RESEARCH ARTICLES
Psychological distress in adolescents who experience changes in family dynamics as a result of alcoholism
Vagna Cristina Leite da Silva PereiraI; Lorena Farias de PimentelII; Lawrencita Limeira EspínolaIII; Elisangela Braga de AzevedoIV; Maria de Oliveira Ferreira FilhaV
I
Nurse. Ph.D. student in Nursing. Professor of the Nursing School Nova Esperança. João Pessoa, Paraíba, Brazil. E-mail: vagna.cristina@bol.com.br
II
Nurse. Master in Nursing. Professor of the Medical Science School. Campina Grande, Paraíba, Brazil. E-mail: lorenafarias@outlook.com
III
Psychology. Master. Clinical Psychology of the Federal University of Paraiba. João Pessoa, Paraíba, Brazil. E-mail: lawrencita_@hotmail.com
IV
Nurse. Ph.D. in Nursing. Professor of the Medical Science. Campina Grande, Paraíba, Brazil. E-mail:elisangelaaz@yahoo.com.br
V
Nurse. Ph.D. in Nursing. Professor of the Graduate Program in Nursing by UFPB. João Pessoa, Paraíba, Brazil. E-mail: marfilha@yahoo.com.br
This article is an excerpt of the Master dissertation defended at the Graduate Program in Nursing UFPB entitled Prevalence of Mental Distress in Adolescents who live with Alcoholics Family.
DOI: http://dx.doi.org/10.12957/reuerj.2015.21629
ABSTRACT
This transversal, population-based study to investigate the impact of alcoholism on family dynamics and evaluate the families' cohesion and adaptability in relation to risk factors for psychological distress in adolescents, was conducted in João Pessoa, Paraíba State, in 2011. The sample of 715 from a population of 21,214 state school students was obtained by systematic, self-weighted, sampling technique, using the Family CAGE and SRQ-20 questionnaires and the FACES III scale. The results indicated that 242 respondents (33.9%) lived with alcoholic family members, of whom 97 (40.1%) displayed some kind of mental suffering; of these, 47 (48.5%) had families with average mental risk classification, but which remained functional in terms of cohesion and adaptability. It was concluded that adolescents living with alcoholic relatives suffer psychological distress, even though living in family contexts classified as functional with average risk for family mental illness.
Keywords: Nursing; mental health; alcoholism; family relationships.
INTRODUCTION
According to the World Health Organization, alcoholism reaches 10% of the population worldwide1,2. Concerning to Brazil, alcohol is among the most abused drugs or at least experienced by the population; the country is listed among the largest world producers of cachaça3. In this sense, research conducted in the country presented data on the routine use of the substance for a large portion of the Brazilian population, predisposed to chemical dependence3,4.
Alcohol abuse is a seriousVI problem requiring immediate and comprehensive care through prevention programs and policies that consider the psychosocial context of users and their families. Among the main problemas, there is the mental illness of people living with an alcoholic person. In Brazil, 12% (2,288,778) of the population has some type of mental disorder, severe or persistent, and 6% (137.326.68) of these people have problems related to psychoactive substance abuse5. These results were based on calculation of the Brazilian population with 190,732,694 people, according to census conducted in 20106.
Addressing to the complexity of alcohol dependency process involves taking as a starting point the family, since the subject´s relationship with parental figures is the primary setting of all the psychosocial development process. Nowadays, alcoholism is a psychosocial impairment that affects, besides the user, all their relationships cycle causing serious consequences, including damage to the quality of life and health of those living with drug addicts, like the psychological distress7.
Such suffering is understood in this study as a process of not adapting to difficult experiences in life or the small flaws in psychic development that can lead the individual to experience mild episodes, possibly transitory, prior to the mental illness process8.
Thus, the family lives representative duality of acting as a major source of protection and risk to the mental health of children and adolescents9,10, although it appears that the troubled daily living with the alcoholic person affects family dynamics causing the psychological distress 11,12. Within the same perspective, it is observed that children who raised in alcoholic families have shown weakened behavior during development13. Therefore, considering the ability to influence the psychosocial development of the individual - either positively or negatively - the family living resonate with other interaction environments and may be a factor for psychiatric disorders14.
Thus, the family context has aroused the interest of researchers, particularly with the implications of living with alcoholism phenomenon in the development of mental suffering, considering the exposure proven of one in four children and adolescents as a result alcohol abuse in the family environment15.
In this context, it emerged the need to seek better thematic coping strategies, together with subsidies for better understanding the familiar scenario in favor of reducing damage to the psychological development of adolescents exposed. It is worth highlighting that mental health promotion must target not only the alcoholic person, but his entire family16.
The development of research related to psychological damage in adolescents involved in scenarios with alcoholic relatives aims, above all, to promote improvements in the effectiveness of interventions. Therefore, as a challenge, the following question in this study is: What is the impact caused by an individual alcoholic in the family dynamics, especially for adolescents´ life that accompanies this problem?
Thus, the objective was to investigate the impact of alcoholism on family dynamics and evaluate cohesion and adaptability of families about the risk factors for psychological distress in adolescents.
LITERATURE REVIEW
Adolescence, by its peculiar critical feature causes a series of linked behavioral changes mainly to the mental development of personality and opinion formation of the subject17. During this period, the adolescent is exposed to health risk situations because of the biopsychosocial transformation process. International research indicates that 20% of the population of children and adolescents worldwide suffer from some psychological distress18,19.
In Brazil, the prevalence of mental illness in this group reaches on average 10% to 29%, and half of the adolescents between 10 and 17 years old is involved in at least two or more risk behaviors for mental illness20.
Risk situations experienced in the household since childhood compromise the mental health of the individual. Therefore, family relationships can contribute to the development of mental disorders and, in this case, there is the consumption of alcohol and drugs between the multiple factors of family risk 18. The presence of the alcoholic in the family interferes in family welfare and can result in a conflictual coexistence, involving stress, insecurity, fear that destabilize the whole core. Thus, alcoholic families have reduced adaptability, these homes are unpredictable, experience constant change processes resulting from its natural functioning and the arising of crisis11:152.
Another highlight is the low family cohesion since mutual support, cooperation and commitment are not always experienced in alcoholic families21 . Thus, when there is good cohesion, there is the healthy development and the preservation of psychosocial well-being of children and adolescents within their family, presented as an important protective factor for mental health in this group11.
Considering the vast majority of Brazilian families living with people who frequent use alcohol3,4, it is assumed that adolescents are daily experiencing changes in family dynamics that can cause mental suffering.
METHODOLOGY
It is a cross-sectional population-based study conducted in public schools in the city of João Pessoa, Paraíba/Brazil.
The student population in the municipality regularly enrolled in high school are 34,782 young people22. In this study, a population of 21,214 students enrolled in high school series in the age group 14-19 years old, male and female were chosen.
For the sample calculation, the basis worldwide survey19 was used estimating prevalence of 20% of children and adolescents with mental illnesses. The calculation was done with the sample size of the EPI OPEN (Open Source Statistics for Public Health) version 2.3.1, with a confidence level of 95% and a margin of error of 3%. The final sample consisted of 715 adolescents. A systematic sampling technique was used and the criteria adopted allowed reducing losses without compromising the reliability of the study.
The selection of the investigation was made from a database created in Excel 2007, with the help of a four-column table, organized in numerical order, in the proportion of 1 to N (1-21214), which distributed the number of students enrolled per class in each school. A equation was made: N/n and the number found determined the size range between one and another interviewee.
Data collection was carried out between May and November 2011. The criteria allowed to determine a sample self-weighted by the size of schools and classes in three shifts. The instruments used were the Questionnaire family CAGE- to trace the family alcoholism, the Self-Report Questionnaire (SRQ- 20), to identify mental disorders in populations without the presence of experts. And finally, the FACES III Scale, which assesses cohesion, adaptability and mental risk in families known as Family Adaptability and Cohesion Evaluation Scales, created by Olson in 1989 and validated in Brazil23,24.
The data were stored, encoded, and in some cases were grouped together to facilitate analysis of the variables. They were statistically analyzed with the aid of R software, version 2.010.0. To make the inference of data, statistical tests of X2 (chi-square) was used to investigate the relationship between the variables.
This study covers the ethical requirements proposed by Resolution 196/96 of the National Health Council, which provides standards and regulatory guidelines for research involving human beings. It was approved under the advice of Protocol 066/11 of a Research Ethics Committee.
RESULTS AND DISCUSSION
It was found that 242 (33.9%) of respondents live with alcoholics relatives and out of them, 97 (40.1%) had some form of psychological distress. According to the operation of the investigated families, it was found that the conflicting family relationships is characterized among the factors that contribute to psychological distress of adolescents.
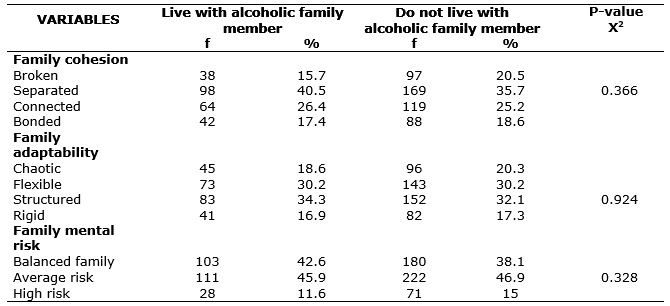
The development of mental health problems can be influenced by the individual characteristics, as well as their interactions with the family. Searching for family function, it is found that 40.5% of households were classified as separated with regard to family cohesion among adolescents who live with alcoholics. Regarding adaptability, families were considered structured (34.3%); with final average risk rating for mental illness (45.9%).
Among adolescents who do not live with alcoholic family members, the families were classified as separated (35.7%) and structured (32.1%); with final classification similar to the above average risk group for mental illness (46.9%). It was not found statistical significance between the variables, according to data in Table 1.
TABLE 1: Association Scale FACES III to the living of adolescents with alcoholic relatives in state schools. João Pessoa-PB, 2011. (N= 715)
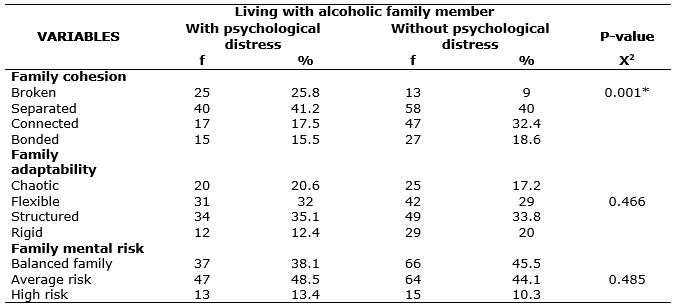
With regard to alcoholism in the family associated with psychological distress, it was identified that in reference to cohesion, adolescents living with family alcoholics suffering from psychological distress or not, have separate types of families, the first group with 41.2% and the second with 40%. Regarding family adaptability, it was observed that, when combined family alcoholism and mental suffering, the results indicated a structured family, the first group (35.1%) and the second group (33.8%) respectively as provided in Table 2.
When searching for the classification of the family risk in the first group, families are classified as medium risk (48.5%). In the group of adolescents without psychological distress who live with alcoholic family members, it was observed that the families were classified predominantly as balanced (45.5%). Another finding was as statistically significant association of the variable family cohesion with p-value = 0.001. Check Table 2.
TABLE 2: Association of Scale FACES III to the living of adolescents in psychic suffering with alcoholic relatives in state schools. João Pessoa-PB, 2011. (N=715)
The responses of the adolescents become clear that living relationships with the alcoholic family and the existence of psychological distress do not alter the frequency responses. It appears that in reference to cohesion in both groups, there are the families considered separated (39.5%) and (34.5%), respectively. See Table 3.
TABLE 3: Association of Scale FACES III to the not living of adolescents in psychic suffering with alcoholic relatives in state schools. João Pessoa-PB, 2011. (N=715)
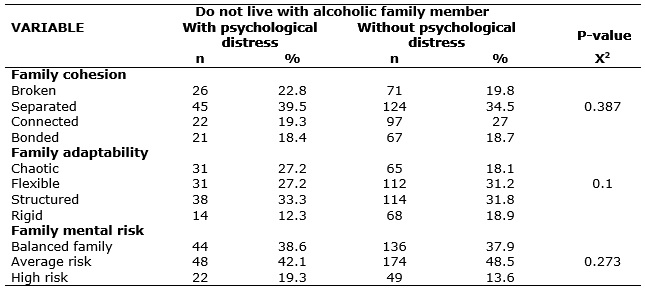
Concerning adaptability, the results were distributed proportionately, resulting in a final rating of structured families, 33.3% and 31.8%, respectively, in the two groups.
Adolescents with or without mental suffering not living with alcoholics have families classified as medium risk for mental illness, according to the final standings, 42.1% and 48.5% respectively in the two groups, with no statistical significance. See Table 3.
Even observing similar classification of low-risk family as functional, by the cohesion and adaptability in both groups, a reflection in the reflection is necessary that, even though adolescents living with family alcoholics had a higher prevalence of psychological distress, it is realized that the family environment has enabled to exercise its role as a member of this group. A functional family is not characterized only by the absence of problems but the ability to cope and solve them11.
According to the family adaptability, families have enabled young people the ability to change the reality, even in difficult situations. Thus, the family can contribute to mental integrity of its members, helping to overcome the adversities as a result of alcoholism24.
Although it is difficult to
[...] articulate the familiar diagnosis with individual diagnosis in the field of mental health, the association of interactional issues seems to be an appropriate way of understanding the individual factors and family interaction, a way to highlight elements of the same reality which, when combined, they trigger to some losses [...] 25:20 .
Especially in the area of nursing, the existence of consensus on some definitions has hampered the household assessment, making it imperative nurses increase their knowledge to draw more effectively nursing diagnoses in trying to help alcoholics and their family11:150.
In this study, adolescents who live with alcoholic family in psychological distress, with regard to cohesion, the families were classified as the separate type functional. That is, in the perception of adolescents and established classification, it is observed there is a loving relationship between adolescents and family members, because, according to the study, functional families are those in which the members have a sense of belonging, although there is possibility of individualization among them26. Despite the problems experienced, the family is the space in which its members preserve, practice and transmit values, (re) create links, stand, protect themselves, even in the experience of conflict27:195.
It is considered the importance of good family cohesion for healthy functioning of the core. However, the relationships in families with alcoholics are unbalanced, in most cases, people commune of relationship problems, experiencing crises, conflicts, and other situations that result in psychological distress28. In this context, families sometimes are in situations of exhaustion, fatigue and misunderstanding, leading to the need for continued aid, involving actions of social objects and support networks offering instrumental and emotional support29.
Regarding adaptability, it is emphasized the need of families showing possibilities to modify behavior in difficult situations and the ability to modify a reality that affect family interaction26. in In this investigation, there are not results showing that extreme values on which the families were classified as inflexible renewals or modifications that may interfere with their daily lives, a result that contradicts the findings of other studies 23,28 analyzing family relationships with drug addicts.
In this bias, a study of women victims of violence by family alcoholic member, the family was considered rigid to adaptability. In this type of operation, members are more often predispose to injuries, as this core is considered at high risk for mental illness28.
Living with such relational problems can act for the development of the subject facing adverse situations, giving the subject possibility to define as a social actor.7,27 On the other hand, not always family conflicts will contribute positively, sometimes consequences that arise at some point in life, as is the case of problems here investigated.
It is known that family interactions of low quality, permeated by conflicts, are often seen as a risk factor for onset of depressive symptoms. Family relationships play an important role in mediating the cognitive and emotional functioning of its members30.
Behaviors and attitudes resonate with changes within family members, causing misunderstanding and weakening of interpersonal relationships, revealed by feelings of ambiguity, helplessness, sadness and anger, expressed by relatives, in relation to its relative and situations generated by the condition of dependency to alcohol31.
Alcoholism disrupts and becomes responsible for family dysfunction, the daily life in these homes is unpredictable and family relationships are modified under the influence of chemical dependency.11 At this time, , it should be considered several aspects for effective nursing care of this core: functioning and dynamic support between family members32.
This theme is challenging for nursing, considering the implications for the quality of life and health of adolescents. The development of care plans are essential from interdisciplinary and cross-sectoral actions to this target audience so comprehensive care can be promoted.
The results discussed should be considered based on the limitations and potential biases. The study design allowed large cut of the study population, while investigating a theme that encompasses prejudice and social stigma difficult adherence of adolescents in the study. This limitation may have influenced the quality of data, while statistically has not allowed errors. Understanding family dynamics starting from statistical results is a challenge, because although there are methods, there is no consensus on what action would be most appropriate to assess family relationships32.
CONCLUSION
The results of this study show that adolescents living with alcoholic family members have a higher prevalence of psychological distress, as well as excessive use of alcohol can cause serious damages to the family functioning, contributing to a core with an average risk of mental illness.
It is also worth stating that the prevention of psychological distress among adolescents is a complex phenomenon that involves the entire development process and covers different influences on them exercised: family, school, social groups and other institutions. Thus, it needs to be addressed through comprehensive and effective public policies to reduce the growing rate of this malaise fostered over the years.
To advancing in how to address this issue, the Brazilian health policy needs to implement extended actions of health education, with different social actors and technicians theoretical contributions, considering the change in family structure caused by chemical dependency situation. It is emphasized the importance of family involvement in the care context, in order to break the paradigm of fragmented care, based only on the needs of the dependent.
Finally, on the data collected and the analyzes carried out, it is appropriate to carry out further research to expand nursing actions to strengthen the planning of public policies aimed at adolescent mental health as a result of the problem of addiction.
REFERENCES
1.World Health Organization (Who). The world health report 2002: reducing risks, promoting healthy life. Geneva: WHO; 2002.
2.World Health Organization (Who). Global status report on alcohol and health 2014. Geneva: WHO; 2014.
3.Acselrad G. Drinking in Brazil: study based on secondary sources. Rio de Janeiro: Faculdade Latino Americana de Ciências Sociais; 2012. [cited on 10 Jan 2015]. Available on: http://flacso.org.br/files/2015/02/RelatorioConsumodoAlcoolnoBrasilFlacso05082012.pdf .
4.Ministry of Justice (Br). National Policy on drugs. First National Survey on alcohol consumption patterns in our population. Brasília (DF): Ministry of Justice; 2007.
5.Ministry of Health (Br). National Coordination STD / AIDS. The Ministry of Health's policy to provide comprehensive care to users of alcohol and other drugs. 2nd ed. Brasília (DF): Ministry of Health, 2004.
6. Brazilian Institute of Geography and Statistics (IBGE). [internet]. Population Census 2010 [cited on Dic 2013]. Available on: http://www.ibge.gov.br/home/.
7.Sena ELS, Boery RNSO, Carvalho PAL, Reis HFT, Marques AMN. Alcoholism in the family context: a phenomenological view. Text-context – nursing [Scielo-Scientific Electronic Library Online] 2011 [cited on 23 nov 2014]. 20:310-8. Available on: http://www.scielo.br/pdf/tce/v20n2/a13v20n2.pdf.
8.Fleitlich-Bilyk B, Cunha GR, Estanislau GS, Rosário MC. Health and mental disorders. In: Estanislau GM, Bressan RA, organizers. Mental health at school. Porto Alegre (RS): Artmed; 2014. p. 25-36.
9.Orth APS, Moré CLO. The Working families with dependent members on psychoactive substances. Psicol argum [Scielo-Scientific Electronic Library Online] 2008 [cited on 10 Jan 2015]. 26(55):293-303. Available on: http://www2.pucpr.br/reol/pb/index.php/pa?dd1=2525&dd99=view&dd98=pb .
10.Ministry of Health (Br). Department of Health Care. Primary care Notebooks. Brasília (DF): Ministry of Health; 2013. [cited on 12 nov 2014]. Available on: http://bvsms.saude.gov.br/bvs/publicacoes/cadernos_atencao_basica_34_saude_mental.pdf .
11.Mangueira SO, Guimarães FJ, Mangueira JO, Fernandes AFC, Lopes MVO. Health promotion and public alcohol policies in Brazil: integrative literature review. Psicol Soc. 2015; 27(1):157-68.
12.Pereira VCLS, Andrade FA, Espínola LL, Azevedo EB, Nogueira JA, Ferreira Filha MO. Psychic suffering in adolescents associated with familial alcoholism: possible risk factors. Rev Eletron Enferm [Scielo-Scientific Electronic Library Online] 2015 [cited on 15 Jan 2015]; 17(2):178-85. Available on: http://dx.doi.org/10.5216/ree.v17i2.24396.
13.Fligie N, Fontes A, Moraes E, Payá R. Do children addicts of drug with psychosocial risk factors require a special look? Rev. Psiq. Clín [Scielo-Scientific Eletronic Library Online] 2004 [cited on 26 Feb 2015]; 31:53-62. Available on: http://www.scielo.br/pdf/rpc/v31n2/a01v31n2.
14.Santos DCM, Jorge MSB, Freitas CHA, Queiroz MVO. Adolescents in psychological distress and the children's mental health policy. Acta Paul Enferm [Scielo-Scientific Electronic Library Online] 2011 [cited on 16 June 2014]; 24:845-50. Available on: http://www.scielo.br/pdf/ape/v24n6/a20v24n6.pdf.
15.Souza J, Jeronymo DV, Zanoti E, Carvalho AMP. Emotional maturity and behavioral assessment of alcoholics´ children. Psicol Estud. 2005; 10:191-9.
16.Bernardy CCF, Oliveira MLF. The role of family relationships in the initiation to the use of drug abuse by institutionalized youths people. Rev esc enferm USP. 2010; 44: 11-7.
17.Campos DMS. Adolescent psychology: normal psychopathology. 22nd ed. Petrópolis (RJ): Vozes; 2010.
18.Organización Panamericana de la Salud. Community Mental Health. 2nd ed. Washington (DC): OPAS; 2009.
19.World Health Organization. Child and adolescent mental health polices and plans. Geneva: WHO; 2005.
20.Avanci JQ, Assis GS, Oliveira RVC, Ferreira RM, Pesce RP. Factors associated with mental health problems in adolescents. Psychol: theory and research. 2007; 23:287-94.
21.Trindade EMV, Costa LF. Considerations about the resilience of adolescent children in the family context of alcoholics. Com Ciências Saúde. 2012; 24:179-88.
22.Ministry of Education (Br). Instituto Nacional de Estudos e Pesquisas Educacionais Anísio Teixeira (INEP). School Census. Brasília (DF): INEP; 2010 [cited on 12 nov 2014]. Available on: http://www.inep.gov.br/basica/censo/censo.asp.
23.Falceto OG, Busnello ED, Bozzetti MC. Validation of diagnostic scales of family functioning for use in primary health care services. Rev Panam salud publica. [Scielo-Scientific Eletronic Library Online] 2000 [cited on 16 Jan 2015]; 7:255-63 Available on: http://www.scielosp.org/pdf/rpsp/v7n4/1928.pdf.
24.Fornazier ML, Siqueira MM. Nursing care to alcoholic patients in alcoholism assistance program. Jornal Bras de Psiq. [Scielo-Scientific Eletronic Library Online] 2006 [citeddd on 10 Jan 2015]; 55:280-7. Available on: http://www.scielo.br/pdf/jbpsiq/v55n4/a04v55n4.pdf.
25.Falceto OG. Families with functional and dysfunctional development: validation of diagnostic scales Faces III, Beavers-Timberlaw and overall assessment of interactional operation (Garf) [Masters dissertation]. Porto Alegre (RS): Federal University of Rio Grande do Sul; 1997.
26.Salgueiro H, Lopes MA. Family dynamics cohabiting and caring for a dependent elderly. Rev. Gaúcha Enferm. [Scielo-Scientific Eletronic Library Online] 2010 [cited on 13 Jan 2015]; 31(2):26-32. Available on: http://www.scielo.br/pdf/rgenf/v31n1/a04v31n1.
27.Silva PA, Silva MRS, Luz GS. Protective interactions in families of alcoholics: basis for the nursing work. Rev. enferm. UERJ [Scielo-Scientific Eletronic Library Online] 2012 [cited on 02 June 2015]; 20:191-6. Available on: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/4043/2808 .
28.Rabello PM, Caldas Júnior AF. Violence against women, family cohesion and drugs. Rev Saude Publ [Scielo-Scientific Eletronic Library Online] 2007 [cited on 13 March 2014]; 41:970-8. Available on: http://www.scielo.br/pdf/rsp/v41n6/5848.pdf.
29.Nóbrega MP, Oliveira EM. Women who use alcohol: qualitative analysis. Rev Saude Publ. [Scielo-Scientific Eletronic Library Online]. 2005 [cited on 13 March 2014]; 39:816-23. Available on: http://www.scielo.br/pdf/rsp/v39n5/26304.pdf.
30.Teodoro MLM, Cardoso BM, Freitas ACH. Affectivity and Family Conflict and Its Relation to the Depression in Children and Adolescents. Psicol. Refl. Crít. [Scielo-Scientific Eletronic Library Online]. 2010 [cited on 13 July 2014]; 23:324-33. Available on: http://www.scielo.br/pdf/prc/v23n2/v23n2a15.pdf.
31.Gonçalves JRL, Galera SAF. Assistance to family caregivers in contact with alcoholism through the problem solving technique. Rev Latino-Am Enfermagem. [Scielo-Scientific Eletronic Library Online] 2010 [cited on 13 June 2014]; 18(esp):543-9. Available on: http://www.scielo.br/pdf/rlae/v18nspe/a09v18nspe.pdf.
32.Souza J, Abade F, Silva PMC, Furtado EF. Family functioning assessment in the context of mental health. Rev Psiquiatr Clin. 2011; 38:254-9.