1 TA=Totally Adequate 2 A=Adequate 3 PA= Partially Adequate 4 I=Inadequate
ORIGINAL RESEARCH
Validation of educational technology on phototherapy to guide family members of icteric neonates
Elisama Brito de JesusI; Arinete Véras Fontes Esteves II; Elizabeth TeixeiraIII; Horácio Pires de MedeirosIV; Marcia Helena Machado NascimentoV; Vera Maria SaboiaVI
I
Nurse. MSc. Nurse at Secretaria Municipal de Saúde de Manaus. Amazonas,
Brazil. E-mail: enfelisamabrito@gmail.com
II
Nurse. PhD. Associate Professor at Universidade Federal do Amazonas.
Brazil. E-mail: arineteveras@bol.com.br
III
Nurse. PhD. Visiting Professor at Universidade do Estado do Amazonas.
Brazil. E-mail: etfelipe@hotmail.com
IV
Nurse. MSc. Nursing course coordinator at Faculdade Estácio Castanhal.
Pará, Brasil. E-mail:
horacio_medeiros@yahoo.com.br
V
Nurse. PhD. Universidade do Estado do Pará. Brasil. E-mail: marciahelenamn@gmail.com
VI
Nurse. PhD. Full professor at Universidade Federal Fluminense. Rio de
Janeiro, Brasil. E-mail: verasaboia@uol.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2018.21789
ABSTRACT
Objective: to validate an educational technology on phototherapy designed to guide family members of icteric neonates. Method: a methodological study carried out in 2012 with 9 specialist, 11 nursing assistants and 11 family members, through the application of questionnaires later submitted to statistical analysis. The study was conducted in a state public maternity hospital in the city of Manaus, Brazil. Results: the technology that was to be validated was a double-sided flip chart called The light that heals, the hand that cares. The Content Validity Index was 79.7%. The Concordance Index for the validation of appearance was 96.1% among nurses and 97.2% among family members. Conclusion: the educational technology was validated for content and appearance and demonstrated potential for orientations of family members of icteric neonates conducted by nurses who work in the neonatal and maternity areas.
Descriptors: Nursing; health education; phototherapy; orientation.
INTRODUCTION
The term technology is very broad and is used in several areas of knowledge. It refers to techniques, methods, instruments, procedures, tools, equipment and settings that enable one or several outcome/processes 1. Educational technologies are extremely important for educational work and for the care process, and nurses need to reflect on their role as educators, which challenges them to be creative, flexible and sensitive professionals when listening to the other2.
The motivation for this study arose during practical classes in the Nursing Undergraduate Course; there was a frequent conflict between the nursing/health team and the mothers and/or relatives of jaundiced neonates regarding their way of thinking and acting during the phototherapeutic treatment. For the mothers and/or family members, the situation was new, unknown and unexpected, while for the team that dealt with the procedure on a daily basis, it was a familiar practice. When there were doubts, the nursing staff tended to provide superficial information, such as what to do - how to do.
Another study found that this situation is delicate for mothers who have their children hospitalized in neonatal intensive care units (NICUs). Mothers suffer from separation, experiencing feelings such as loneliness, anxiety, fear of asking staff about their child's health, shyness towards an unknown team, and sometimes even symptoms of postpartum depression3.
Studies corroborate that nursing professionals have little knowledge about caring for the family, failing to consider them as partners in the care process. Thus, there is a need for a continuing education that encourages critical reflection on educational work and education at work4,5. Therefore, an educational technology validated by judges and by the target public could be a useful tool to address the care and education of the relatives of jaundiced neonates.
This research is justified since the validation processes includes, besides specialized judges, the target public. This can be understood as an expression of civil rights in the health area, as it is giving voice to individuals so that they can express their opinion on educational technologies that are built for them. In addition, the use of educational technologies by nurses improves nursing care.
In this sense, the objective of this study was to validate an educational technology on phototherapy, on the form of a double-sided flip chart, designed to guide family members of jaundiced neonates.
LITERATURE REVIEW
Jaundice is a common condition in the neonatal period, especially in the first week of life. In this period, it is the most common diagnosis and treatment6. The yellowish color of the skin and sclera, a characteristic of jaundice, is caused by an elevation in serum bilirubin, which is called hyperbilirubinemia7.
In most neonates, the jaundice is only physiological and does not have serious repercussions. But, in some cases, bilirubin levels can be extremely high, increasing the risk of neurological damage, kernicterus8.
The initial therapy of choice for persistent physiological jaundice or pathological jaundice in newborns is phototherapy, and, in the most severe cases, the exchange transfusion. Phototherapy is the most widely used treatment with neonates hospitalized in neonatal intensive care units (NICUs) or in wards (two-bed room or more), as it is not invasive and is highly effective in decreasing bilirubin levels. It is a treatment that exposes the body surface of the newborn to a light source, which can be a fluorescent, halogen or LED light7-9.
In the context of nurses' work, it is possible to encounter care-educational possibilities, based on the person-person, person-tool and/or person-universe relationship, which can be very useful if applied in the educational care process in the neonatal environment10.
From a caring and educational perspective, educational technologies can be considered an innovative possibility to conceive/justify technological products and processes developed, validated and/or used, transcending their conception as solely educational or assistance technologies, that is, correlating care and education.
As a complement, it should be emphasized that validation studies in the field of educational technologies are important, since validity will guarantee the quality of the material used. The process of validation will measure the degree of mediation that the technology created aims to achieve. Therefore, it can be said that the validation procedure is not the validity of the object itself, but of the purpose for which it was developed11.
METHOD
This is a method development study carried out in six phases: after the literature review (phase 1), the educational technology was elaborated, in the form of a double-sided flip chart (phase 2); one side was directed to the relatives of jaundiced neonates undergoing phototherapy and the other to the nurse who facilitates the teaching-learning process. Content (phase 3) and design (phase 4) were then validated. In this article, we highlight the quantitative results of phases 3 and 4 of validation.
Method development research focuses on the development, evaluation and improvement of methodological tools and strategies12. The validity is related to the measurement properties of an instrument, and it is not considered a simple task, but one of extreme importance, since the instrument is only scientifically valid after validation studies are conducted13.
The theoretical and methodological framework proposed by Pasquali was used, which consists of three principles: theoretical, empirical and analytical. The theoretical analysis of the items includes the semantic analysis, which addresses their intelligibility, and the analysis by the judges, which is the analysis of the instrument itself, concerned with the relevance of the items. In the empirical analysis, the psychometric quality of the instrument is evaluated. And, in the analytical principle, it is possible to estimate the validity and reliability of the instrument14. In this study, we chose to use the procedures of the theoretical principle, since they are considered the most important and are focused on theorizing about the object of interest11.
The study was conducted in 2012, with nine specialist judges, eleven care nurses and eleven family members, through the application of questionnaires later submitted to statistical analysis. It was conducted at a state public maternity hospital in the city of Manaus, AM, Brazil.
The group of specialist judges was composed by those who reached 9 points (health professionals) or 8 points (professionals from other areas) in a set of inclusion criteria. The nurses and relatives selected were those present at the time of data collection in the department where the jaundiced neonate was hospitalized and who used phototherapy in the hospital settings. Each group was composed of an odd number of subjects, in order to avoid ambiguous questions15.
The instruments used were organized in three parts: identification, instructions and blocks of questions in Likert Scale: Totally Adequate (TA); Adequate (A); Partially Adequate (PA); Inadequate (I).
The judges' instrument had four blocks: objectives; structure and presentation; relevance; general comments and suggestions. The target audience instrument had six blocks: objectives; organization; writing style; design; motivation; general comments and suggestions.
In order to determine the validity of the technology, the Content Validity Index (CVI) was used as a parameter, summing the TA + A options. Thus, the answers were considered as concordant (TA + A), indecisive (PA) or discordant (I).
The study project was submitted to the Research Ethics Committee of the Federal University of Amazonas (UFAM) for evaluation and was approved under Protovol no. 86,547.
RESULTS
Characterization of participants
The group of expert judges was composed of nine professionals, three nurses with expertise in neonatology, one nurse with expertise in education, one physician with expertise in neonatology, one psychologist with expertise in educational psychology, a pedagogue with expertise in educational technology and teaching-learning, a social communicator with expertise in visual communication and a graphic designer with expertise in visual programming. There were eight women and one man. The age ranged from 32 to 60 years, with a mean of 47 years. Regarding length of service, they had between 9 and 31 years of service, with an average of 21.66 years.
The target group consisted of two subgroups: eleven nurses (subgroup A - acronym NTA - nurse target audience) and eleven relatives (subgroup B - FTA - family target audience). Among nurses, the age ranged from 27 to 50 years, with an average of 35.7 years. All nurses had, at least, a specialist certificate degree directly related to their field of activity. Length of service ranged from 1 year (minimum time for inclusion in the study) to 22 years, with an average of 5.9 years. Among the family members (nine mothers and two fathers), the age ranged from 18 to 35 years, with an average of 26.18 years. Regarding their level of education, 2 (18.18%) had completed elementary education, 4 (36.36%) completed secondary education and 5 (45.45%) had a higher education degree.
Content Validation
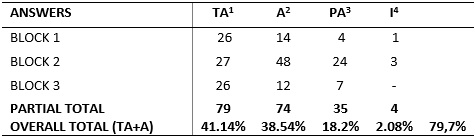
The specialized judges who participated in the content validation produced 192 responses, of which 79 (41.14%) were Totally Adequate - TA and 74 (38.54%) were Adequate - A, with a general agreement of 79.7%, as shown in Table 1.1.
Table
1: Answers from the judges in the three blocks Manaus, 2012. (N=192)
1 TA=Totally Adequate 2 A=Adequate 3 PA= Partially Adequate 4 I=Inadequate
Design validation
The first of the target audience, composed of nurses, produced 286 responses, of which 219 (76.57%) were Totally Adequate - TA and 56 (19.58%) were Adequate - A, with a general agreement of 96.1%, according to Table 2.
Table
2: Answers from the target audience – nurses according to the blocks.
Manaus, 2012. (N=286) 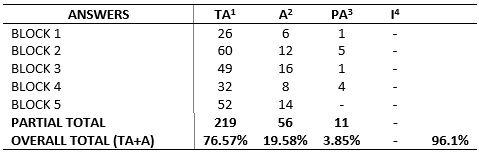
1 TA=Totally Adequate 2 A=Adequate 3 PA= Partially Adequate 4 I=Inadequate
The second group of the target audience, composed of relatives, produced 286 responses, of which 248 were Totally Adequate – TA (86.71%) and 30 (10.48%) were Adequate - A, with a general agreement of 97.2% , according to Table 3.
Table
3: Answers from the target audience – family members according to the
blocks. Manaus, 2012. (N=286) 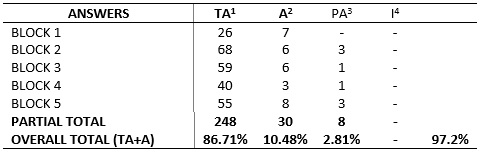
1 TA= Totally Adequate 2 A=Adequate 3 PA= Partially Adequate 4 I=Inadequate
Specialist judges and target audience suggestions
The suggestions and considerations of the judges and the target public converged on the following aspects: it is necessary to take into account the culture, ethnicity and particularities of the family members of jaundiced neonates; it is important to identify the risks, prevent and treat possible complications; it is relevant to build the technology in partnership with its target audience; it is necessary to include family members of jaundiced neonates in the context of care; the flip chart will be able to bring professionals closer to the families.
Based on the validation and suggestions, adjustments were made on the flip-chart (phase 5), aiming to improve the quality of the educational technology. With the final version, the authorship protocol was implemented (phase 6).
DISCUSSION
The double-sided flip chart, The Light That Heals, The Hand That Cares, was based on evidence from the literature, which pointed out, among other things, the needs of the family members of jaundiced neonates. After its elaboration, its content and design were validated considering a level of agreement above 70%, as recommended by specialists11,16. The Likert Scale that guided the instruments allowed qualitative facts – the judges' opinions - to be transformed into quantitative facts – numbers of the options17.
Regarding the participation of the target audience in the process of design validation, it is known that prevention actions constructed and shared with the individuals for whom they are intended tend to achieve greater success and effectiveness in the teaching-learning process18.
It was possible to perceive the reduced presence of fathers among the participants of the research. One of the possible reasons for this fact is that men are still the main breadwinners of some families and they have, as a rule, only few days of work leave. Considering that the jaundiced neonate needs longer hospital care, this father may have difficulty to manage his time, and he will also have to take on household chores while his partner is in the neonatal unit19.
It is possible to observe an incipient, but still perceptible growth of the presence of the father figure in ward and NICUs, with their active participation in the care provided to their children. The proximity to the infants benefits the triad father, son, and mother and the presence of the father in the neonatal unit helps strengthening the support network of the mother. Therefore, the healthcare team must value these moments by promoting family-centered care19,20. In addition, the involvement of the father in the care routine with the newborn is another possibility for establishing a father-child bond21.
Regarding the content of the flip chart, one of the issues raised by the judges during the analysis was to include more information regarding the side effects of phototherapy. These were already mentioned in the first version; however, it was considered prudent to give more prominence to this theme. Studies report that mothers have little knowledge about jaundice and phototherapy and that the information they receive is mostly superficial. In addition, the lack of communication between family and healthcare team may generate problems in the care provided to the newborn22.
Considering that it is important to value the singularities and subjectivities of the family member/learner, non-verbal language should also be used when thinking about an integrative and participatory health education mediated by technology, favoring face to face contact and dialogue. In the context of a more humanized and emancipatory educational practice, it is necessary to guarantee the student's autonomy and decision making capacity23,24.
It is worth mentioning that the flip chat was created with the intention of being an instrument to assist in the teaching-learning process facilitated by the nurse. Therefore, the effectiveness of health education will depend directly on the nurses' educational ability and experience, as showed in the National Curricular Guidelines for Undergraduate Nursing Courses 25. However, it is still necessary to overcome challenges and obstacles to the training and raise awareness among professionals, so that they see the establishment of a family bond as an important aspect and treat it as a fundamental tool in the provision of care26.
Educational technologies can qualify nursing practice, improve nurses' knowledge on education and highlight the scientific knowledge created and developed throughout the history of the profession, with the objective of improving the nursing care provided to the client/patient27.
Care-educational technologies aligned with reality can provide the patient with the possibility of conquering, advancing, overcoming and transforming reality, significantly improving their quality of life based on the knowledge built and developed by nursing professionals28. Therefore, the development and validation of educational technologies should be considered as a process of nursing know-how1.
It is important to note that there was no "inadequate" answer in the relevance block of the flip chart. This reinforces that the model of educational technology adopted provides great possibilities for the development of an educational process with a broad, welcoming point of view, valuing humanization and the establishment and/or strengthening of bonds between professionals, family and newborn, evidencing that comprehensive and humanized care are national healthcare guidelines and, therefore, should also be applied in neonatal units29,30.
It is important to note that this technology, a double-sided flip chart, allows the educator to work with it, trying to establish effective communication, paying attention to the facial expressions, sounds and gestures of the family member/learner, remembering to listen before talking and therefore, remaining sensitive to the learners' individuality 31,32.
Another factor in the structure of the flip chart pointed as positive by the target audience was the illustrations and introductory phrase on the side intended for the learner, with informative-guiding content on the face intended for the nurse. The efficacy of communication through illustrations and of the flexibility of the educational process according to the needs of each individual is recognized1.
A study carried out to analyze the good practices adopted to care for the woman and her newborn found that the nurse must value the complaints, expressions and feelings of the women, as this will enable the elaboration of a care plan that meets their particularities, guaranteeing comprehensive and quality care33.
The puerperium period is a time of many changes and adaptations for the mother. For the mothers of a jaundiced neonate, the construction of motherhood can be an even more delicate process, surrounded by uncertainties. They will always have deal with the separation factor, either in hospitalization units or due to the need for the neonate to be exposed to phototherapy light while blindfolded. According to the literature, these challenges can become easier when the professional helps resolving these uncertainties and then builds a support network, establishing bonds. It is interesting to note that the nursing professional has a special role in dealing with these uncertainties, due to the difficulties presented by other health professionals in this situation 4,34,35.
Therefore, the health care team must be open to the needs of the mothers, mindful to their social knowledge, and then welcome and educate them with a questioning perspective. In this perspective, health education stimulates the reflection and action of individuals with the purpose of granting them autonomy and participation36.
Some mothers who have their children hospitalized in NICUs resent not receiving this type of sensible care. The relationships are based on hierarchy and contain little dialogue. When it does happen, dialogue in about the institutional norms regarding the newborn. This generates fear to express doubts, increases feelings of insecurity and can even provoke anger due to the impersonal treatment received and to the rules imposed by the healthcare team37.
In a study on problem-based health education, aimed at promoting independent maternal care with the premature neonate, the educational process was horizontal, with the learner and not for the learner, establishing a relation of rights and fairness. When this mother is empowered, she is able to assume an active position in care, even in neonatal units38.
It is possible to perceive that the use of educational technologies can facilitate the teaching-learning process. In addition, when the family member acquires knowledge, he or she becomes more secure to care for the newborn30. It is important for the nurse and the healthcare team to exercise listening and sensitive praxis to strengthen the support network for the mother, including her family and the newborn and providing them education and support31,39.
CONCLUSION
The educational technology was validated in terms of content and design, with potential to orient family members of jaundiced neonates and to guide nurses working in the neonatal and maternity areas.
The flip chart was well evaluated by the target audience, nurses and relatives of jaundiced neonates. During the data collection, they expressed interest in obtaining the technology for the service, since they considered it of great value for the practice and they did not have an educational tool available.
This study is expected to allow the use of this educational technology, which could be an important strategy to the care-education action, helping the nurse in the education of family members of jaundiced neonates undergoing phototherapy and also instigating new research in other spaces, aiming to empower and establish bonds through a questioning perspective.
New studies must be carried out to carefully evaluate the application of the technology, following its repercussions among nurses and family members in the medium and long term. Among the limitations of the study, we highlight the small sample and the single scenario, which restricts the generalization of the findings.
REFERENCES
1.Nascimento MHM, Teixeira E. Educational technology to mediate care of the
"kangaroo family" in the neonatal unit. Rev. bras. enferm. (Online) 2018;
71(suppl. 3):1290-7.
2.Santos ZMSA, Lima HP. Tecnologia educativa em saúde na prevenção da hipertensão arterial em trabalhadores: análise das mudanças no estilo de vida. Texto & contexto enferm. 2008; 17(1):90-7.
3.Campos ACS, Cardoso MVLM, Pagliuca, LMF, Rossi, LA. Communication: basic nursing instrument to look after mother of newborn under phototherapy. Rev. Rene (Online). 2008; 9(4):24-32.
4.Ribeiro JSST, Sousa FGM, Santos GFL, Silva ACO, Sousa BAP. Nurses' attitudes toward the families caring process regarding the childbirth and the immediate postpartum period. Rev. pesqui. cuid. fundam. (Online). 2018; 10(3):784-92.
5.Fagundes NC, Rangel AGC, Carneiro TMC, Castro LMC, Bárbara dos Santos Gomes BS. Continuing professional development in health for working nurses. Rev. enferm. UERJ. 2016; 24(1):e11349.
6.Stevenson DK, Wong RJ. Metalloporphyrins in the management of neonatal hyperbilirubinemia. Semin. fetal neonatal med. 2010; 15(2):164-8.
7.Almeida MFB. When should we start phototherapy in preterm newborn infants? J. pediatr. (Online). 2004; 80(4):285-7.
8.Greco C, Arnolda G, Boo NY, Iman F. Iskander IF,
Okolo AA, et al. Neonatal Jaundice in Low and Middle-Income Countries:
lessons and future directions from the 2015 Don Ostrow Trieste Yellow
Retreat. Neonatol. 2016; 110:172-80.
9.Campos ACS, Cardoso MVLML. Educational technology for nursing care practice for mothers of newborns under phototherapy. Texto & contexto enferm. 2008; 17(1):36-44.
10.Salbego C, Nietsche EA, Teixeira E, Girardon-Perlini NMO, Wild CF, Ilha S. Care-educational technologies: an emerging concept of the praxis of nurses in a hospital context. Rev. bras. enferm. (Online). 2018; 71(suppl. 6):2666-74.
11.Teixeira E, Mota VMSS, organizadoras. Tecnologias educacionais em foco. São Caetano do Sul (SP): Difusão; 2011.
12.Polit DF, Beck CT, Hungler BP. Fundamentos de pesquisa em enfermagem. Porto Alegre (RS): Artmed; 2004.
13.Oliveira MS, Fernandes AFC, Sawada NO. Educational handbook for self care in women with mastectomies: a validation study. Texto & contexto enferm. 2008; 17(1):115-23.
14.Oliveira MS. Autocuidado da mulher na reabilitação da mastectomia: estudo de validação de aparência e de conteúdo de uma tecnologia educativa [dissertação de mestrado]. Fortaleza (CE): Universidade Federal do Ceará; 2006.
15.Lopes ML. Uso de simulação filmada para avaliar o relacionamento interpessoal enfermeiro-paciente no cuidado ao adulto hospitalizado [tese de doutorado]. São Paulo: Universidade Federal de São Paulo; 2004.
16.Lacerda RA, Nunes KB, Batista AO, Egry EY, Graziano KU, Angelo M et al. Evidence-based practices published in Brazil: identification and analysis of their types and methodological approaches. Rev. Esc. Enferm. USP . 2011; 45(3):777-86.
17.Enoki C., Yamamoto E, Marietto M, Meireles M, Convergência e concordância. In: II Simpósio de excelência em gestão e tecnologia; 2005; Resende; Brasil. Resende (RJ): Associação Educacional Dom Bosco;2005.
18.Armindo GL, Diniz MCP, Schall VT. Printed educational materials about dengue: qualitative and quantitative analysis and reflections about health communication and health education. In: Atas do VIII Encontro Nacional de Pesquisa em Educação em Ciências e I Congresso Iberoamericano de Investigación em Enseñanza de las Ciéncias; 2011 dez 5-9; Rio de Janeiro, Brasil. Rio de Janeiro: Associação Brasileira de Pesquisa em Educação em Ciências; 2011. p.138-48.
19.Santana JO, Borges KI, Souza DA, Pinto KRTF, Rossetto EG, Zani AV. Paternal care for hospitalized premature children: maternal representations. Rev. baiana enferm. 2017; 31(4):e22310.
20.Skene C, Gerrish K, Price F, Pilling E, Bayliss P. Developing family-centred care in a neonatal intensive care unit: an action research study protocol. J. adv. nurs. 2016; 72(3):658–68.
21.Matos MG, Magalhães AS, Carneiro TF, Machado RN. Building the father-infant bond: the experience of fathers. Psico USF. (Online). 2017; 22(2):261-71.
22.Ivo RS, Ribeiro LM, Leon CGRMP, Schardosim JM, Guarda LEDA, Beleza LO. Maternal perception and construction of an educational material on phototherapy. UFPE on line. 2017; 11(suppl. 12):5361-9.
23.Torres GMC, Figueiredo IDT, Cândido JAB, Morais APP, Almeida MI. The use of soft technologies in the care of hypertensive patients in Family Health Strategy. Esc. Anna Nery Rev. Enferm. 2018; 22(3):e20170169.
24.Demarchi SM, Gouvea MPG, Souza SP. Paulo Freire in the nursing academic production: a bibliometric study. Rev. pesqui. cuid. fundam. (Online). 2017; 9(4):1094-8.
25.Conselho Nacional de Educação (BR). Câmara de Educação Superior. Resolução CNE/CES 3/2001. Diário Oficial da União. Brasília (DF): Conselho Nacional de Educação; 2001 nov 09. seç.1, p.37.
26.Moura EL, Santos RS, Rocha SS. Evidence on reception and bond of nurses strategy health. Rev. Saúde em foco. 2015; 2(2):62-79.
27.Leopardi MT. Produção e aplicação das tecnologias nos sistemas de saúde. In: Nietsche E, Teixeira E, Medeiros HP, organizadores. Tecnologias cuidativo-educacionais: uma possibilidade para o empoderamento do(a) enfermeiro(a)? Porto Alegre (RS): Moriá; 2014. p. 37-55.
28.Teixeira E, Medeiros HP. Tecnologias na literatura de enfermagem: do reconhecimento ao desenvolvimento. In: Nietsche E, Teixeira E, Medeiros HP, organizadores. Tecnologias cuidativo-educacionais: uma possibilidade para o empoderamento do(a) enfermeiro(a)? Porto Alegre (RS): Moriá; 2014. p. 57-73.
29.Wernet M, Ayres JRCM, Viera CS, Leite AM, Mello DF. Mother recognition in the Neonatal Intensive Care Unit. Rev. bras. enferm. (Online). 2015; 68(2):228-34.
30.Cherubim DO, Rodrigues AP, Paula CC, Padoin SMM, Trojahn TC, Rechia FPNS. The nursing care meanings to mothers aiming at the lactation maintenance in a neonatal intensive care unit. Rev. pesqui. cuid. fundam. (Online). 2018; 10(4):900-5.
31.Barbosa EMG, Sousa AAS, Vasconcelos MGF, Carvalho REFL, Oriá MOB, Rodrigues DP. Educational technologies to encourage (self) care in postpartum women. Rev. bras. enferm. (Online). 2016; 69(3):545-53.
32.Cabeça LPF, Sousa FGM. Dimensions qualifying for communication of difficult news in neonatal intensive care unit. Rev. pesqui. cuid. fundam. (Online). 2017; 9(1):37-50.
33. Andrade LFB, Rodrigues QP, Silva RCV. Good Partices in obstetric care and its interface with humanization of assistance. Rev. enferm. UERJ. 2017; 25:e26442.
34.Rocha LLB, Dittz ES, Duarte ED, Costa PR. The experience of the hospitalized woman with the newborn in neonatal intensive therapy unit. Rev. enferm. Cent.-Oeste Min. 2018; 8:e2589.
35.Marques SFS, Oliveira TMG, Jesus CAC, Pinho DLM, Ribeiro LM. Uncertainties of newborn's parents in intensive therapy units incertitumbres de los padres de recién nacidos internados en unidades de terapia intensiva. Rev. enferm. UFPE on line. 2017; 11(suppl. 12):5361-9.
36.Dodou HD, Oliveira TDA, Oriá MOB, Rodrigues DP, Pinheiro PNC, Luna IT. Educational practices of nursing in the puerperium: social representations of puerperal mothers. Rev. bras. enferm. (Online). 2017; 70(6):1250-8.
37.Wernet M, Ayres JRCM, Viera CS, Leite AM, Mello DF. Mother recognition in the Neonatal Intensive Care Unit. Rev. bras. enferm. (Online). 2015; 68(2):228-34.
38.Araújo BBM, Rodrigues BMRD, Pacheco STA. Promoting mothers' care for premature neonates: the perspective of problem-based education in health. Rev. enferm. UERJ. 2015; 23(1):128-31.
39.Riberio JP, Lima FBC, Soares TMS, Oliveira BB, Klemtz FV, Lopes KB, Hartmann M. Needs felt by women in the puerperal period. Rev. enferm. UFPE on line. 2019; 13(1):61-9.