Minimum wage in force in the time of the study -R$ 678.00 (*)
ORIGINAL RESEARCH
Population-based study: socio-demographic and health profile of older adults
Álvaro da Silva SantosI, Joilson MeneguciII, Lúcia Marina ScatenaIII, Mariana Campos de SousaIV, Marta Regina FarinelliV, Renata DamiãoVI
I
Nurse. PhD in Social Sciences. Associate Professor of the Graduate program
in Health Care of the Federal University of Triângulo Mineiro. Brazil.
Email: alvaroenf@hotmail.com
II
Physical educator. Master in Physical Education. Doctoral student in Health
Care at the Federal University of Triângulo Mineiro. Brazil. E-mail:
joilsonmeneguci@yahoo.com.br
III
Production engineer. Post Doctor in Public Health Nursing. Associate
Professor at the Federal University of Triângulo Mineiro. Brazil. Email: lmscatena@uol.com.br
IV
Nurse. Specialist in Health of the Elderly. Mater in Health Care from the
Federal University of Triângulo Mineiro (UFTM). Brazil. E-mail:
mhppaiva@gmail.com
V
Social Worker. PhD in Social Work. Associate Professor of the Graduate
program in Psychology of the Federal University of Triângulo Mineiro.
Brasil.E-mail: martafarinelli@gmail.com
VI
Nutritionist. PhD in Sciences. Associate Professor of the Graduate program
in Physical Education of the Federal University of Triângulo Mineiro.
Brazil. Email: damiaorenata@hotmail.com
VII Acknowledgements to the Foundation for Research Support of Minas Gerais for
funding the study under protocol APQ-00995-11.
DOI: https://doi.org/10.12957/reuerj.2018.21473
ABSTRACT
Objective: to identify the sociodemographic and health profile of older adults in municipalities of the Uberaba Health Region in Minas Gerais, Brazil. Method: in this cross-sectional, population-based study, the Mini-Mental State Examination, a demographic and health profile instrument, the Mini Nutritional Assessment, WHOQOL-BREF and WHOQOL-OLD were applied to 3430 older adults in 24 cities, between 2012 and 2013. Data were analyzed using SPSS version 20.0. Results: female (61.5%), 60 to 69 years old (52.6%), no schooling or incomplete basic schooling (83.5%), income of one minimum wage or less (39.7%), pensioners (80.7%), mean 3.17 illnesses (SD = 1.92), use of 2.47 medicines (DP = 1.37), at risk for malnutrition (29.1%), overweight (62.9%), alcohol use (15.7%), smoking (15%), sedentary (43.1%), and with lowest quality of life scores in the environment domain (62.0%; DP = 13.2) and autonomy facet (66.8%; DP = 16.4). Conclusion: the study population was characteristically female, low-income, overweight, sedentary, had three diseases, and lowest quality of life scores in the environment domain and autonomy facet.
Descriptors: Health of the Elderly; aging; health profile; Population studies in Public Health.
INTRODUCTION
The life expectancy of the world population has increased, and in Brazil the increase was of five years in the period from 2000 to 2013. Such increase differs according to factors such as gender and level of regional development; Brazilian women live approximately 78.5 years while men live 71.2 years1.
Population aging has caused an inversion in the age pyramid2. Projections for 2050 show that the world will have about two billion elderly people, and Brazil will be the sixth country with the largest number of elderly people3. In 2012, Brazil had about 12.6% of the total elderly people in the world2.
The Southeast region has the largest contingent of elderly people (12.7%). The contingents of these individuals in the states of the South region, Rio de Janeiro, Minas Gerais, São Paulo and Espírito Santo, are 15%, 12.2%, 12.2% and 10.8%, respectively4.
The state of Minas Gerais is divided into 13 divisions called Health Macroregions; 18 Regional Health Superintendencies; and 10 Regional Health Offices. The Triângulo Mineiro region is composed of two Macroregions: South Triângulo and North Triângulo. The Regional Health Superintendence of Uberaba (SRS Uberaba) corresponds territorially to the South Triângulo Macroregion, covering 27 municipalities. According to the latest demographic census, this Macroregion had 697,812 individuals, 82,134 of whom were 60 years old or older, representing 11.8% of the general population5.
Based on the reality that there are no population-based studies on the profile of the elderly in the South Triângulo/Minas Gerais, the goal of this study was to identify the sociodemographic and health profile of the elderly in the municipalities of the Regional Health Superintendence of Uberaba, Minas Gerais.
LITERATURE REVIEW
Demographic transition is a global event. The particular characteristics of each country, such as socioeconomic factors, result in different rhythms in this phenomenon between developed and developing countries6.
Due to the increase in the number of elderly people, the World Health
Organization (WHO) created a proposal of Active aging, with a view
to optimizing health, participation and safety as people age because the
epidemiological profile of the population has also changed; the number of
infectious diseases has decreased and the prevalence of chronic
non-communicable diseases (NCDs) has increased7.
Knowledge about the sociodemographic and health profile of the elderly population can, among other things, provide elements for better planning of public policies for this age group, with a view to active and healthy aging. A study describes the importance of investigations showing and discussing the conditions of life, health and social support of the elderly, the group that grows the most in the population, especially to meet their social, health, economic and even affective demands8.
METHODOLOGY
This is a cross-sectional study based on the population of 79,924 people aged 60 and over4, living in 24 municipalities that compose the Regional Health Superintendence of Uberaba. The municipalities have a territory of 33,594.041 km² and the average Human Development Index of 0.7172. The region studied is made up of three other municipalities, part of an earlier pilot study. This article is an excerpt of the project titled: Health profile of the elderly population of municipalities of the Regional Health Office - Uberaba/Minas Gerais .
The elderly population of each municipality was considered as reference for sample calculation9, as well as the following parameters: sampling error of 0.05; confidence interval of 95% and proportion of elderly people in each municipality (number of elderly people divided by the total population of the municipality). The minimum sample, considering the sum of the minimum samples of all municipalities, was calculated to be 3198. The sampling process was simple and random. Considering the risk of losses, an additional value of 20% was taken into account, corresponding to 3838 attempts.
The inclusion criteria of elderly people were: agreement to participate in the study by signing the informed consent form; absence of cognitive impairment according to the screening scale of the Mini Mental State Examination according to educational level10 and ability to walk, also with the aid of walking sticks or walkers. The exclusion criteria were: being wheelchair user, presence of severe hearing or vision impairment that could prevent communication, and being bedridden.
Data collection occurred between May 2012 and April 2013. The participants answered a structured questionnaire, applied through an interview by trained interviewers, and covering information on sociodemographic profile, health conditions, behavioral habits and quality of life. They had also they body mass (kilograms) and height (meters) measured.
The sociodemographic characteristics evaluated were sex; age group; marital status; schooling; color; religion; family income; housing; number of people living in the household; presence of financial aid from family members; paid occupation; retirement; presence of children who are alive; number of children who are alive; and presence of children who live with them.
The health conditions evaluated correspond to a self-assessment of health status; falls; use of orthosis or orthopedic prosthesis; use of dental prosthesis; self-reported diseases; consumption of medicines; search for medicines; nutritional assessment according to a Nutritional Mini-assessment11 classifying individuals as to malnutrition, risk of malnutrition or no risk of malnutrition; body mass index (BMI) calculated using the body mass in kilograms and the height in meters, and classified as low weight, eutrophic or overweight12; and ability to perform basic activities of daily living, determined by the Katz Scale adapted for the Brazilian 13. The scale investigates the following self-care activities: bathing, dressing, going to the bathroom, lying down and getting out of bed, eating and controlling urination and/or evacuation functions. The elderly were classified as dependent or independent.
In behavioral habits, the analyzed variables were: self-reported alcohol consumption; self-reported smoking; regular practice of physical activity; search for information about sexuality; practice of sexual activity; and condom use.
The quality of life was assessed using the WHOQOL-BREF14 and the WHOQOL-OLD 15validated for the Brazilian population, and the scores were calculated on a scale of 0 to 100. In the WHOQOL-BREF questionnaire, the following domains were assessed: physical; psychological; social relations; and environment. In the WHOQOL-OLD module, the following facets were verified: functioning of the senses; autonomy; past, present and future activities, social participation; death/dying; and intimacy.
The data collected were inserted in a spreadsheet from the Microsoft Office 2007 Excel® software through double typing and statistical analyses were carried out in the software Statistical Package for Social Sciences (SPSS) version 20.0. Descriptive data (frequency, mean and standard deviation) were calculated to present the data.
The participants were informed of the study's objectives and gave their written consent to participate. The present study followed the ethical principles of Resolution 466/12 of the National Health Council, and the research protocols were evaluated and approved by the Human Research Ethics Committee of the Federal University of Triângulo Mineiro (Opinion nº 1640/2010).
RESULTS AND DISCUSSION
This population-based survey identified the sociodemographic and health profile of elderly residents in 24 municipalities in the South Triângulo Mineiro. Due to the rapid growth of the elderly population, knowledge about the profile of this group has become important in the creation of public policies.
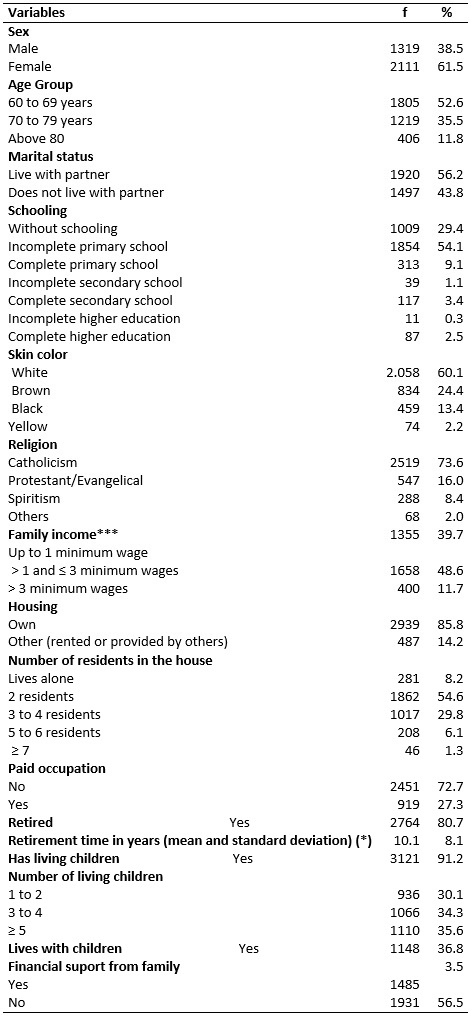
A total of 3430 elderly people were evaluated, with an average age of 70.1 years (SD = 7.3). Most of the participants were female (61.5%) in the age group between 60 and 69 years (52.6%), living with a partner (56.2%), with incomplete primary education (54.1%), white skinned (60.1%), and of the Catholic religion (73.6%). The family income was between one to three minimum wages (48.6%), most had their own house (85.8%), lived with two people at home (54.6%), received no financial support from the family (56.5%), had no paid employment (72.7%), were retirees (80.7%), and had an average retirement time of 10.1 years (SD = 8.1). A total of 91.2% elderly had living children, 35.6% had five or more children, 36.8% lived with them, and 56.5% did not receive financial support from their families, according to Table 1.
TABLE 1:
Sociodemographic aspects of the elderly. Regional Health Superintendence of
Uberaba, MG, 2013.
Minimum wage in force in the time of the study -R$ 678.00 (*)
A Brazilian study about the profile of the elderly showed similar values regarding gender and age group16.
The combination of aspects - living alone or with one other person, low level of schooling, low income and, not receiving any financial aid from family members - leads to a condition of social vulnerability, which should cause concern on the part of public and social policy managers and encourage them to interfere in this age group.
Having few people in the family circle, and living alone or without a partner can mean a low network of relationships and social support, and this is especially worrying when the elderly have poor health conditions. Low income and little financial support from the family can also denote the low purchasing power of the families and the difficulties these elderly face to have quality of life. An investigation which showed the vulnerabilities, including those of social nature, of elderly people reported a better income17 than the one found in the present study. In the mentioned study, the authors say that income is an important aspect because determines the access to goods and to care to meet the needs of the elderly.
The majority of the participants had no paid occupation, received income only from their retirement, which was therefore the main source of income. Despite of this, most of the surveyed people had their own house, which means an aspect of valorization in the life of the elderly, although this alone does not determines whether housing conditions are adequate or not.
Financial aid from family members to the elderly with low income, low education and greater dependence on retirement seems to be necessary. Only 43.5% reported receiving such support. Another study showed that 38.6% of the surveyed elderly received this financial support18.
In health conditions, 51.9% of the studied elderly considered their health state as regular or poor; 27.7% had suffered falls in the last 12 months, with an average of 2.3 falls (SD = 2.6); 59.9% used orthosis or orthopedic prosthesis; and 70.5% used dental prosthesis. As for diseases, there was an average of 3.17 diseases per elderly (SD = 1.78) among those who used medicines. The main health complaints were: systemic arterial hypertension (65.8%), musculoskeletal disorders (35.8%), hyperlipidemia (30.9%), rheumatic diseases (30.5%), heart diseases (24.5%), diabetes mellitus (19.9%), and depression (17.3%). As for use of medicines, 87.1% reported to use them, with an average of 2.47 drugs (SD = 1.37) per person. The more consumed medicines were antihypertensive (74.3%), followed by analgesics (45.1%) and diuretics (36.9%). The drugs were purchased by 47.1% in drug stores and in obtained in public services, according to Table 2.
TABLE 2:
Health conditions of the elderly. Regional Health Superintendence of
Uberaba, MG, 2013.
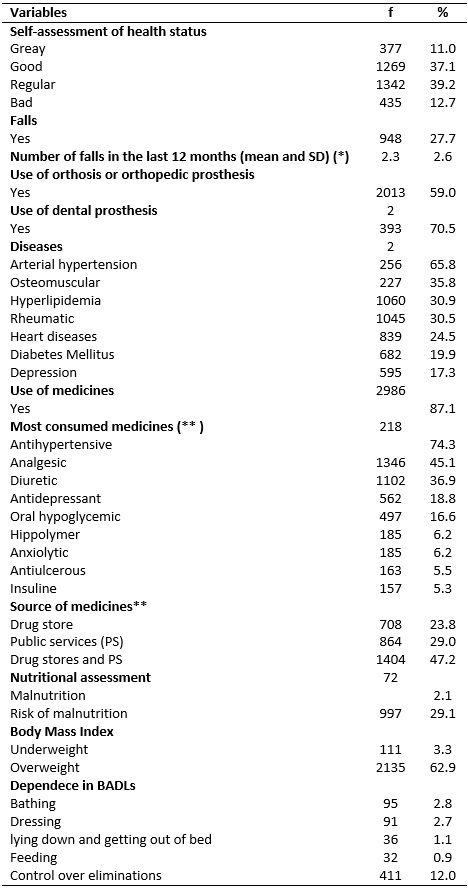
(*) In relation to those who suffered falls. (**) For those who consume
drugs.
A study conducted in the South with long-lived elderly showed values similar to the ones presented here. Better values were seen in a study carried out in Campinas, but there was a strong association with income 20.
An investigation carried out in São Paulo showed that 67.4% of the participants had arterial hypertension and 19.6% had Diabetes mellitus 21. Furthermore, diseases of the circulatory system as well as osteomuscular diseases were very freuquent21, similar to data of the present study. These diseases, when not properly monitored, can generate serious complications for the elderly, with high costs to the health system. Regarding the condition of depression, another study, also from Minas Gerais, showed an incidence of 15.5%22, which is lower than the present study.
In recent years, there have been actions to combat some of the most serious incidents in the community, especially among the elderly. The Hiperdia Program is one of these actions. In this program, the goal is to monitor and monitor hypertensive and diabetic people. Yet, other disorders have been somehow neglected, as is the case of depression, present here in 17.3% of the investigated elderly. The actions of the Hyperdia Program have generated economic impacts to the system, for it has been useful to reduce morbidities in users and promotion of better adherence to therapy 23. Hyperlipidemia - the second most mentioned pathology in the present study (30.9%) - also when chronic and without proper follow-up may lead to the onset or worsen of cardiovascular conditions. The presence of musculoskeletal and rheumatic diseases is a major cause of pain and prompts a high consumption of analgesics, which were the second type of medication most used in the studied population.
There were no similarities between the diseases mentioned and the profile of medicines consumed. This may denote a series of aspects: intake of medicines without prescription, lack of knowledge or denial of the disease, polypharmacy, and others. In every case, high consumption of medicines is clear. Consuming various medications for different conditions and being monitored in this practice seems to be therapeutically correct. A survey showed that the elderly consume on average four medications, with the most common being those with action on the cardiovascular system, as well as the practices of polypharmacy, self-medication and inappropriate consumption of medicines usual among the elderly24.
Access to medication is another important aspect. A low frequency of collection of medicines only in public services was observed; most elderly need to purchase the medicines, or combine the two possibilities of getting the medicines. Most of the income of the elderly, which is already low in the group surveyed, is used to purchase medicines. Given the economic situation of the health sector and of the country, and the number of drugs consumed by the elderly, besides the risks of inappropriate drug use, self-medication and polypharmacy, the use of medicines should be rational and monitored.
As for nutritional status based on MAN scores (MAN is an instrument that has high sensitivity and is capable of detecting undernourished elderly individuals, or at risk of malnutrition25), a significant percentage of elderly individuals at risk of malnutrition was found. In a study carried out with elderly residents in Criciúma-SC, it was observed that 25% presented risk of malnutrition26; that value is lower than the one observed in the present study.
When analyzing BMI, we found overweight elderly in this study. According to data from the Family Budgets Survey (POF, 2008-2009) carried out by the IBGE and the Ministry of Health, overweight predominated in the elderly population in relation to eutrophy and low weight27.
Regarding the Basic Activities of Daily Living (BADLs), there was an overall low dependence, but the continence function was the most affected (12%). This is in line with another study28. These data indicates the importance of measures to improve the control of urinary and evacuation functions, either through exercises or even practices that may facilitate such control, because this impairment may compromise, among other aspects, the socialization of the elderly.
When it comes to behavioral habits, 15.7% reported the consumption of alcoholic beverage and 15% the use of tobacco. In relation to physical activity, 43.1% did not practice it regularly. About sexuality, only 14.1% sought information on this topic, 44.5% had sexual activity and of these 81.6% did not use condoms. Regarding the quality of life according to facets (WHOQOL-BREF) and domains (WHOQOL-OLD), the highest mean scores were found in the social relations domain (73.5, SD = 14.1) and the death and dying facet (72.3, SD = 25.0), while the worst scores were on the environment domain (62.0, SD = 13.2) and the autonomy facet (66.8, SD = 16.4), as shown in Table 3.
TABLE 3:
Behavioral habits and self-reported Quality of Life of the elderly.
Regional Health Superintendence of Uberaba, MG, 2013.
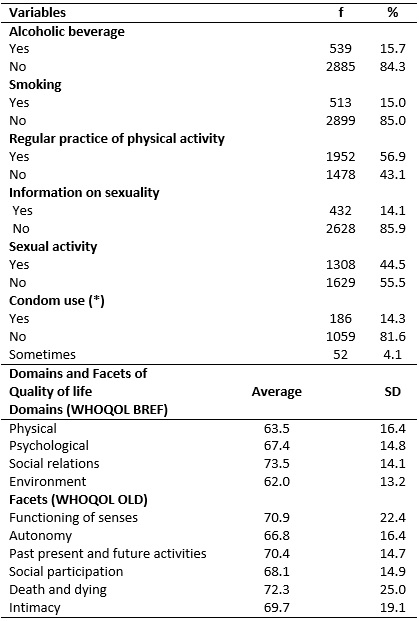
(*)
In relation to those who practice sexual activity.
Tobacco use among the elderly, and especially for longer periods, may cause important respiratory changes. Elderly smokers are frequently found to develop stroke, cancer and chronic lung disease29.
Alcohol consumption by the elderly is also an important public health problem. The majority of alcoholic elderly have low socioeconomic status and generally associate alcoholism with tobacco consumption. They tend to have cirrhosis, hypertension, diabetes mellitus and dementia30. Interventions aimed at alcohol users and smokers represent for health services an interdisciplinary work, with family participation, and the arduous task of prolonged actions.
The present study identified a high prevalence of lack of practice of regular physical activity among the studied elderly, a fact that deserves attention due to the association of this lifestyle with a higher risk of mortality31.
A research carried out in a Brazilian municipality verified that the negative perception of health is a barrier to the practice of physical activity32. This factor probably influenced the regular practice of physical activity among elderly participants of this study, since 51.9% negatively evaluated their health status. The relationship between physical activity and quality of life was demonstrated in a survey comparing active and inactive people; the first group had better perception in all domains 33. The number of elderly people who had falls in the last 12 months was also significant, a factor that can be influenced by poor adherence to physical activity. Falls also hinder physical activity after such events.
Lack of information about sexuality among the elderly can lead to unprotected sexual behavior, with serious risks of sexually transmitted diseases. Although a minority of elderly people has sexual activity, it is verified that those who had such activity do it in an unprotected way. Research showed that there is a belief that condoms reduce sexual pleasure and that prevention must be linked to infidel persons32. Here we point out challenges in health education practices, both to encourage elderly people to review what sexuality is and to teach them preventive practices. An investigation carried out with community elderly showed that the elderly saw sexuality beyond the sexual act, especially with regard to feelings and emotions34.
As for quality of life, the domain with lower score (WOQHOL-BREF) was environment, followed by the physical domain. In turn, the social and psychological relations domains stood out as the best scored. Regarding the facets (WOQHOL OLD), the best score was that of death and dying and the worst, autonomy. A survey showed that in the environment domain, family income and schooling are associated. In turn, in the physical domain, association was found between family income, schooling, the condition of being alone and age of 80 years or more35. A survey conducted in Portugal and Brazil also showed the facet death and dying as the best scored, and autonomy as the worst for Brazilian elderly36.
Another study showed that the physical function had the lowest scores among the ones evaluated as having a strong negative association with age 37. The proposal of better income and education to the elderly seems to be a challenge that must be shared with families and with the community. The reduced autonomy of the elderly is an important aspect to be worked out and is usually multifactorial, including the presence of physical limitations, access to income, difficulties in socialization, and others problems. These people should be monitored by health services with a view to improve their autonomy and satisfaction with life.
CONCLUSION
The objective of this research was to present the sociodemographic and health profile of the elderly population residing in the Regional Health Superintendence of the South Triângulo/Minas Gerais. There were vulnerabilities resulting from low income and lack of family support, especially financial support; low education level; living alone or with few people; relying solely on retirement; regular or poor health perception; compromised nutritional status (risk of malnutrition and overweight); sedentary life style, alcoholism and smoking with expressive frequency, as well as non-use of condoms in sexually active elderly; presence of several diseases among the elderly population (which are prevalent and well known in the health services) and high consumption of medicines, to which the elderly do not even have an easy access; and, perception of quality of life with low scores.
This study has as limitation to have covered only one health macroregion in one Brazilian state, what precludes the possibility of generalization to the national territory. However, it is possible that the results produced herein reflect the reality of many Brazilian regions, especially in the social and health conditions of the elderly.
It is concluded that there is a need for public policies aimed at the elderly in the region. Such policies should meet several needs, such as income generation; increasing of the levels of schooling; monitoring health problems; improving the access and monitoring the consumption of medicines; and finally health education actions that can expand self-care, physical activity, leisure, recreation, more conscious sexual activity, and family participation.
REFERENCES
1. Brazilian Institute of Geography and Statistics. Synthesis of social indicators: an analysis of the living conditions of the Brazilian population. Rio de Janeiro: IBGE; RJ, 2014.
2.Veras R. Contemporary population aging: demands, challenges and innovations. 2009; 43(3):548-54.
3. World Health Organization. Aging in the twenty-first century: a celebration and a challenge. 2012 [cited in 2017 Mar 02]. Available from: http://www.onu.org.br/populacao-com-mais-de-60-anos-alcancara-1-bilhao-de-pessoas-em-uma-decada/
4. Brazilian Institute of Geography and Statistics. National Household Sample Survey: Summary of Indicators 2011. Rio de Janeiro: IBGE; 2012.
5. Brazilian Institute of Geography and Statistics (IBGE). Preliminary results of the universe of the demographic census 2010, 2011. [cited in 2017 Mar 02] Available from: http://www.ibge.gov.br/home/estatistica/populacao/censo2010/resultados_preliminares/preliminar_tab_municipio_zip.shtm
6. Brito F. Demographic transition and social inequalities in Brazil. Brazilian Journal of Population Studies. 2008; 25: 5-26. DOI: doi.org/10.1590/S0102-30982008000100002.
7. World Health Organization. Active aging: a health policy. Translation by Suzana Gontijo. Brasília. (DF): PAHO; 2005. p. 60 (PAHO).
8. Silva HO, Maynna JC, Alencar D, Lima FEL, Vieira LR. Epidemiological profile of elderly people attending groups in the municipality of Iguatu, Ceará. Rev. Bras. Geriatr. Gerontol. (Online). 2011 [cited in 2017 Mar 02]; 14 (1): 123-34. Available from: http://revista.unati.uerj.br/scielo.php?script=sci_arttext&pid=S1809-98232011000100013&lng=en
9. Brazilian Institute of Geography and Statistics. IBGE-Cities - Minas Gerais: 2010. [cited in 2017 Mar 02]. Available from: http://cidades.ibge.gov.br/xtras/uf.php?lang=&coduf=31&search=minas-gerais
10.Bertolucci PHF, Brucki SMD, Campacci SR, Juliano Y. The mini mental state examination in a general population: impact of schooling. Archives of Neuro-Psychiatry. 1994; 52 (1): 1-7.
11.Guigoz Y, Vellas B, Garry PJ. Assessing the nutritional status of the elderly: the Mini Nutritional Assessment as part of the geriatric evaluation. Nutrition reviews. 1996; 54 (1 Pt 2): S59-65.
12.World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO Consultation on Obesity. Geneva (Swi): World Health Organization; 1998.
13.Lino VTS, Pereira SRM, Camacho LAB, Ribeiro Filho ST, Buksman S. Transcultural adaptation of the Independence Scale in Daily Life Activities (Katz Scale). Cad. Saúde Pública (Online) 2008; 24(1):103-12.
14.Fleck MP, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. Application of the Portuguese version of the short version of the WHOQOL quality of life assessment instrument. Rev. saúde pública. (Online) 2000; 34(2):178-83.
15.Fleck MP, Chachamovich E, Trentini C. Development and validation of the Portuguese version of the WHOQOL-OLD module. Rev. saúde publica. (Online) 2006; 40(5):785-91.
16.Santos AFLJ, Guerra RO, Falcão Nascimento AF, Maciel ÁCC. Profile of the social support provided for elderly people in the municipality of Natal, State of Rio Grande do Norte, Brazil, 2010-2011. Epidemiol. serv. saúde (Online). 2013 [cited in 02 Mar 2017] 22(2):335-46. Available from: http://scielo.iec.pa.gov.br/scielo.php?script=sci_arttext&pid=S1679-49742013000200015&lng=pt
17.Rodrigues NO, Neri AL. . Social, individual and programmatic vulnerability in the elderly in the community: study data FIBRA, Campinas, SP, Brazil. Ciênc. saúde coletiva (Online). 2012: [cited in 2017 Mar 02] 17(8):2129-39. Available from: http://www.scielosp.org/pdf/csc/v17n8/23.pdf
18.Jacinto LAT, Santos AS, Diniz MA, Silva LC, Pedrosa FSS, Arduíni JB. Coronary artery disease and family support among the elderly. Rev. enferm. UERJ. 2014; 22(6):771-7.
19.Pereira LF, Lenardt MH, Michel T, Carneiro NHK, Bento LF. A portrait of the health-disease profile of elderly people who are users of primary health care. Rev. enferm. UERJ. 2015; 23(5):649-55.
20.Borim FSA, Barros MBA, Neri AL. Self-assessment of health in the elderly: population-based research in the Municipality of Campinas, São Paulo, Brazil. Cad. Saúde Pública (Online). 2012; [cited in 2017 Mar 02] 28(4):769-80. Available from: http://www.scielosp.org/pdf/csp/v28n4/16.pdf
21.Cabrelli R, Sousa CS, Turrini RNT, Cianciarullo TI. Elderly people in family health units: morbidity and use of health services. Rev. RENE. 2014; 15(1):89-98.
22.Soares SM, Silva PAB, Santos JFG, Silva LB. Association between depression and quality of life in the elderly: primary health care. Rev. enferm. UERJ. 2017; 25(e19987):1-8.
23.Alves EBL. Nursing follow-up for elderly hypertensive patients: experience report. InterScientia: 2014; 2(2):3-15.
24.Santos TRA, Lima DM, Nakatani AYK, Pereira LV, Leal GS, Amaral RG. Consumption of medicines by the elderly, Goiânia, Brazil. Rev. saúde pública (Online). 2013 [cited in 2017 Mar 02]; 47(1):94-103. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-89102013000100013&lng=en&nrm=iso
25.Gobbi S, Sebastiao E, Papini CB, Nakamura PM, Valdanha Netto A, Gobbi LT, et al. Physical inactivity and related barriers: a study in a community dwelling of older brazilians. J. Aging Res. 2012; 2012:685190.
26.Ribeiro RSV, Rosa MI, Bozzetti MC. Malnutrition and associated variables in an elderly population of Criciúma, SC. Rev. Assoc. Med. Bras. 2011; 57(1):56-61.
27.Brazilian Institute of Geography and Statistics. Research of Family Budgets. 2008-2009. Anthropometry and nutritional status of children, adolescents and adults in Brazil. Rio de Janeiro:IBGE;2010.
28.Andrade NB, Novelli MMPC. Cognitive and functional profile of elderly people attending the Centers for interaction of elderly people in the city of Santos, SP. Cad. Ter. Ocup. UFSCar. 2015; 23(1):143-52.
29.Zaitune MPA, Barros MBA, Lima MG, César CLG, Carandina L, Goldbaum M et al. Factors associated with smoking in the elderly: Health Survey in the State of São Paulo (ISA-SP). Cad. Saúde Pública (Online). 2012 [cited in 2017 Mar 02]; 28(3):583-96. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0102-311X2012000300018&lng=en
30.Souza AAM, Sales LR, Gonçalves MS, Botelho TV, Xavier VLL. The elderly alcoholics assisted by the CAPS: role of the nursing team. Rev. Norte Mineira de Enf. 2014; 3(2):79-89.
31.Wu CY, Hu HY, Chou YC, Huang N, Chou YJ, Li CP. The association of physical activity with all-cause, cardiovascular, and cancer mortalities among older adults. Prev. Med. 2015; 5(72C):23-9.
32.Santos AS, Arduini JB, Silva LC, Fonseca AS. Understanding of the elderly and their relatives regarding sexuality and HIV/AIDS: a descriptive study. Online braz. J. nurs. (Online). 2014; 13(2):175-85. [cited in 2017 Mar 27] Available from: http://www.objnursing.uff.br/index.php/nursing/article/view/4326
33.Ferreira MM, Ferreira EF, Toledo C, Oliveira RAR. Relationship between physical activity and quality of life in the elderly. Fagoc Undergraduate and Postgraduate Scientific Notebook (Online). 2016; 1(2):9-15. [cited in 2017 Mar 02]. Available from: http://revista.fagoc.br/index.php/caderno/article/view/129
34. Carvalho CF, Bezerra A, Castro JR, Ceia Nascimento A, Pereira BM, Silva CC, et al. Sexuality and quality of life of the elderly of Grow – Live together network of Uberlândia – MG. E-RAC (Online). 2016 [cited in 2017 Mar 02]; 6(1):1-15. Available from: http://www.computacao.unitri.edu.br/erac/index.php/e-rac/article/view/705
35.Pereira KCR, Alvarez AM, Traebert JL. Contribution of sociodemographic conditions to the perception of quality of life in the elderly. Rev. Bras. Geriatr. Gerontol. (Online). 2011 [cited in 2017 Mar 02]; 14(1):85-96. Available from: http://revista.unati.uerj.br/scielo.php?script=sci_arttext&pid=S1809-98232011000100010&lng=pt
36.Ermel RC, Caramelo AC, Fracolli LA, Ortiz FVB, Zutin TLM, Gianini SHS et al. Contribution of sociodemographic conditions to the perception of quality of life in the elderly. Revista Eletrônica Acervo Saúde (Online). 2017; [cited in 2017 Mar 02] 9(2):1315-20. Available from: https://www.acervosaude.com.br/doc/REAS98.pdf
37.Lobo AJS, Santos L, Gomes S. Level of dependency and quality of life of elderly. Rev. bras. enferm. (Online). 2014 [cited in 2017 Mar 02]; 67(6):913-9. Available from: http://dx.doi.org/10.1590/0034-7167.2014670608