Figure 1: Table of Four Houses to the inductor term Caring for the person with HIV/AIDS among health professionals from 20 health units. Rio de Janeiro, 2012. (N=148)
ORIGINAL RESEARCH
Social representation by health professionals of care for patients with HIV/AIDS
Antonio Marcos Tosoli GomesI; Priscila Cristina da Silva ThiengoII; Denize Cristina de OliveiraIII; Jeferson RodriguesIV,
I
Nurse. Ph.D. in Nursing from the Federal University of Rio de Janeiro. Full
Professor, State University of Rio de Janeiro. Brazil. E-mail: mtosoli@gmail.com
II
Nurse. Master in Nursing. Assistant Professor, State University of Rio de
Janeiro. Brazil. E-mail: profprithiengo@gmail.com
III
Nurse. Ph.D. in Public Health from the University of São Paulo. Full
Professor, State University of Rio de Janeiro. Brazil. E-mail: dcouerj@gmail.com
IV
Nurse. Ph.D., Professor, Federal University of Santa Catarina. Brazil.
E-mail:
jef_rod@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.22321
ABSTRACT
Objective: to identify the representational structure of health care for patients seropositive for human immunodeficiency virus (HIV/ AIDS) among health professionals, describe that representation using structural and procedural approaches, analyze the representations constructed, and discuss changes in knowledge and practice stemming from those representations. Method: qualitative study guided by Social Representations Theory. The 148 informants were health professionals working in public institutions in Rio de Janeiro. Characterization questionnaires, free evocation and semi-structured interviews were used. Data were analyzed using the four-square format designed by EVOC 2003 software. Results: the most prominent element of the constituents of the central nucleus was love, with a higher frequency of evocation (52) and average order of importance (2,712). Conclusion: the social representation of care among health professionals has love as the central element in its structure and organization. The importance of offering this loving care lies in the humanization of actions, especially in respect for the uniqueness of the unwell person.
Keywords : Social Representation; Health care; HIV; SIDA.
INTRODUCTION
This study shows the results from the dissertation titled The social representation of HIV patient care among health professionals . Also, it integrates the multicenter study called The transformations of health care and nursing in times of AIDS: social representations and memories of nurses and health professionals in Brazil.
The discovery of the Human Immunodeficiency Virus (HIV) in 2013 and the Acquired Immunodeficiency Syndrome (AIDS) completed 33 years. During this period, this infection has become a major public health problem. According to epidemiological data from the Ministry of Health, the epidemic is increasing every year and it is estimated that approximately 734,000 people living with HIV/AIDS in 2014, of which only 842,710 were notified in the SINAN, from 1980 to June 2016.1
Initially, images and understanding about AIDS were linked to homosexual relationships and then to other forms of stigmatization, such as prostitution, promiscuity, sexual drift, and gender differences that largely mark the whole history of the epidemic and to this day it is the most deeply rooted aspect of stigmatization and discrimination related to HIV and AIDS².
Not only human relationships, but science was faced with this new and continuous challenge of living with the syndrome and its representations in the human condition. Thus, it is the challenge of its surprising and unexpected appearance. AIDS has shaken the structures of reliance on the effectiveness of technology and science, as well as the idea of continuous evolution, in which communicable diseases identified as diseases of poverty would actually be overcome. This case becomes even more important when considering that the earliest records of the syndrome were described in the United States of America (USA), considered the symbol of technological evolution and science classified as hard.3
In some settings, stigmatization and discrimination against HIV and AIDS have often been identified and documented in the literature, such as health care. There are descriptions of denial of treatment to patients or those left unattended in a hospital bed, HIV testing without consent, privacy violations and denial of access to hospitals and medicines in different countries and cultures throughout the world. One classic analysis describes HIV/AIDS as an epidemic of meaning in which the use of language is never simply neutral and serves the interests of power in a variety of ways².
Based on the considerations set here, it is necessary for health professionals to be able to carry out a humanized approach to care for people with HIV and AIDS. Thus, the object of this research was delimited in the social representation of health care to the HIV/AIDS patient for the health team. Two guiding questions have guided this study: What are the meanings the health team attributes to the health care provided to people with HIV/AIDS? How can the social representations of care professionals interfere with their knowledge and practice? To respond to these questions, we set out the following objectives: to identify the representational structure of HIV/AIDS patient care among health professionals, to describe their representation through structural and procedural approaches, to analyze constructed representations and to discuss knowledge and practices change from them.
Knowing the social representations of health care to HIV/AIDS patients for the health team is an imperative to contribute both to the understanding of the relationships and the work process, as well as to enable the analysis of the humanization of care and conditions where the work is registered. It is also worth noting that it can contribute to human relations as a whole, inserting them in the struggle for the eradication of prejudices and behaviors unfavorable to the process of humanization of these patients.
THEORETICAL-METHODOLOGICAL REFERENCE
An exploratory-descriptive research with a quantitative approach was carried out to reach the desired objectives and the guiding questions proposed for this research, based on the structural approach of Social Representation Theory (SRT) in the social psychology field4.
In its structural approach, the SRT emphasizes the structuring of the cognitive contents of representations but also deals with the process of its transformation from social practices5. Social representations are a form of knowledge elaborated and shared by society with a practical vision for the construction of a reality common to a social set6. The structural approach organizes social representation in two systems: the central nucleus, constituted by one or some cognitive elements, linked to the collective memory and the history of the group forming the representation.
The study scenario had 20 health units, in which activities based on the National Sexually Transmissible Diseases (STDs), AIDS and Viral Hepatitis Viruses of the Ministry of Health were developed, in a random way, to approach all the program areas of the city of Rio de Janeiro. Among the services in which the study participants worked, the Specialized Attention Service (SAE) and/or Testing and Counseling Center (CTA) stand out.
The participants were 148 health professionals (physicians, nurses, pharmacists, social workers, psychologists, technicians/nursing assistants, nutritionists, and biologists) who answered the socio-professional questionnaire and the free evocations of the inductor term Caring for the person with HIV/AIDS.
During the collection of the evocations, the professionals were asked to speak the first five words that came to their mind when they heard the term inductor. The data of the socio-professional questionnaire were organized with the help of the SPSS software and analyzed with the help of descriptive statistics. For the analysis of the evocations, the four houses of the EVOC 2005 software was used, trying to identify the structuring of the representational contents.
Participation in the research was voluntary based on the free and spontaneous acceptance of its objectives and methodological design, and signing the Informed Consent Term. The meetings were held in the workplace and the data collection took place in the municipality of Rio de Janeiro, from August 2011 to July 2012. The project was approved by the Research Ethics Committee (CEP) of the Municipal Health and Civil Defense (SMSDC-RJ) under number 38A/2011. The research respected the ethical-legal procedures that constituted the fulfillment and use of the ethical values established by Resolution 196/96 of the Ministry of Health7.
RESULTS AND DISCUSSION
The participants were mostly female (79.72%), with ages varying between 45 and 54 years old (18.91%), living with a partner (52.70%), Catholics (45.27%), with a specialization (45.94%), reported that the main sources of information on HIV were by sites in general, technical manuals of the Ministry of Health, professional daily conversations and television (45 %, 33%, and 17%, respectively).
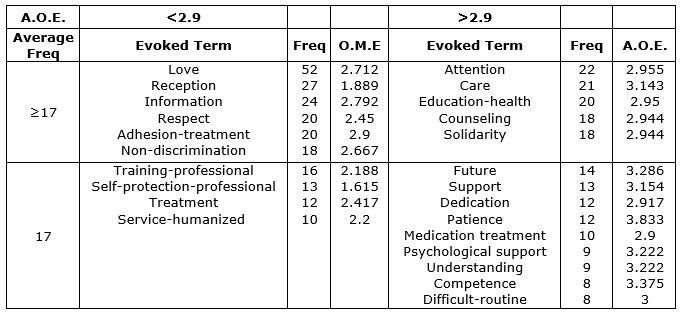
From the application of the Free Evocations technique, there were 695 words evoked, where 150 were different. Based on the Zpif Law of word distribution8, a minimum frequency of 8 was chosen and the words evoked in a smaller number than the one by the subjects were excluded from the composition of the Table of Four Houses. After defining the minimum frequency, the mean frequency was calculated, resulting in 17. The Average Order of Evocation (OME) was 2.9.
From the construction of the analysis, it was perceived the way in which health professionals represent the care provided to the HIV-positive person, presenting, as outstanding characteristics, the affection dimension, characterized by the expression of the feeling of love, knowledge and the practice of care, as well as social memories about HIV/AIDS. It is important to establish the organization of its contents to explicit the content present in this representation so the social thought about care can be understood. See Figure 1.
Figure 1: Table of Four Houses to the inductor term Caring for the person with HIV/AIDS among health professionals from 20 health units. Rio de Janeiro, 2012. (N=148)
According to Central Core Theory,4-9 the elements located in the upper left quadrant of the Four-House Table characterize the possible central core of the representation, since they were often more evoked and more readily evoked. However, it should be noted that not all the components of this house are necessarily central, while elements in other quadrants can be characterized as such in certain situations 4,8,10, but the central nucleus lies in this quadrant.
Thus, in the upper left quadrant there are the words more readily evoked and with higher frequencies of evocation: love, reception, information, respect, adherence-treatment and non-discrimination, indicating a dimension at the same time related to affective aspects as love and care, as to the practical and functional aspects of care such as information, respect, adherence-treatment and non-discrimination.
The elements of the central nucleus can be classified into two types:
functional and normative. The functional types are associated with the
descriptive characteristics and the inscription of the object in social or
operative practices, determining the behavior before the object.
The normative types are directly originated from the value system of
individuals, consisting of a fundamentally social dimension of the core 11. It is worth mentioning the presence of some words with
normative characteristics, linked to the value system of the group studied,
love, acceptance, respect, and non-discrimination, which allows the central
nucleus to exercise its dual role, evaluative and pragmatic11.
At the same time, as regards the functional character, it privileges the
most important elements for the accomplishment and justification of a task,
that is, elements linked to an action, in this case, information and
adherence-treatment.
Considering especially the analysis of each cognition, the most prominent element refers to love, often evocation 52 and a mean order of importance of 2.712, representing the higher frequency of the nucleus. The terms standardized under such denomination were: affection and care.
Even though there is no explicit reference to the disease, people evoke care when there is something that bothers them and worries them. From these concerns and anxieties, there is the expression of their desires and expectations and giving the possibility of apprehending what they indicate as a priority and what touches them the most. The manifestation of commitment to those who want to take care comes from this feeling that was called love12. Loving care and humanization go hand in hand, so as to enable to offer care that meets the human needs of these individuals, respecting their dignity, reducing suffering and facilitating the achievement of their vital project. Therefore, love is concretized in this harmony of care13,14.
The second element to highlight was the reception with the frequency of 27 and average order of evocation of 1,889. The terms standardized under this denomination were: welcome, host, and receiving-well. The presence of this element in the social representation on screen may be related to the approach of the humanization issue in the National STD/AIDS Program. The proposal to host this program follows the guidelines of the Ministry of Health in health production practices15. Then, the reception can be understood as a technology or process built through each meeting as the construction of networks of conversations, humanitarian relationships, and solidarity that potentiate the processes of health production.
Another element standing out was the information, with the frequency of 24 and average order of evocation of 2,792. The terms standardized under such denomination were: clarify; clarifying doubts; clarification; inform, take questions and alert. In the sense of actions aimed at the quality of life of the HIV, the patient is health education, with the purpose of clarifying him about his illness. To that end, the health professional should be able to provide all appropriate information regarding the patient's uncertainties, since it is believed that only from the adequate information the patient will achieve the necessary awareness becoming responsible for his treatment and, in this way, exercising his autonomy8,16,17.
The respect and non-discrimination elements suggest positive attitudes of the professionals towards the care developed with the person living with HIV. The respect had a frequency 20 and average recall order of 2,450, with standardized terms: respect and make-respect-another and the non-discrimination had frequency 18 and average order of recall of 2.667, with standardized terms: non-judgment, without judgment, no-differentiated-look, non-bias without-prejudice, service-without-prejudice, prejudice-deprive, deprive, dogma, destigmatize, demystification, exculpation, win-prejudice, and bias-detachment. The adherence-treatment element is closely linked to the coping of the disease by the person living with HIV and the help of the professional.
This finding reminds us of the past, with the onset of the syndrome and, later, the discovery of its causative agent, with widespread fear among the population in general and especially health professionals, producing repercussions on the care provided. This has often led to discrimination and segregation of individuals living with HIV, explaining the lack of scientific basis for this type of behavior, based largely on the bias. The advancement of information with the new findings of the virus and the ways to control led to profound changes in behavior by the professionals, promoting greater security in procedures and converting discriminatory attitudes as part of the past.
In the lower left quadrant, in the contrast zone, there are the words professional qualification, self-protection-professional, treatment, care-humanized. These elements are part of the so-called contrast zone, which may reveal the existence of a subgroup with a different social representation, whose central nucleus would consist of one or more elements of this quadrant, but may also present as a complement to the first periphery8.11.
Thus, the self-protection-professional and care-humanized elements seem to reinforce a positioning, an attitude towards the care of the seropositive patient by the subjects, present in the central nucleus through the words respect and non-discrimination. The term professional-training reinforces the present meaning of the word information, both in knowledge about the disease itself and in informing patients about it. The word treatment seems to be related to adherence-treatment, constituting a practice of coping with the disease and its complications.
The term self-protection-professional has been singled out in research that addresses the issue of HIV/AIDS. The biological risk is prominent in the hospital environment due to the exposure of several biological agents and this risk increased with the onset of AIDS and the growth of the number of people infected by Hepatitis B and C viruses18. However, it should be noted that, in health services, most accidents are due to non-observance of safety standards, since the use of safe practices and the use of appropriate Personal Protective Equipment (PPE) reduce the risk of an occupational accident. The use of PPE is an essential measure for the safety of the health team and also for patients19.
In the upper right quadrant, the first periphery is the words attention, care, education-health, counseling, and solidarity. The cognitions present in this house include peripheral components considered more relevant 8,11. Thus, attention corroborates with the attitudes of these professionals such as respect and non-discrimination. The words education-health and counseling reinforce the idea of confrontation presented by information and reception, respectively. Solidarity is directly linked to the word love present in the central nucleus, showing affection by the deponents.
Counseling is part of HIV patient care. According to the Ministry of Health 14 it is a dialogue based on a relationship of trust between professional and patient used as an effective strategy in prevention and health promotion in the process of HIV diagnosis. It is composed of educational components (such as clarification of doubts, advice on disease and treatment), risk assessment (dialogue on lifestyle, exposures to risk situations related to sexual practices and drug use, leading to risk and protection possibilities) and emotional support (implying the establishment of a relationship of trust with the user so he feels welcomed and cared for his specific needs).
In the lower right quadrant, there are the terms future, support, dedication, patience, drug treatment, psychological support, understanding, competence, difficult-routine. According to the assumptions of the structural approach, these elements constitute the second periphery of the social representation in question, being infrequent and defined as less important among the evocations enunciated by the deponents of the research 8,11. In this perspective, the words future and difficult-routine express an imaginary dimension, demonstrating a perspective of the social representation of markedly negative care. However, the words support, dedication, patience, and understanding refer to the behaviors of these professionals towards this care, evidencing a connection with the terms respect and non-discrimination. The measures to cope with the disease are confirmed by the terms treatment-drug and psychological-support according to adherence-treatment. And competence is closely adjusted to the word information, demonstrating the knowledge by the professional who cares.
CONCLUSION
In this study, it was found that the social representation of health care to the HIV patient was constructed by the general group, with love as a core element, determining the characteristics of the care provided, and associated with it, there are the constituent elements of this representation. The importance of the care offered by the idea of love lies in its relation to the humanization of care actions that, at the same time, meet the individual's demands and respects their uniqueness as a human being, facilitating their illness and the search for improvement of health.
Therefore, this study evidenced the dynamics of care practices both for oneself and those provided to people with HIV/AIDS oriented by the social representations of the syndrome. It allows understanding, from such representations, how care has been and is being developed, its modifications, and consequently the introduction of positive elements in its constitution. Finally, the social representation of care has a structure related to the interaction sustained by an archeology linked to the considered noble feelings and actions of self-denial and human overcoming. This archeology also maintains a strong social memory about communicable diseases in which punishment, salvation, guilty and victims are called in the conformation of a complex daily life and difficult to cope with. The relationship between the care of the other and self-care was presented as polarities that are shaped as a result of the biomedical, symbolic and human process experienced by professionals in the face of the drama of caring for other human beings who are facing a situation with the intensity and challenges of AIDS.
REFERENCES
1. Ministry of Health (Br). Epidemiological Bulletin AIDS: preliminary version. 2015/2016; 5(1). Brasília (DF): Ministry of Health; 2016. [cited on July 17. 2017]. Available on: http://www.aids.gov.br/data.
2.Parker RG, Aggleton P. Stigma, Discrimination, and AIDS. Rio de Janeiro: Brazilian Interdisciplinary AIDS Association; 2001.
3.Nuland SB. How We Died: Reflections on the Last Chapter of Life. Rio de Janeiro: Rocco; 1995.
4.Sá CP. The Central core of social representations. 2nd ed. Petropolis (RJ): Vozes; 2002.
5.Sá CP. The construction of the research object in social representations. Rio de Janeiro: EdUERJ; 1998.
6.Jodelet D. Social representations: an expanding domain. In: Jodelet D, Organizer. The social representations. Rio de Janeiro: EdUerj; 2001.p.17-44.
7. Ministry of Health (Br). National Council of Health. National Commission on Ethics in Research/CONEP. Regulatory guidelines and norms of research involving human beings. Resolution n.º96/96. Rio de Janeiro: FIOCRUZ; 1998.
8.Oliveira DC, Marques SC, Gomes AMT, Teixeira MCTV. Analysis of free evocations: a technique of structural analysis of social representations. In: Paredes AS. Theoretical-methodological perspectives on social representations. João Pessoa (PB): University Publishing House UFPB; 2005 p.573-603.
9.Abric JC. The structural approach of social representations. In: Moreira ASP, Oliveira DC, organizers. Interdisciplinary studies of social representation. 2nd ed. Goiania (GO): AB Publishing house; 2000. p. 27-38.
10.Abric JC. La recherche du noyau et la zone muette des représentations sociales. In: Abric JC. Méthodes d'études des représentations sociales. Ramonville (Fr): Saint-Agne; 2003. p.60-80.
11.Abric JC. The structural approach to social representations: recent developments. In: Campos PHF; Loureiro MCS Social representations and educational practices. Goiânia (GO): Ed. UCG; 2003. p.37-57.
12. Collière MF. Take care ... the first art of life. 2ª ed. Loures (Pt): Lusodidacta; 2003.
13.Grüdtner DI, Carraro TE, Hilda Sobrinho S, Carvalho ALG, Campregher G. Love in nursing care. Rev enferm UERJ. 2010. 2(18): 317-22. [cited on July 17, 2017]. Available on: http://www.facenf.uerj.br/v18n2/v18n2a25.pdf .
14. Gomes AMT. Love in nursing: an approach from Plato. Rev enferm UERJ. 2015. 23(4): 441-2. [cited on July 17, 2017]. Available on: http://www.facenf.uerj.br/v23n4/v23n4a01.pdf .
15. Ministry of Health (Br). National STD and AIDS Program. Basic care notebooks: HIV/AIDS, Hepatitis, and other STDs. Brasília (DF): Ministry of Health. 2006.
16.Macêdo SM, Miranda KCL, Silveira LC, Gomes AMT. Nursing care in Specialized HIV/Aids Outpatient Services. Rev Bras Enferm [Internet]. 2016. 69(3): 483-8. [cited on July 17, 2017]. Available on: http://www.redalyc.org/html/2670/267046071014/ .
17.De Melo BMG, Pereira VMAO, Góis ARS, Silva CRL, Silva FMA. Social representations of the nursing team before the HIV / AIDS patient: an integrative review. Rev enferm UFPE. 2017. 11(2), 625-33. [cited on July 17, 2017]. Available on: http://www.seer.unirio.br/index.php/cuidadofundamental/article/viewFile/4844/pdf_1726 .
18.Leite JL, Dantas CC, Silva CC, Gonçalves SD. AIDS: twenty-four years of struggle. Enfermería Global. 2006. 9, 1-13. [cited on March 03, 2016]. Available on: www.um.es/eglobal/.
19.Valle ARMC, Feitosa MB, Araújo VMD, Moura MEB, Santos AMR, Monteiro CFS. Social representations of biosafety by nursing professionals of an emergency service. Esc Anna Nery. 2008. 2(12); 304-9. [cited on July 17, 2017]. Available on: http: http://www.scielo.br/pdf/ean/v12n2/v12n2a16.pdf .