characterized by individual stories and experiences, capable of preserving the diversity and contradictions of the group. Peripheral elements more easily undergo context action, and so can become.12
The structural approach is complementary to the TRS and considers that the social representation has a specific characteristic, that is to organize around a central nucleus, being formed by one or more terms that impart meaning to the representation.13
According to the structural approach, the central nucleus will be the element that will least undergo influence of the medium, resisting the change. Therefore, any change of the central nucleus will promote the transformation of representation itself. Thus, it is the central nucleus that characterizes a representation, in such a way that, in order to distinguish two representations from each other, it will be necessary that their nuclei be composed of different elements.13
METHODOLOGY
To obtain the data that would allow to reach the objective of this study, the technique of free evocations will be used. In this stage of data collection, we intend to apprehend the perception of reality from a semantic construction already existing through some objects of representation. This composition includes the use of concrete elements and organized images through simple symbolic elements. The technique used is to ask the subjects to present ideas from the visualization or hearing of inductive terms, that is, words that can stimulate this association.14 The term used in this phase of the research was hemodialysis.
In addition to the free evocations, the data collection instrument contained an initial phase dedicated to the characterization of the subjects of the study, with sociodemographic information, such as: age, sex, marital status, professional training and current labor conditions, religion, HD and if there had been another type of renal replacement therapy prior to HD.
Data were collected between October and December 2015. In total, 100 patients were included in two private dialysis centers in the northern area of Rio de Janeiro. It should be mentioned that all agreed to voluntarily participate in the study, and their consent was registered by means of the free and informed consent term. We did not include individuals with a time to onset of HD less than six months. Also not included were those who proved incapable of performing the mental task of producing the data according to the technique mentioned.
The analysis of the evocations was carried out through the EVOC (Ensemble de Programmes Permettant L´Analyse des Évocations) software, version 2003. Using this resource, it was possible to organize the words produced according to the number of terms (frequency) and the natural order of recall.
By applying said software, we obtain a table of four houses, where the evoked terms are presented, according to the criterion of higher frequencies and medical order of evocation (OME). Thus, for each of the inducing terms used, a corresponding four-box frame was obtained.
The upper left quadrant (central nucleus) presents the words that were evoked more frequently and more immediately, constituting the most consistent part of the representation. It is, so to speak, what gives meaning to the central core of a representation. The lower left frame (contrast zone) contains the words that presented lower frequencies and were, however, more readily evoked. They are terms that can demonstrate variation of the centrality of representation to some more specific groups within a larger group.
The quadrants to the right of the table include words that present late evocations, but with higher (upper) or lower (lower) frequencies. They are called respectively the first and second periphery. The peripheral zone expresses the elements associated with the common elements of life, the daily life of social practices. They are unstable elements and allow individual variation of representation.15,16
From the terms that compose the quadrant for the term evoked, it is possible to perform similarity analysis, which consists of the elaboration of graphical structures with cognitive mapping function. This type of analysis allows to identify the simultaneous occurrences between words and their result expresses the connectivity between them, aiding in the identification of the representation structure. Thus, it is possible to know the binding force between the terms evoked and, therefore, to increase the understanding about the object of study.17
It is noteworthy that the study followed all the ethical precepts, being approved by the Research Ethics Committee under the opinion number: CEP/UERJ 1.393.230.
RESULTS AND DISCUSSION
Among the study participants, the majority were female (56%), with a predominant age group above 60 years of age (41%). There was a predominance of people living alone (single, widowed, divorced - 60%), and retirees (65%). Concerning religion, most of the patients declared themselves Catholic (57%); and among all participants, the majority (83%) reported performing PD as replacement renal therapy of the first choice. For the group included in the study, the mean diagnosis time was 8.1 years; and mean time to onset of HD of 5.5 years.
The sample of the population selected for the study reflects, in fact, the reality of the dialysis centers of Brazil, where despite the distribution with little distinction between the sexes, there is predominance of age from the 60 years of age, that is, with elderly patients.18 The process of aging of the population is one of the factors that has been increasing the number of patients in HD. However, the important growth of patients with CKD in the dialysis phase is also due to the high incidence of chronic diseases (mainly arterial hypertension and diabetes melitus) and comorbid conditions associated with inadequate lifestyle (obesity, sedentary lifestyle, smoking and alcoholism).19
An expressive quantitative study of patients with HD is the first-choice method, that is, they did not undergo peritoneal dialysis from the terminal phase of CKD, which is also observed in the national context.18 Among the participants of the study, an average interval of almost three years between the diagnosis of CKD and the beginning of HD were identified.
It was decided to analyze the representations of this therapy in order to reveal its meaning for these individuals, since we believe that the meaning of HD can interfere in the relationships and in the way the individual behaves in their own universe, considering that it is in this context that the patient deepens the reflection about the questions regarding his daily life, his attitudes, feelings and perspectives regarding his life. 20
During the recall phase, 434 words were obtained for the term inductor hemodialysis. Then, these words were organized for the analysis step, which consists in performing the standardization of a dictionary from the terms evoked, disregarding the repetitions and, finally, we obtained 173 words. Only then the corpus obtained with the set of evocations was submitted to the EVOC software, which presents the simple occurrence frequency of each term, weighted average and the average orders. To follow up the analysis, the cut-off point (minimum frequency) was calculated and the mean frequency and mean recall order (OME) were calculated. The OME corresponds to the average position of each word in the corpus under study.21
Figure 1:
Table of four slots referring to patient evocations for the term
hemodialysis inducer, Rio de Janeiro, 2016 (n = 100 subjects, Fmin = 3,
Mean Rang = 3.0, Favg = 10)
(*)
Average Order of Evocation
The central nucleus, identified in the upper left frame, presents three words, revealing the idea of the need for HD to maintain life (survival, survival, life). Highlight for the term life, with absolute frequency almost three times higher than that of the other terms. In addition, life also has the largest OME (2,800). The survival of the individual affected by end-stage CKD is the performance of renal function replacement therapy, such as HD, a condition without which it would be impossible to remain alive.22,23
The contrast zone (lower left quadrant) is composed of five terms. The first one (salvation) reinforces the idea of the central nucleus, namely that HD is linked to survival, or otherwise, to prolonging life. It is also the term with the highest OME (2,545). A term (treatment) seems to be related to the technical dimension of the therapy, considering that HD is a recommended therapy for a given pathological condition. Then we have the expression of two feelings involved with the realization of HD, both of which carry in themselves a noxious conception (sadness and panic). These feelings sometimes arise with the first signs and symptoms of the pathology, together with the onset of bodily changes, i.e. the first contact with the reality of the manifestation of the disease.14
Finally, the contrast zone presents what seems to us a compensatory strategy, starting from a single (better) term, which creates the sensation that there were situations even more undesirable than the HD itself and that, for this reason, it would be easier to accept the beginning of this therapy. This term includes evocations such as: life-enhancement; to-the-people-to-improve; improvement-quality-of-life; better-than-peritoneal; best-solution; me-feel-better-doing-hd.
The first periphery (right upper quadrant) reinforces the ideas contained in the central nucleus, expressing in its single term (dependence) the notion of subjecting survival to therapy, in such a way that life is conditioned to HD.
The second periphery (lower right quadrant) expresses some of the wear conditions associated with HD, due to its continuous and endless characteristic (tiring and boring). The conditioning of one's life to the performance of therapy is reinforced here by means of a taxation term (obligation). Finally, due to the evoked conditions, the larger OME term of this quadrant (4,429) expresses the condition of submission to HD (conformed). It should be noted that this term does not translate into acceptance, expressing resignation in the face of an inevitable and necessary condition.
As mentioned, similarity analysis was also performed from the terms contained in the table of four houses for evocations of the term inductor hemodialysis. The figure below presents these words, as well as the binding force between them, expressed by means of a numerical index.
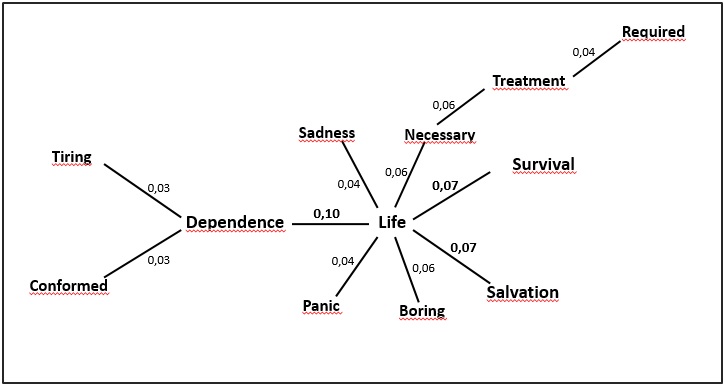
Figure 2:
Patient recall for the hemodialysis inducer term, Rio de Janeiro, 2016 (n =
100 subjects, Fmin = 3, Mean Rang = 3.0, Favg = 10).
The main axis of the previous similarity analysis is represented by the nexus between the words dependence and life (0.10). This representation comes from the fact that, for the patient with terminal CKD, maintenance of life depends on the performance of renal replacement therapy, in this case HD. This notion is reinforced by the following two correlations, according to the decreasing order of significance, both with the same similarity index (0.07): life and salvation, and life and survival. Therefore, it is the connection between the idea that HD represents salvation and survival for those who perform this therapy.
The power of representation about the need for HD for the extension of life is also expressed through the connections between life and necessary (0.06), and necessary and treatment (0.06).
Despite the proven relevance of HD in the sense of providing a continuation of life, the fact that treatment occurs uninterruptedly, in the face of a chronic and therefore incurable disease, has aggregated representations that denote wear and fatigue.24 This is what has been identified through the links between: life and boring (0.06);dependence and tiring (0.03), and treatment and required (0.04).
However, postponing life at the expense of HD can arouse harmful feelings, in the face of a treatment that sometimes causes pain, malaise, physical deformities and that consumes much of the day of the individual, holding back their freedom and autonomy.3 Thus, it was observed that, despite the life being central to the representation of HD, it is linked feelings like sadness and panic, both with 0.04.
Finally, there is the link between dependence and conformed (0.03), a representation that does not translate into acceptance. If an individual's life depends on the achievement of HD and if this fact is a must, one way to accommodate the undesirable is to move toward conformism.
In view of the distribution of the quadrants and similarity analysis for the term hemodialysis, one has the idea of dependence for the maintenance of life strongly expressed. In this sense, therapy emerges as salvation and from dependence, destructive feelings and undesirable conditions, patients turn to conformism.
CONCLUSION
At the conclusion of this study, it was possible to analyze the social representations of patients with end-stage CKD about HD, a proposed goal. Significantly, the association between this renal replacement therapy and the life of the patients who underwent it was significantly enhanced. Through the construction of the quadrant of evocations and similarity analysis, it was found that there is a sense of dependence on HD to survive. HD was also associated with the notion of salvation.
Despite the extreme relevance of treatment to life maintenance, we also observed the association with feelings of sadness and panic, and that HD is a tiring and annoying treatment, given its obligatory characteristic. Finally, in the face of the inevitable, patients are conformed to the realization of the method.
The study had as limitation the difficulty of some patients to perform the abstraction exercise to produce the data through free evocations. Those who were unable to do so independently and clearly were excluded from the study.
Finally among the terms mentioned, there is not the presence of health professionals, including nursing staff, which makes them ask about their relevance to patients with CKD in HD.
REFERENCES
1.Prestes FCP, Beck CLC, Magnago TSBS, Silva RM, Tavares JP. Contexto de trabalho em um serviço de hemodiálise: avaliação dos trabalhadores de enfermagem. Texto & contexto enferm. 2015; 24(3):637-45.
2.Prestes FCP, Beck CLC, Tavaves JP, Silva RM, Cordenuzzi OCP, Burg G, Prochnow A. Percepção dos trabalhadores de enferamgem sobre a dinâmica do trabalho e os pacientes em um serviço de hemodiálise. Texto & contexto enferm. 2011;20(1):25-32.
3.Abreu IS, Santos CB. Qualidade de vida relacionada à saúde de pacientes em hemodiálise. Rev. enferm. UERJ. 2013;21(1):95-100.
4.Ferraz RN, Maciel CG, Borba AKOT, Frazão IS, França VV. Percepção dos profissionais de saúde sobre os fatores para a adesão ao tratamento hemodialítico. Rev. enferm. UERJ. 2017;25(e15505):1-
5.Spagnol CA, Santiago GR, Campos BMO, Badaró MTM, Vieira JS, Silveira APO. Situações de conflito vivenciadas no contexto hospitalar: a visão dos técnicos e auxiliares de enfermagem. Esc. Enferm. USP. 2010;44(3):803-11.
6.Sesso RC, Lopes AA, Thomé FS, Lugon JR, Watanabe Y, Santos DR. Relatório do censo brasileiro de diálise crônica 2012. J. Bras. Nefrol. 2014;36(1):48-53.
7.Gomes AMT, Oliveira DC. A enfermagem entre os avanços tecnológicos e a inter-relação: representação do papel do enfermeiro. Rev. enferm. UERJ. 2008;16(2):156-61.
8.Masson LP, Brito J, Athayde M. Dimensão relacional da atividade de cuidado e condições de trabalho de auxiliares de enfermagem em uma unidade neonatal. Physis Rev. Saúde Coletiva. 2011; 21(3):879-98.
9.Broca PV, Ferreira MA. Equipe de enfermagem e comunicação: contribuições para o cuidado de enfermagem. Rev. bras. enferm. 2012;65(1):97-103.
10.Jacó-Vilela AM, Ferreira AAL, Portugal F. História da Psicologia: rumos e percursos. Rio de Janeiro: Nau Editora; 2007.
11.Sá CP. A Construção do objeto de pesquisa em representações sociais. Rio de Janeiro: Eduerj; 1998.
12.Sá CP. As representações sociais na história recente e na atualidade da psicologia social. In: Jacó-Vilela AM, Ferreira AAL, Portugal FT. História da psicologia: rumos e percursos. Rio de Janeiro: Nau; 2007.
13.Abric JC. Pratiques sociales et représentations. Paris: Presses Universitaires de France; 1994.
14.Oliveira DC, Gomes AMT, Marques SC. Análise das evocações livres: uma técnica de análise estrutural das representações sociais. In: Paredes AS. Perspectivas Teórico-Metodológicas em representações sociais. João Pessoa: Editora Universitária UFPB; 2005 p. 573-603.
15.Abric JC. A abordagem estrutural das representações sociais: desenvolvimentos recentes. In: Campos PHF, Loureiro MCS, organizadores. Representações sociais e práticas educativas. Goiânia (GO): Ed. UCG; 2003 p. 37-57.
16.Oliveira DC, Gomes AMT, Marques SC. Análise estatística de dados textuais na pesquisa das representações sociais: alguns princípios e uma aplicação ao campo da saúde. In: Menin MSS, Shimizu AM, organizadores. Experiência e representação social: questões teóricas e metodológicas. São Paulo: Casa do Psicólogo; 2005 p. 157-200.
17.Moura SRB, Junior MASSM, Rocha AKL, Vieira PPN, Mesquita GV, Brito JNPO. Análise de similitude dos fatores associados à queda de idosos. Rev. Interd. 2015;8(1):167-173.
18.Sociedade Brasileira de Nefrologia. Censo da Sociedade Brasileira de Nefrologia [Internet]. 2015 [citado em 25 mai 2016]. Disponível em http://sbn.org.br/censo-de-dialise-sbn-2015.
19.Braga SFM, Peixoto SVP, Gomes IC, Acúrcio FA, Andrade EIG, Cherchiglia ML. Factors associated with health related quality of life in elderly patients on hemodialysis. Rev. saúde pública (Online). 2011;45(6):1-9.
20.Barbosa GS. Delineando o cuidado de enfermagem a partir da práxis do enfermeiro de hemodiálise: a busca pela proficiência e suas contribuições à oferta do cuidado [dissertação de mestrado]. Rio de Janeiro: Universidade Federal do Rio de Janeiro; 2010.
21.Antunes M, Corso D, Brock F, Fortes VLF, Bettinelli LA, Pomatti DM. Quando uma máquina mantém a vida: o itinerário do idoso renal crônico em hemodiálise. Rev. contexto & saúde. 2011;10(20):1283-86.
22.Oliveira SG, Marques IR. Sentimentos do paciente portador de doença renal crônica sobre a autoimagem. Rev. enferm. UNISA. 2011;12(1):38-42.
23.Rudinick T. Doença renal crônica: vivência do paciente em tratamento de hemodiálise. Contextos clínicos. 2014;7(1):105-16.
24.Souto SGT, Lima GS, Silva PLN, Oliveira RS, Gonçalves RPF. Percepção do portador de insuficiência renal crônica quanto às implicações da terapia hemodialítica no seu cotidiano. Rev. enferm. UERJ. 2017; 25(e8093):1-6.