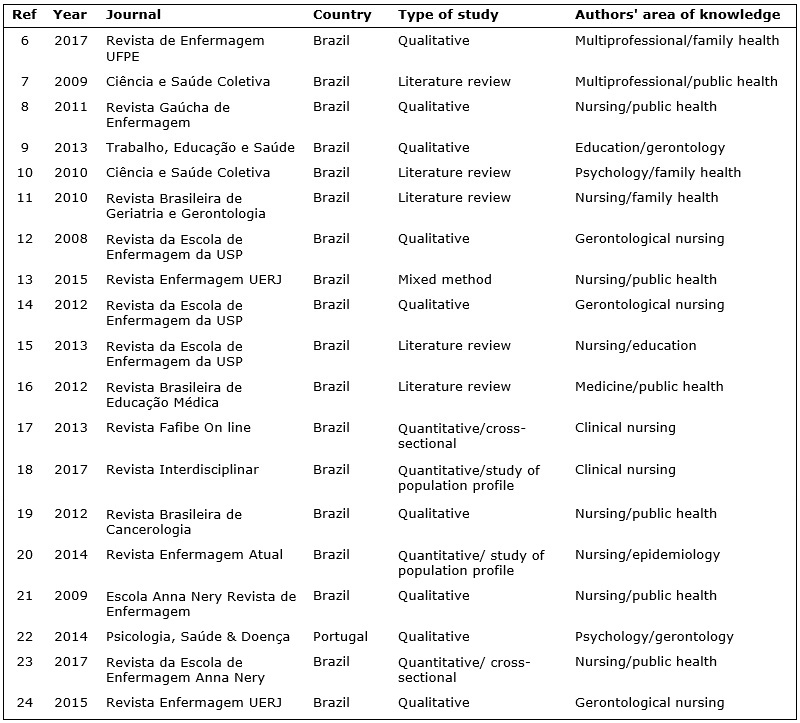
FIGURE 1: Characteristics of included studies. Period of publication 2008-2017.
REVIEW ARTICLES
Factors affecting adhesion by older women to gynecological cancer prevention programs
Aline Fatima Correia BatistaI; Célia Pereira Caldas II
I
Specialist in Geriatrics and Gerontology, Policlínica Hospital Municipal
Duque de Caxias. Rio de Janeiro, Brazil. E-mail: alifatima1922@gmail.com
II
Associate Professor. Nursing School, Universidade do Estado do Rio de
Janeiro. Brazil. E-mail: ccaldas@uerj.br
DOI: http://dx.doi.org/10.12957/reuerj.2017.21839
ABSTRACT
Objective: to discuss the factors that affect older women's adhesion to gynecological cancer prevention programs. Method: a literature search of the LILACS, SCIELO and BIREME databases (published in 2006-2017) and in official documents of the Ministry of Health and the Brazilian Cancerology Society found 142 articles, 19 of which were retained for review after applying the inclusion criteria. Results: women's adherence to gynecological cancer prevention programs was found to be affected by five factors: health service access and accessibility difficulties; social prejudices in relation to old age; availability of a person to accompany the older woman to the health service; insufficient training for health professionals to work with older women; and inadequate investment in health education in this area. Conclusion: health education to break down health professionals' prejudice towards aging will help to ensure that older women adhere to cancer prevention programs and facilitate the prevention, early detection and treatment of oncological diseases.
Keywords: Gynecological cancer, geriatrics, gerontology, health education.
INTRODUCTION
The number of new Brazilian cases of cervical cancer expected in 2016 is 16,340. Excepting non-melanoma skin tumors, cervical cancer is the most common cancer in the northern region of the country. Cervical cancer is the second most common in the center-western and northeastern regions, it is the third in the southeastern region and it is in the fourth place in the south of the country1.
Similar to the cervix, the vulva presents lesions considered pre-malignant. Only 10% of these lesions evolve to vulvar cancer. In developed countries, endometrial cancer is the most common site for cancer of the female genital tract; IN Brazil, it is in fourth place of the genital sites. There has been a gradual increase in the number of patients with endometrial cancer in recent years, due to the increase in life expectancy as endometrial cancer is a cancer of elderly woman and also because of the significant increase in the prolonged and indiscriminate use of estrogenic hormones to treat the symptoms of climacteric and menopause2.
Ovarian cancer is one of the most common gynecological cancers and the fifth leading cause of death due to cancer in women with more than 50% of cases occurring in over 40-year-old women. The peak of the disease occurs between 75 and 79 years of age. More than two thirds of the patients are diagnosed in advanced stages with ascites (Stage III). In Brazil, this accounts for 1.8% of all female cancers3.
Death rates among cancer patients are high, with gynecologic cancer having a high incidence in the elderly. This is related to the early onset of sexual activity and motherhood, sexual promiscuity with multiple partners, which increases the risk for sexually transmitted diseases, eating habits, long-term use of contraceptives, prolonged and indiscriminate use of estrogenic hormones to treat the symptoms of menopause and climacteric, smoking, early menarche and late menopause, multiparity and nulliparity. This information generates discussion in the field of geriatrics and gerontology, where there is a concern about active and healthy aging. Although life expectancy has increased, the concern in this field is to stimulate health care and avoid functional disability related to chronic degenerative diseases such as cancer.
Traditionally, cell senescence is described as a process of protection against oncogenesis in that it limits the number of cell divisions. Faced with this, it is to be expected that the longer that one lives, the greater the chances of acquiring and dying of cancer. This actually occurs in the elderly up to the seventh decade. However, from the age of 85, death rates due to cancer tend not to rise, which leads us to suppose that other factors are involved in these individuals4.
Death due to cancer is influenced by clinical and socioeconomic factors, as well as the availability and quality of the care provided. Nursing professionals involved in the management and planning of screening programs or in providing direct care to women, participate in all stages of prevention, early detection and treatment of cervical cancer. Thus, these professionals are committed to reducing intraregional inequalities and the quality of care, both in individual and collective contexts5.
The present study reviews the literature in the field of women's health, geriatrics and gerontology. Its objective was to discuss the factors that interfere in the adherence of elderly woman to gynecologic cancer prevention programs.
METHODS
This is a comprehensive review of the literature. The data were collected through a survey of scientific research published in the Latin American and Caribbean Literature on Health Sciences (LILACS), Scientific Electronic Library Online (SCIELO) and Virtual Health Library Databases (BIREME).
To organize the information contained in the 142 scientific publications initially found, the abstracts of the works were read quickly to identify the focus, objectives of the study and results. The selection of the publications considered parameters such as the period of publication and its relationship to the proposed theme using the keywords: Gynecologic cancer; geriatrics and gerontology; interdisciplinarity; Health education.
The inclusion criteria used to select articles were studies available in full in Portuguese, published between 2006 and 2017 and with a focus on the elderly. Nineteen articles were identified 6-24. The results were discussed based on the information available in documents of the National Cancer Institute (INCA)1,25,26, Ministry of Health (Portaria N ° 675 / GM of March 30, 2006)27 and the Brazilian Society of Cancerology2, with specific references to oncological diseases in geriatrics and gerontology.
RESULTS AND DISCUSSION
Of the 19 articles identified using the inclusion criteria6-24, none were published in 2006, 2007 or 2016.
Of the 19 studies, 18 were conducted in Brazil and one in Portugal. Regarding the field of knowledge, 13 studies were related to nursing, six of which were public health nursing, three gerontological nursing, two clinical nursing, one nursing education and one family health nursing. Moreover, two studies were on psychology (one in the area of family health and the other in the area of gerontology). One study was from the area of gerontological education and another from public health medicine. Two studies were multidisciplinary in the area of public health. Therefore, studies in the areas of nursing and public health were most common. Qualitative studies predominated, with nine articles. There were four literature reviews and four quantitative studies. One study applied mixed methodology and one study was a report on experience. The characteristics of the studies are listed in Figure 1.
FIGURE 1: Characteristics of included studies. Period of publication 2008-2017.
In the analysis of these studies, five factors were identified that interfere with elderly women's adherence to gynecologic cancer prevention programs: difficulty in accessing/accessibility to health services; the preconceptions of society in general in relation to old age; the availability of a person to accompany the elderly woman to the health service; the insufficient training of the health professionals who work with elderly woman; insufficient investment in health education actions in this field.
Factor 1 - Access and accessibility to health services
Access to health care is the first point to be discussed. Ordinance No. 675 MS/GM of March 30, 200627 is the Charter of Rights of Users of Health Services, which consolidates the rights and duties of exercising citizenship in health throughout the country. This ordinance ensures, as a first principle, orderly and organized access to health services, aiming at fairer and more efficient care. The eighth paragraph states that guaranteeing accessibility implies an end to architectural barriers and communicability, offering adequate conditions of care, especially to people with disabilities, the elderly and pregnant women. The legislation ensures comprehensive care for the elderly, but in practice, services and actions do not meet the true necessities relating to the quality of life of the elderly population, they do not promote autonomy and disregard the precariousness of health services6.
Although health care is a universal right in Brazil, access to services by the elderly population is strongly influenced by their socioeconomic situation or that of their family. The elderly with lower monthly household incomes have worse health conditions and visit doctors less frequently compared to those with better socioeconomic statuses7. Major healthcare problems, such as unequal access, inadequate services when they really need them, lack of comprehensive care, the parallelism of supply and the low quality of services, define guidelines for the restructuring of care models8. It is worth emphasizing that the difficulty of access is not only due to the functional disability of the elderly. Socioeconomic conditions have a considerable influence on the health of the elderly person. Many forget their own health needs due to the family, they are caregivers of their own family members and they guarantee family support. According to the gerontological literature, in the great majority of Western countries women end up carrying out the task of caring. Generally, these women are middle-aged or elderly, wives or daughters, who live with the elderly and have no help to provide care23,24. In this way, the self-care of these women is affected. Many intrinsic and extrinsic factors may contribute to the development of cancer. Exposure to factors is cumulative in time, and therefore, the risk of cancer increases with age. But it is the interaction between the intrinsic and extrinsic factors that determines the individual risk of cancer25.
Factor 2 - Preconceptions in relation to old age
The second factor to be discussed is the view of the elderly, family, society and health professionals in relation to the aging process, where there are still dogmas and prejudices that start from an outdated context and that need to be worked on daily.
In the context of old age, in addition to the perception of the elderly regarding the meaning of healthy aging in order to reach this stage of life with good health and feeling well, it is necessary to consider the life habits of the elderly, as well as their behaviors in relation to old age. The behavior of non-elderly people in respect to the elderly and the elderly relative to their own age depends on the interaction between different beliefs and between the cognitive and affective attributes of attitudes. Behavior directly influences changes in outlooks and the way people deal with learning in respect to health. How older people will act in relation to their own health and other aspects of their lives depends, to a large extent, on the images of old age and their attitudes towards aging9.
It is seen that considering only the elderly in this context is not enough. It is necessary for society to understand that the elderly need to be monitored, treated and respected. The paradigm of an elderly dependent, without expectation regarding their health just waiting for the death process, has been broken. The practice of active and healthy aging is a focus of the elderly; the National Policy on Elderly Health, instituted by ordinance 2528/GM of October 19, 2006, aims to ensure adequate and dignified care for the elderly Brazilian population28.
Factor 3 - Availability of a person to accompany the elderly to healthcare services
The family and the caregiver are an important basis for guaranteeing the continuity of adherence to prevention programs, since the increase in the life expectancy of the Brazilian elderly population leads to an increase in chronic diseases that can lead to functional disability, thereby making the elderly dependent29,30.
It is within the family and by the family that essential healthcare is provided. Healthcare ranges from the affective interactions necessary for the full development of mental health and the mature personality of its members to learning about hygiene and food culture and involves the level of adherence to the treatment prescribed by healthcare professionals (medications, diets and preventive activities). This complementarity takes place through concrete actions in the families' daily life that allow illnesses to be recognized, a search for medical care, incentive for self-care and, not least, emotional support10.
Numerous situations of long-term dependencies accepted by families reveal that people with advanced and progressive disease are cared for by informal caregivers, whether family members or not. On the other hand, these caregivers perform tasks assigned to them most of the time without proper guidance and with ineffective support from the health system11.
Several difficulties are related to family assistance to the elderly including the lack of social policies to provide support to caregivers, reductions in the family size due to falling fertility, increased breakups of marriages and families with elderly people who have a family income of less than three minimum wages with formal support being incapable of replacing the family12.
The health system needs to provide educational measures and support to the family, caregiver and the elderly. Health education is a very important part of this process, since the organization of the health system does not only depend on professional support, but also on the availability of structural resources in the municipality, as previously discussed.
Factor 4 - Insufficient training of the health professionals
Life-long education of health professionals needs to be established in all health systems. A continuous renewal of educational abilities remains critical. Thus, it will be possible to transform and disrupt social dogmas, facilitating the elderly user's adherence to health services, especially regarding the prevention of gynecological cancer.
The biased view of many health professionals related to some pathologies remains latent. In the case of the elderly, it is common to find professionals who, due to ignorance of the aging process, attribute signs and pathological symptoms to age. Others have outdated concepts regarding this type of cancer, not respecting or inappropriately following guidelines for the screening of elderly women in relation to the prevention and early detection of gynecological cancer.
The Brazilian guidelines for cervical cancer screening recommend that cytopathological examinations should be performed once a year in women between 25 to 60 years of age and, after two consecutive negative annual tests, every three years13,26.
Even with the extension of health care from the 1980s, the majority of the elderly are only approached because of chronic diseases and the occasional sporadic consultation without continuity, without considering the impact of this situation on their quality of life. Precarious care for the elderly can be observed due to the high proportion of deaths with ill-defined causes (up to 65%) and to the underreporting of problems considered expected or normal for the age and not responsive to interventions 7.
Our beliefs generate our behaviors, which generate our way of caring. The understanding that health professionals have of the elderly, interferes in the way they care for and treat them. Only by knowing this perception and understanding it, is it possible that we develop training programs and review paternalistic/authoritarian positions that inhibit the autonomy and independence of the elderly. The assumption is made that training seeks not only to improve the knowledge but also the attitudes of health professionals so that they can assess and treat conditions that afflict older people by providing them with tools and strengthening them with the focus on healthy aging14.
The interdisciplinarity that has been forgotten for decades is again the watchword in educational proposals, articulating projects and sustaining visions and procedures in the most varied areas. Professionals with different graduations willing to move between specific areas of training, articulate their specific knowledge with others in the work organization making it possible to share actions and to delegate activities to other professionals as a collaborative practice15. It is an important mechanism in geriatrics and gerontology, since the joint action of professionals tends to have very positive effects on the aggregation process of the elderly/family with health services.
The population of older women has increased in all Brazilian states. However, the joint goal of the Ministry of Health and the states in respect to cervical cancer screening has not been achieved in any of the states and the screening rate has even decreased in some20. Knowing the reasons that influence the non-performance of cervical cancer screening is necessary in order to understand the behaviors of these women 21 . The qualification of the health team associated with better working conditions and decent access to the health service are key elements in the health of the elderly.
Factor 5 - Little investment in health education related to this field
Health education is a very important strategy in the establishment of behavior that promotes or maintains good health. It is a social practice that contributes to the formation of people's critical awareness of their health problems, taking into account their reality. It also stimulates the search for solutions and the organization of individual and collective actions. It is considered a resource by which scientific knowledge in the health area influences the daily life of people, as, an understanding of the determinants of the health-disease process, provides support to the adoption of new habits and health behaviors16.
A study carried out at a long stay institution found that many elderly women, when asked about the preventive examination for cervical cancer said that they had never performed it and adding that they were not interested in doing so for the following reasons: lack of sexual activity, shame, fear and as they considered themselves close to death. This last reason was a surprise and a special cause of concern for the researchers as these women not only did not perform the preventive examination, but also they did not perform other actions of self-care. This practice can really harm their health and their quality of life. Some women suggested that preventive examinations were only important for promiscuous women17.
Low socioeconomic status is related to the incidence of cervical cancer because of less access to health services making it impossible to perform the pap smear, to adopt disease prevention measures and to continue treatment. Women of higher economic class and consequently a higher level of schooling, are more aware of the practice of safe sex 18. Faced with this situation, it is essential to encourage women to attend gynecological consultations and, especially, to ensure access to this type of service is facilitated 19.
Investment in health education has a great influence on the user's adherence to health services. It is necessary that the professional has the ability to work with health education, respecting social, economic and cultural aspects and the most varied age groups, since the family and caregiver are also part of this process. Using an appropriate language and respecting the particular universe of the elderly, which also includes cognitive issues, is essential to obtain satisfactory results.
CONCLUSIONS
This study showed, through a literature review, that five factors interfere with women's adherence to gynecological cancer prevention programs. These factors are the difficulty to access health services; the prejudices of society in general in relation to old age; the availability of a person to accompany the elderly woman to the health service; insufficient training of health professionals who work with the elderly woman and the lack of investment in health education actions in this field.
The integrality of care provided by the Statute of the Elderly, the structure of health services, interdisciplinarity together with health education for the individual and family, respect for the particularities of each elderly person and the professional's understanding of geriatrics and gerontology, are fundamental pieces in the process of aggregating this user, aiming to break down taboos acquired throughout life, stimulating health practices and consequently promoting active and healthy aging.
In conclusion, by eliminating the prejudice of many professionals regarding aging, seeing the elderly as an adult with increased life expectancy and innumerable possibilities for a full life, and working with health education respecting social barriers, we will contribute to the number of older women who are more conscious and concerned about health. Thus, the prevention, early detection and treatment of gynecological cancer and other types of oncological diseases that may affect this age group will be facilitated.
REFERENCES
1. Instituto Nacional de Câncer (Br). José Alencar Gomes da Silva. [site de Internet]. Estimativa 2016/2017 do câncer do colo do útero. [cited on July 31, 2017] Available from: http://www.inca.gov.br/wcm/dncc/2015/index.asp
2.Sociedade Brasileira de Cancerologia [site de Internet]. Câncer ginecológico. [cited on July 31, 2017]. Available from: http://www.sbcancer.org.br/?s=cancer+ginecol%C3%B3gico
3.Simões JC, Gama RR, Winheski MR. Câncer : estadiamento & tratamento. São Paulo: Livraria e Editora Marina; 2008.
4.Veras R, Lourenço R. Formação humana em geriatria e gerontologia: uma perspectiva interdisciplinar. Rio de Janeiro: UnATI/UERJ; 2006.
5.Santos RS, Melo ECP, Santos KM. Análise espacial dos indicadores pactuados para o rastreamento do câncer do colo do útero no Brasil. Texto contexto - enferm. 2012; 21( 4 ): 800-10.
6.Freire IM, Nogueira MF, Lucena IM, Alves MSCF. O Atendimento em unidades de saúde da família: um estudo de representações sociais com idosos. Revista de Enfermagem UFPE on line. 2017; 11(4): 1652-61
7.Melo MC, Souza AL, Leandro EL, Mauricio HA, Silva ID, Oliveira JMO. A educação em saúde como agente promotor de qualidade de vida para o idoso. Ciênc saúde coletiva. 2009; 14 (supl. 1): 1579- 86
8.Soares MC, Mishima SM, Silva RC, Ribeiro CV, Meinckes SMK, Corrêa ACL. Câncer de colo uterino: atenção integral à mulher nos serviços de saúde. Rev. Gaúcha Enferm. 2011; 32 (3): 502-8.
9.Patrocinio WP, Pereira BPC. Efeitos da educação em saúde sobre a atitude de idosos e sua contribuição para a educação gerontológica. Trab educ Saúde. 2013; 11 (2): 375-94.
10.Gutierrez DMD, Minayo MCS. Produção de conhecimento sobre cuidados da saúde no âmbito da família. Ciênc saúde coletiva . 2010; 15 (supl.1): 1497-508.
11.Portella MR. Atenção integral no cuidado familiar do idoso: desafios para a enfermagem gerontológica no contexto da estratégia de saúde da família. Rev Bras Geriatr Gerontol 2010; 13 (3): 501-6.
12.Simonetti JP, Ferreira JC. Estratégias de coping desenvolvidas por cuidadores de idosos portadores de doença crônica. Rev esc enferm USP. 2008; 42(1): 19-25.
13.Costa MS, Leite ES, Torquato JA, Costa IP, Sarmento AMMF, Moreira MASP. Práticas interdisciplinares na promoção da saúde da pessoa idosa. Rev enferm UERJ. 2015; 23(6):773-9.
14.Schimidt TCG, Silva MJP. Percepção e compreensão de profissionais e graduandos de saúde sobre o idoso e o envelhecimento humano. Rev esc enferm. USP. 2012; 46 (3): 612-7.
15.Peduzzi M, Norman IN, Germani ACCG, Silva JAM, Souza GC. Educação interprofissional: formação de profissionais de saúde para o trabalho em equipe com foco nos usuários. Rev esc enferm USP. 2013; 47 (4): 977-83.
16.Rodrigues BC, Carneiro ACMO, Silva TL, Solá ACN, Manzi NM, Schechtman NP,et al. Educação em saúde para a prevenção do câncer cérvico-uterino. Revista Brasileira de Educação Médica . 2012; 36 (supl. 1): 149-54.
17.Olhê L, Oliveira RC, Campanelli RF, Nogueira LDP. Papanicolau na terceira idade: um desafio para a enfermagem. Revista Fafibe on line. 2013; 6 (6): 78-86.
18.Tavares NCM, Santos VSMS, Queiroz RCCS , Souza IBJ , Pinto AP , Castro ABBSC. Perfil clínico, sexual e reprodutivo das mulheres que realizaram o exame papanicolau no ambulatório de uma faculdade em São Luís-MA. Revista Interdisciplinar. 2017; 10 (1): 129-38.
19.Melo MCSC, Vilela F, Salimena AMO, Souza IEO. O enfermeiro na prevenção do câncer do colo do útero: o cotidiano da atenção primária. Revista Brasileira de Cancerologia. 2012; 58(3): 389-98.
20.Rodrigues L, Silva PS, Oliveira MLC, Moraes F, Gomes L. Rastreamento do câncer do colo uterino na população idosa: um estudo das regiões geográficas do Brasil. Revista Enfermagem Atual. 2014; 14 (70): 29-34 .
21.Ferreira MLSM. Motivos que influenciam a não realização do exame papanicolau segundo a percepção de mulheres. Esc Anna Nery. 2009; 13 (2): 378-84.
22. Areosa SVC, Henz LF, Lawisch D, Areosa RC. Cuidar de si e do outro: estudo sobre os cuidadores de idosos. Psic, Saúde & Doenças. 2014; 15(2): 482-94.
23.Orlandi AAS, Brito TRP, Ottaviani AC, Rossetti ES, Zazzetta MS, Gratão ACM. Perfil de idosos que cuidam de outros idosos em contexto de alta vulnerabilidade social. Esc Anna Nery [Internet]. 2017 [cited on July 31, 2017]; 21(1): e20170013. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1414-81452017000100213&lng=en .
24.Costa SRD, Castro EAB, Acioli S. Apoio de enfermagem ao autocuidado do cuidador familiar. Rev enferm UERJ. 2015; 23(2):197-202.
25.Instituto Nacional de Câncer José Alencar Gomes da Silva (Br). Ações de enfermagem para o controle do câncer: uma proposta de integração ensino-serviço. 3ª ed. rev. ampl. Rio de Janeiro: INCA; 2008.
26.Instituto Nacional de Câncer José Alencar Gomes da Silva (Br). Diretrizes brasileiras para o rastreamento do câncer do colo do útero. 2ª ed. rev. atual. Rio de Janeiro: INCA; 2016.
27.Ministério da Saúde (Br). Portaria GM n° 675, de 30 de março de 2006. Aprova Carta dos Direitos dos Usuários da Saúde, que consolida os direitos e deveres do exercício da cidadania na saúde em todo o País. Brasília, (DF): Gabinete Ministerial, 2006.
28.Ministério da Saúde (Br). Portaria GM nº 2.528, de 19 de outubro de 2006. Aprova a Política Nacional de Saúde da Pessoa Idosa. Brasília (DF): Gabinete Minesterial; 2006.
29.Zaponi ALB, Tocantins FR, Vargens OMC. O enfermeiro na detecção precoce do câncer de mama no âmbito da atenção primária. Rev enferm UERJ.2015;23(1):33-8.
30.David HMSL. Sem uma enfermagem participativa, não haverá saúde de qualidade para cuidar bem das pessoas. Rev enferm UERJ.2015;23(2):147.