* Two subjects in the private system did not answer the question
# Positive residue greater than 1.96 at the analysis
ORIGINAL RESEARCH
Public and private sectors: sociodemographic characteristics of people with tuberculosis, and diagnostic actions
Jessica Oliveira TombergI, Jenifer HärterII, Lílian Moura de LimaIII, Dagoberta Alves VieiraIV, Eduarda Russo-GonçalvesV, Roxana Isabel Cardozo-GonzalesVI
I
Master. Federal University of Pelotas. Nursing school. Pelotas, Rio Grande
do Sul, Brazil. E-mail: jessicatomberg@hotmail.com
II
Master. Professor at the Federal University of Pampa. Unipampa, Rio Grande
do Sul, Brazil. E-mail: jeniferharter@hotmail.com
III
PhD. Professor at the Federal University of Pelotas. Nursing school.
Pelotas, Rio Grande do Sul, Brazil. E-mail: lima.lilian@gmail.com
IV
Master. Federal University of Pelotas. Nursing school. Pelotas, Rio Grande
do Sul, Brazil. E-mail:
daguialvesvieira@hotmail.com
V
Nurse. Federal University of Pelotas. Nursing school. Pelotas, Rio Grande
do Sul, Brazil. E-mail: duda-crag@hotmail.com
VI
PhD. Professor at the Federal University of Pelotas. Nursing school.
Pelotas, Rio Grande do Sul, Brazil. E-mail: roxana_cardozo@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.22155
ABSTRACT
Objective: to examine demand for public or private sector care, by sociodemographic characteristics of tuberculosis patients, and these services' diagnostic actions in response to respiratory symptoms. Method: this quantitative, cross-sectional study of 96 people with tuberculosis in a city of southern Brazil from 2013 to 2014 used structured forms, descriptive analysis and chi-square test. The study was approved by the research ethics committee (No. 310.801) in 2013. Results: the factor accounting for the largest contribution to public sector demand was non-white skin color and, in the private sector, white. Single people sought the public sector, and people with stable relationships sought private care. Less than eight years' schooling related to use of public sector services. Conclusion: the private sector diagnosed the most people. The test most requested was chest X-ray.
Keywords: Tuberculosis; diagnosis; health services; health services evaluation.
INTRODUCTION
After 21 years of the declaration of tuberculosis control as a global public health emergency by the World Health Organization, a number of strategic investments to detect cases and succeed in treatment have been implemented until present. Health indicators show significant reductions in incidence rates, averaging 1.5% per year. Currently, it is estimated that 37 million people have had their lives saved by efficient disease detection and treatment actions1.
In Brazil, the incidence rate of tuberculosis has decreased by 20.4% in the last 10 years, and the mortality rate fell by 45%1 when comparing data from the year 1990 with data from the following two decades. The implementation of the National Tuberculosis Control Program in the Brazilian territory has contributed to the progress of the indicators and also to the guarantee of gratuity, in the public sector, of essential diagnostic exams (sputum smear microscopy and chest radiography) and treatment of the disease.
The characteristics of people affected by tuberculosis have been maintained throughout these years; they are predominantly male and economically active individuals2-4. There is also a population that is closely related to vulnerability factors such as social status (poverty, low level of education), behavioral habits (alcoholism, smoking, and drug addiction), specific populations (indigenous peoples, homeless people, prison inmates), and the presence of comorbidities (HIV/AIDS and diabetes)2-5.
Such profile indicates a direct relationship between social vulnerability and the infection with tuberculosis. In this cycle, there are barriers to diagnosis in the public sector. For example, the diagnosis depends on the individual's perception of the symptoms of the disease and his seeking for health care; the access to health services is difficult; the timely search of individuals with respiratory symptoms for public health services, in special primary health care units, is absent or low.
Care for tuberculosis in the private sector is also a reality; individuals with better economic conditions can make this option for the resolution of their health needs4. This fact has become gradually more frequent in the country6,7. This is incentivized by the characteristics of the fragmented health system in the national context, where services offered are duplicated and supplementary7, that is, both sectors have similar service offer. Access to the private sector can result from the disbursement of classic liberal services directed to autonomous services or from the contracting of private health insurance plans. In December 2013, 49,373,689 people had health plans in the country, which represents a 25.5% health care coverage rate; in December 2014 the rate was 26%, with 50,496,436 beneficiaries8.
Individuals with respiratory symptoms seeking the private sector tend to receive the diagnosis of the disease with more delay, which may be a reflection of low suspicion for the fact that they do not fit the predominant profile of tuberculosis patients; the preference for the use of chest radiography by professionals in this sector; or the low demand of the sick person for these health services, leading the professionals to have little contact with tuberculosis in these spaces9,10. A study found that people with a family income of more than five minimum wages delayed more to seek for health services11, which may indicate a flaw of the health system also among respiratory symptomatic patients with a favorable economic situation.
Research carried out in countries of the African, Asian and American continents points to the deficiency of the public sector in the attention to tuberculosis with regard to the costs of diagnosis and treatment of the disease implied to the affected individuals10. This means that although a person uses public services, he is not free of personal costs in the search for a cure from tuberculosis.
Given the preponderant role of the public health system, the expansion of health plans and their complementary function in the Unified Health System, it is considered relevant to identify the prevalence of the demand for particular services and the directions given to cases of tuberculosis in this sector. Thus, this study aimed to analyze the search for care in the public or private sector, according to the sociodemographic characteristics of tuberculosis patients, and the diagnostic actions of these services in the case of individuals with respiratory symptoms.
LITERATURE REVIEW
The National Tuberculosis Control Program guides actions to combat the disease in Brazil, and is linked to the health service network and articulated with other government programs. The program is administrated by the three government spheres, with the respective levels of competencies and duties, guiding the specificity of the care according to the different Brazilian scenarios2.
Tuberculosis control actions are totally covered by the Unified Health System. They are based on early detection of cases by means of the search for individuals with respiratory symptoms, agility at diagnosis, and start of treatment, ensuring that the patient completes the treatment until reaching the cure. To that end, the facilitation of access of people with respiratory symptoms of tuberculosis to health services, whether public or private, is recommended. These services, regardless of their specialty, are responsible for identifying potential cases of the disease (people who present a cough for three weeks or more), and establishing the adequate flow of these individuals for completion of the diagnosis. The decentralization of detection and treatment actions for primary health care services is strongly recommended2.
Private units and clinics are also important access points to the health network7. In the case of these services, it is suggested that when they receive individuals with respiratory symptoms of tuberculosis, such individuals must be directed to the public network in view of the gratuity of the services, according to the availability of resources. It is optional for the person with respiratory symptoms to remain in the private network. In these cases, the responsible health professionals must communicate with the Municipal Tuberculosis Control Program for the purpose of notification of the follow-up of cases, reports and records necessary for epidemiological surveillance.
The diagnosis of tuberculosis involves the request of two sputum samples for sputum smear examination - the first being at the time of the consultation and the second, in the following day in the morning - and a chest X-ray. It should be noted that every health professional is ready to carry aout such process, which is not an exclusive activity of the medical category. After collection, the material needs to be sent to the laboratory. Thus, municipal management should establish a flow of reference laboratories, guiding and raising awareness among health professionals about this process2.
Compliance of health professionals with the recommendations can potentially and effectively contribute to disease control. Therefore, in order for the actions to be developed, it is necessary to ground them on a structured network of health services, which requires that the municipal administration fulfill its responsibilities and actively participate in the control process of tuberculosis.
METHOD
This is a cross-sectional and quantitative study developed in a large municipality in the Southern Region of Brazil, considered a priority for the control of tuberculosis by the Ministry of Health.
The municipality has a population of 328,275 inhabitants12. In December 2013, there were 53,903 health plan beneficiaries in the city and, in the same month in 2014, this contingent increased to 55,3498. The city's health network has 814 establishments, of which 80 are directly managed by the health sector, four are public foundations under indirect management, 717 are private institutions, two are private foundations and 11 are charitable, non-profit organizations13. In tuberculosis care, the diagnosis and treatment of patients are mainly centralized in the Municipal Tuberculosis Control Program. In 2012, the number of tuberculosis cases was 254, of which 207 were new cases; in 2013, there was a reduction to a total of 222 cases, of which 169 were new cases. As early as 2014, the number of cases was 266, with 197 new cases, corresponding to an incidence of 60 cases per 100,000 inhabitants14.
Data collection was prospective and occurred in the outpatient clinic of the Municipal Tuberculosis Control Program, considering all the 127 people who started treatment for pulmonary tuberculosis from August 2013 to July 2014. The exclusion criteria adopted were: minors, people who could not communicate verbally, people with cognitive deficits, and institutionalized people. At the start of treatment, pulmonary tuberculosis patients who met the criteria for participation in the study were invited by trained interviewers to respond to the structured interview form in a private room.
The study had a convenience sample including all persons (127) undergoing treatment for tuberculosis during the period of data collection. Among these people, three died before they could be interviewed; seven were transferred to other municipalities; two refused to participate in the study; six abandoned treatment and could not be located for the interview during data collection; and 13 were considered as losses. The final sample totaled 96 participants.
The structured form had questions directly addressing the use of health services and the actions they performed. This data collection instrument was evaluated by researchers in the thematic area of tuberculosis of three universities in the Southern Region of Brazil, and a pilot test was carried out in a priority municipality for tuberculosis in the State of Santa Catarina. The variables gender, skin color (white, black, brown and others), marital status (single, married/common-law married, and separated/divorced/widowed), and schooling (greater or equal to eight years, or more than eight years) were used to know the profile of the subjects interviewed. The presence of comorbidities, the grant of benefits from the State, and the consumption of illicit drugs, alcohol and tobacco were also evaluated.
The first service sought by people diagnosed with tuberculosis was identified by means of an open question (which was the first health service that you sought when you perceived the symptoms?), and the mentioned services were later stratified into public and private, according to lists of public services in the municipality and partner services.
The analysis of the data was developed with the Statistica 12 software by StatSoft. The Chi-square test with residue analysis was applied to verify the association between the variable first service sought, identifying it as either public or private, and the variables related to the characteristics of the subjects, and to the conduct of the health services.
All subjects interviewed agreed to participate in the study by signing the Informed Consent Term. The research project was approved by the Research Ethics Committee, under Opinion 310,801 in 2013.
RESULTS AND DISCUSSION
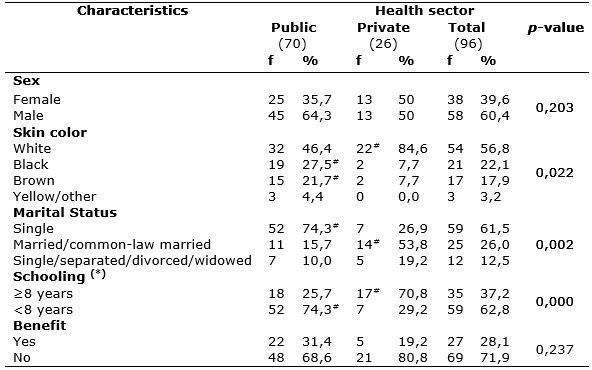
A total of 96 people with pulmonary tuberculosis were interviewed; 70 (73%) had received the first care in public health services and 26 (27%) in private services. The sample was predominantly composed of male patients - 58 (60.4%), and 45 (64.3%) of the interviewees had sought for public services. The most frequent skin color was white, 54 (56.8%), with a noteworthy concentration of white people among the group that used private services, 22 (84.6%), as shown in Table 1.
People who sought the public sector had a mean age of 38.27 years (SD = 15.05) and the average family income reached R$ 1,009.78 (SD = 747.92). Among the people that had received care in the private sector, the mean age was 44.88 years (SD = 17.11) and the average family income was R$ 2,625.38 (SD = 2,391.50).
TABLE 1:
Sociodemographic characteristics of people with pulmonary tuberculosis,
stratified according to the health sector sought for first care. Rio Grande
do Sul-Brazil, 2017.
* Two subjects in the private system did not answer the question
#
Positive residue greater than 1.96 at the analysis
The actions of diagnosis and treatment of tuberculosis are offered by the Unified Health System, free of charge, aiming at universal access. The supplementary and duplicate characteristic of the Brazilian health system allows the population to have a wide range of services, whether public or private, available to meet their health needs.
The results regarding family income were already expected; families with a favorable financial situation had greater access to the private sector, while families living in unfavorable financial situations used the public health sector as the only option for the care of their health needs. It is known that the low income of people affected by tuberculosis, already evidenced in previous studies, acts as a triggering factor for the delay of the diagnosis6,11.
Furthermore, the social context of inequality in the country associated with the illness of tuberculosis establishes a relationship with a cascade effect in which the poverty and the living conditions of the population, configured as a situation of vulnerability, put people at greater risk of infection, and tuberculosis accentuates the vulnerability. Such inequality is also perceived when people with black or brown skin color are far less represented in the private sector care, suggesting that the skin color determines their social situation4.
The public sector is responsible for the majority of the consultations among individuals with respiratory symptoms of tuberculosis. Generally, the individuals themselves seek this health service4,15,16. The financial issue is among the factors that motivate the search for care in the public sector. Individuals do not directly pay for assistance. The service is indirectly financed by the taxes paid by the population to the Government. On the other hand, the choice of respiratory TB patients for care in the private sector is related to the affinity, reliability, and feeling of security provided by such service, since the private sector allows the users to choose the health insurance and/or the professional they want to use and see, something that is often not possible in the public sector. Moreover, the expanded provision of services that eliminates the dependence on a single access route can promote the perception of assurance of coverage of the health needs.
Thus, the two sectors act as possibilities for the diagnosis of tuberculosis. However, after the diagnosis, communication between both sectors is strictly necessary to start treatment. It is the responsibility of the Ministry of Health, through Epidemiological Surveillance, to manage the information on diagnosed and treated cases of tuberculosis. In this sense, institutions of the private sector that assist sick people need to communicate the cases of the disease to the Epidemiological Surveillance, so that notification/investigation forms can be filled out.
It should be noted that the public sector faces problems in filling in such forms17 due to communication failures. This failure ultimately causes underreporting and errors in cure or treatment abandonment rates. In addition, services providing care for tuberculosis and producing data for the National Disease Notification System show a distancing from actual health indicators, making it difficult to plan evidence-based actions in the public sector18. The situation is even worse in the private sector, which sometimes keeps distant from the reality of the local health system, assuming only punctual actions focused on the practice of clinical diagnosis. Thus, the flow of patient care is usually characterized by the transfer of responsibility, after diagnosis, to the public sector, which assumes case management and investigation of contacts.
Regarding marital status, the majority of the sample - 59 (61.5%) was single, with a predominance of 52 (74.3%) among those who sought out for the public health service. As for schooling, 59 (62.8%) of the interviewees had less than eight years of schooling. The predominance of this group is also observed among those who searched for public services, 52 (74.3%), as opposed to the observed among those who sought the private sector, who were clients with eight or more years of study - 17 (70.8%).
It should be noted that regarding certain variables - skin color, marital status and schooling, a p-value < 0.05 was obtained, which indicates a statistical significance of the differences between the two types of health sectors sought.
A study pointed out to the low level of education among people assisted by the public sector as a barrier to the detection, diagnosis and initiation of treatment of the disease19. The success of these actions is conditioned to the set of activities developed by professionals and to the participation and acceptance of the patients.
In a research carried out in the municipalities of Foz do Iguaçu 15 and São José do Rio Preto11, there was also the predominance of single individuals affected by tuberculosis, and these had an additional significant delay to search for the first care measures. This peculiar feature may be associated with lack of family support and/or a strengthened support network.
The results of the distribution of the characteristics of use of illicit drugs, alcohol and tobacco, and the presence of comorbidities among the interviewees are shown in Table 2. It is noteworthy that in the studied sample, there was no statistically significant difference in these characteristics. Regarding the distribution of the interviewees per health sector, there was a higher relative frequency of comorbidities among those who sought the private sector, and tobacco consumption was more frequent primarily in the group that sought public health services.
TABLE 2:
Characteristics of comorbidities and use of drugs and tobacco among people
with pulmonary tuberculosis, stratified per health sector sought for first
care measures. Rio Grande do Sul-Brazil, 2017.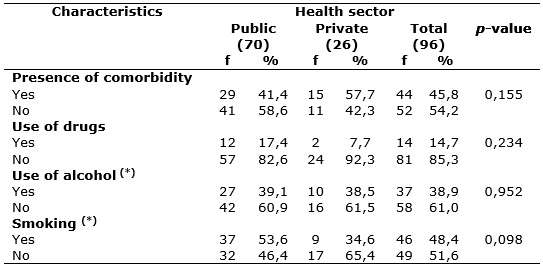
* One subject who sought the public system did not answer this question and
was therefore excluded from the analysis.
It is understood that care in the different health sectors should consider the individual characteristics and specific problems of each patient. Regardless of the sector sought, tuberculosis infection has similar characteristics in the population as a whole.
However, it is known that certain population groups are not prioritized for attention to tuberculosis3, such as people affected by comorbidities, those who use alcohol and drugs, smokers and financially disadvantaged people. Although the results showed that the majority of people with tuberculosis is not included in these groups, it is understood that they are more susceptible to the severe forms of the disease, which would demand specific and directed attention.
The municipality under study structures the attention to tuberculosis around a public reference service. In turn, this favors the discontinuity of actions. This situation promotes unnecessary referrals to the abovementioned center. The failure to resolve the health problem in the first service sought by the person with tuberculosis leads to delayed diagnosis and initiation of treatment.
This logic of organization of attention to tuberculosis stimulates the lack of commitment and the resistance of health professionals, and of the city's health care network, to implement practices to decentralize the actions. The valorization of compliance with normative protocols, the performance of exams, procedures and inputs are considered essential for the diagnosis of the disease20.
Regarding the realization of diagnoses, the highest relative frequency (60.9%) was observed among individuals who sought the private sector. The diagnostic test used was predominantly chest X-rays in the two health sectors, whereas sputum smear microscopy was not required in more than half of the studied population. It should be emphasized that the behavior of professionals of the two health sectors was not statistically different, according to Table 3.
TABLE 3:
Distribution of the conduct of health professionals according to the health
sector sought for first measures. Rio Grande do Sul-Brazil, 2017
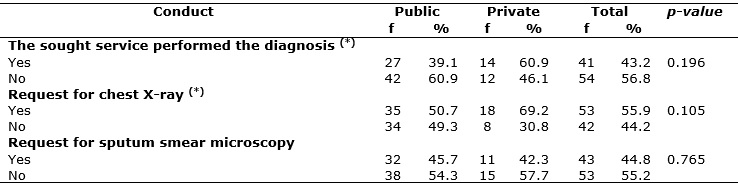
*One subject who sought the public sector did not answer this question and
was therefore excluded from the analysis.
It should be noted that the lack of structure of public services, in terms of availability of sputum pots, forms, collection site, and sample delivery flow in the health network may influence the decision of professionals for not requesting sputum smear microscopy, but rather directly send the patient with respiratory symptoms to perform a chest x-ray in a diagnostic support service. This occurs mainly in the primary health care, which is usually the place of choice for the first care measures6,15,16.
A devaluation of sputum smear microscopy was confirmed in this study, as already mentioned in a previous study16. Both the private and the public sector do not assume tuberculosis as the first diagnostic hypothesis, and the use of radiography makes it possible to investigate a wider range of diagnostic hypotheses, whereas smear microscopy is a specific and targeted test for tuberculosis.
The higher prevalence of diagnostic action in the private health service can be linked to the rapid access to the tests and the agility in obtaining the results. In this sense, the dynamics of the private sector can present a differentiated interaction with its users as a result of the mercantilist logic of buying and selling services. Furthermore, the subject's motivation for rapid diagnosis may influence this aspect, as well as the higher schooling, observed in this study.
CONCLUSION
The greatest search for the public health sector is consistent with what is advocated by the national management program of the disease. However, the use of private services in the context studies was relevant, calling attention for investments in the complementarity and consolidation of an effective communication system between both sectors in the attention to tuberculosis, in order to allow the monitoring and evaluation of the actions so as to guarantee the continuity and agility in the diagnosis and treatment of the disease.
The characteristics associated with the private and public service groups mark the persistence of inequalities in the use of health sectors in terms of skin color, schooling and marital status. It is urgent to increase the diagnostic potential in both sectors, especially in the public services, given the regulatory role of the system, which is responsible for population health. The valuation of sputum collection, whether for sputum smear or molecular testing, should take the status of routine procedure in the practice of the health services, as advised in the recommendations of attention to tuberculosis.
The limitations of the study are related to the reduced sample, although all subjects undergoing treatment were considered. We suggest to expand the approach to other contexts. However, this should be done with caution, considering scenarios that present characteristics such as those cited at the study site, mainly related to the centrality of care in the follow-up of the disease. Also, there is a scarcity of investigations in the private sector focusing on the diagnosis of tuberculosis. Therefore, studies to deepen the theme of the use of private services, as well as the monitoring of patients with respiratory symptoms and tuberculosis cases are recommended, in order to identify the potential interfaces of these sectors in the control of tuberculosis.
REFERENCES
1. World Health Organization WHO. Global tuberculosis report 2013. Geneva (Sw); 2013. [cited on March 12, 2016]. Available from: http://apps.who.int/iris/bitstream/10665/91355/1/9789241564656_eng.pdf?ua=1
2.Ministry of Health (Br). Recommendations manual for tuberculosis control in Brazil. Secretariat of Health Surveillance, Department of Epidemiological Surveillance. Brasília (DF): MS Publisher; 2011.
3.Dantas DNA, Enders BC, Queiroz AAR, Coura AS, Silva MPM, Menezes RMP. Factors associated with the first choice of site for diagnosis of tuberculosis. Rev Gaúcha Enferm. 2014; 35(3):75-81.
4.Trigueiro DRSG, Nogueira JÁ, Monroe AA, Sá LD, Anjos UU, Villa TCS. Individual determinants and use of health services for the diagnosis of tuberculosis. Rev enferm UERJ. 2013; 21(3):371-8.
5.Lacerda SNB, Silva TCD, Araújo PDPCD, Pinto ML, Figueiredo TMRMD. The comorbidity tuberculosis and diabetes mellitus. JNUOL. 2015; 10 (suppl.1): 239-47.
6.Andrade SL, Rodrigues DCS, Barrêto AJR, Oliveira AAV, Santos ARBN, Sá LD. Tuberculosis in the elderly: gateway to the health system and late diagnosis. Rev enferm UERJ. 2016; 24(3):e5702.
7.Santos IS. Evidence on the public-private mix in countries with duplicate coverage: worsening inequities and segmentation in national health systems. Ciênc saúde coletiva. 2011; 16(6):2743-52.
8. National Supplementary Health Agency (BR). Sectorial data and indicators. [Internet] 2016 [cinted on 28 March, 2016]. Available from: http://www.ans.gov.br/perfil-do-setor/dados-e-indicadores-do-setor#sthash.ewi0rJB0.dpuf
9.Rundi C, Fielding K, Godfrey-Faussett P, Rodrigues LC, Mangtani P. Delays in seeking treatment for symptomatic tuberculosis in Sabah, East Malaysia: factors for patient delay. Int J Tuberc Lung Dis. 2011; 15(9):1231-8.
10.Mauch V, Bonsu F, Gyapong M, Awini E, Suarez P, Marcelino B, et al. Free tuberculosis diagnosis and treatment are not enough: patient cost evidence from three continents. Int J Tuberc Lung Dis. 2013; 17(3):381-7.
11.Wysocki AD, Ponce MAS, Scatolin BE, Andrade RLP, Vendramini SHF, Ruffino-Netto A, et al. Delay in the search for the first care measures for diagnosis of tuberculosis. Rev esc enferm USP. 2013; 47(2):440-7.
12.Brazilian Institute of Geography and Statistics. Estimated population of the city of Pelotas for the year 2010. 2010 [cited on February 11, 2016]. Available from: http://cidades.ibge.gov.br/xtras/perfil.php?lang=&codmun=431440
13. National Registry of Health Establishment (Br). Report of nature in the municipality of Pelotas in 2015. 2015 [cited on March 19, 2016]. Available from: http://cnes.datasus.gov.br/Mod_Ind_Natureza.asp?VEstado=43&VMun=431440
14.National Disease Notification System (BR). Confirmed cases of tuberculosis in the years 2013 and 2014. 2014 [cited on March 19, 2016]. Available from: http://dtr2004.saude.gov.br/sinanweb/tabnet/dh?sinannet/tuberculose/bases/tubercbrnet.def
15.Silva-Sobrinho RA, Andrade RLP, Ponce MAZ, Wysocki AD, Brunello ME, Scatena LM, et al. Delay in the diagnosis of tuberculosis in a municipality in the tri-border Brazil, Paraguay and Argentina. Rev Panam Salud Publica. 2012; 31(6):461-8.
16.Loureiro RB, Scatena-Villa TC, Ruffino-Netto A, Peres RL, Braga JU, Zandonade E, et al. Access to the diagnosis of tuberculosis in health services in the city of Vitória, ES, Brazil. Ciênc saúde coletiva. 2014; 19(4):1233-44.
17.Bartholomay P, Oliveira GP, Pinheiro RS, Vasconcelos AMN. Improving the quality of information on tuberculosis from the relationship between databases. Cad Saúde Pública. 2014; 30(11):2459-69.
18.Silva Júnior SHAS, Mota JC, Silva RS, Campos MR, Schramm JMA. Description of the repeated records in the National Disease Notification System, Brazil, 2008-2009. Epidemiol Serv Saúde. 2016; 25 (3): 487-98.
19.Cavalcante EFO, Silva DMGV. Profile of tuberculosis patient. Rev RENE. 2013;14 (4):720-9.
20. Brito EWG, Silva AKF, Teixeira GGA, Dias GBS, Costa NDL, Uchôa SAC. Care organization for tuberculosis in the primary care of Rio Grande do Norte Rev enferm UFPE on line. 2015; 9(supl. 6):8643-52.