IMAGE 1: Cross-sectional mapping of the nursing diagnoses, according to NANDA-I, in patients' charts of an outpatient clinic specialized in wound treatment. Niterói, RJ, 2013.
ORIGINAL RESEARCH
Nursing diagnoses in ambulatory care for wound patients: cross-mapping
Fernanda Pessanha de Oliveira I, Rosimere Ferreira Santana II, Bruna de Paula Silva III, Jessica de Souza Carvalho Candido IV, Michelle Hyczy de Siqueira Tosin V, Beatriz Guitton Renaud Baptista de Oliveira VI
I
Doctorate in Nursing, Universidade Federal Fluminense, Niterói. Rio de
Janeiro, Brazil. E-mail:
fernandapessanh@hotmail.com
II
PhD in Nursing. Assistant Professor, Universidade Federal Fluminense.
Niterói, Rio de Janeiro, Brazil. E-mail: rosifesa@yahoo.com.br
III
Nurse graduated from Aurora de Afonso Costa Nursing School of the
Universidade Federal Fluminense (UFF). Niterói, Rio de Janeiro, Brazil.
E-mail: brunapaula@id.uff.br
IV
Nurse graduated from Aurora de Afonso Costa Nursing School of the
Universidade Federal Fluminense (UFF). Niterói, RJ, Brazil. E-mail:
jessicacandido88@yahoo.com.br
V
Master in Nursing. Nurse in Neurological Rehabilitation. Universidade
Federal Fluminense. Rio de Janeiro, Brazil. E-mail: michellehyczy@gmail.com
VI
PhD in Nursing. Titled Professor, Universidade Federal Fluminense. Niterói,
Rio de Janeiro, Brazil. E-mail: beatrizguitton@globo.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.20028
ABSTRACT
Objective: cross-mapping of terms identified in wound patient medical records, by NANDA International (I) Classification nursing diagnosis. Method: this retrospective observational study, using cross-mapping in a sample of 81 records and 405 nursing progress reports on patients treated at a specialized wound clinic, was conducted in 2013 in two steps: descriptive terms in nursing diagnoses were mapped to the intersection with NANDA-I and related expert agreement was analyzed. Results: 309 descriptive terms corresponding to 19 NANDA-I diagnoses (3.7 ± 0.2), in seven areas of terminology, were mapped. The most common were Impaired skin integrity (20.4%) and Risk of impaired skin integrity (16.1%). Conclusion: cross-mapping identified the main nursing diagnoses in wound patients, indicating that it is possible to draft a clinical protocol to contribute to advanced nursing practice.
Keywords: Ulcer; wound healing; nursing process; nursing care.
INTRODUCTION
It is known that, currently, about 6.5 million people suffer from the direct and indirect consequences related to wounds1. These include pain, immobility and disability, which may impact self-esteem and self-image. Consequently, social changes may happen, resulting from hospitalizations and withdrawal from social life, which indicates the complexity of the latter, and is considered a public health problem 2-4. In addition, the burden suffered by the patient and the health system, which treats complications related to wounds, is worth more than US$ 25 billion per year in the United States1,5.
From this perspective, the importance of interdisciplinary actions in healthcare is recognized, in which the nursing care is inserted. Care is taken in the human integrality with the purpose of minimizing the bio-psychosocial impacts on the wounded patient. And, for this to happen, the clinical reasoning of the care nurse should transcend the search for signs and symptoms that will lead to diagnoses solely related to the presence or absence of tissue and skin lesions.
In this sense, the Systematization of Nursing Assistance (SNA) and the implementation of the five stages of the Nursing Process are based, respectively, on the organization of work and the clinical reasoning of the nurse6, in order to integrally articulate the health demands of the wounded patient. But for this care to be internationally recognized, it is recommended the use of a classification system for the standardization of the nursing vocabulary.
In the view of what has been exposed, the present study had the objective of cross-mapping the terms identified in the medical records of wounded patients, according to the NANDA International Nursing Diagnostic Classification (NANDA-I).
THEORETICAL REFERENCE
Being developed since 1973, the NANDA-I classification system defines a diagnosis as: the clinical judgment of the nurse on the response of an individual, family or community, based on health problems or actual or potential life processes that provide the basis for a therapy, which looks for achieving results. In other words, nursing diagnoses are the basis for the selection of actions or accurate interventions that aim at achieving results of improvement in the patient's health status6-8.
The need to consolidate care protocols focused on specific health problems and based on a language that represents nursing is still a necessary strategy to enable the SNA and the Nursing Process in the nurses' clinical practice.
However, there is, currently, a dearth of studies that, through the NANDA-I classification system, look for interrelating the inherent aspects of wounded patients. It should be emphasized that there are scientific publications that are specific to the context of women with wounds 9 or exclusively related to the diagnoses that refer to skin lesions10,11. There is also evidence that deal with the issue of wounds without, however, relating them to nursing diagnoses12,13.
METODOLOGY
A retrospective, quantitative, cross-sectional observational survey as a strategy that allows the comparison of the languages used in the daily life of healthcare services with the standardized classification systems 14.
In a university hospital in the city of Niterói-RJ, Brazil chosen as the scenario for this research, it was verified that in 2012, 190 patients with wounds were followed up in a specialized outpatient clinic for the treatment of this morbidity. Based on this population, the sample of medical records has been defined according to the following inclusion criteria: to be a patient older than 18 years old, with a wound of any etiology and presenting at least five nursing evolutions. Those that contained only phrases indicative of nursing interventions have been excluded. Thus, 81 medical records have been elected, of which 405 evolutions have been analyzed.
It is surmised that, in the charts evaluated in this research, there was no specific space to record the diagnoses, so the mapping has been done from the nursing evolutions. This corroborates, therefore, the strenuous task of analyzing the clinical reasoning of the nurse, who has described in a textual way what was considered by the researchers as descriptive terms indicative of nursing diagnoses.
Data collection was carried out by three researchers, from May to July of 2013; it happened through the completion of a form that was in a personal computer, and organized in three parts: data referring to the sociodemographic and health characteristics of the patient; complete transcription of the nursing evolutions from the medical record; fragmentation of the evolutions in order to highlight the terms related to the nursing diagnoses.
Sequentially, the research has been conducted in two stages: cross-mapping and concordance analysis among specialist nurses.
In the first stage, the search for the terms highlighted by the fragmentation of the evolution for the comparison according to the defining characteristics of NANDA-I 2012-2014 has been carried out, using as rules of the crossed mapping: map the context of the term and map the meaning of the words and not just words15. In a Microsoft Excel 2010 software spreadsheet, the terms extracted from the medical records have been stored in the first column and, in the next column, the defining characteristics according to the NANDA-I Nursing Diagnostics Classification. The related factors and risk factors have been identified from related terms, synonyms or similar concepts that mainly reflected the changes caused by the pathophysiology of the underlying diseases.
Then, the standardized diagnoses have been submitted to the evaluation of four specialist nurses so they could analyze the agreement between the terms that have been recorded in the charts and the mapped NANDA-I diagnoses. The sample of the nurses was composed of two specialists in wounds and two in nursing diagnoses. This process happened through a consensus meeting among the experts, who obtained 100% agreement among the evaluators regarding the descriptive diagnoses, the defining characteristics and related risk factors, and the NANDA-I diagnoses.
This research has been submitted to the ethical evaluation with the number of Certificate of Presentation for Ethical Assessment 13452713.3.0000.5243 and has been approved under the Opinion No. 219.752, dated from 28/03/2013, to comply with the provisions of the Resolution No. 466/12 of the National Health Council.
RESULTS E DISCUSSION
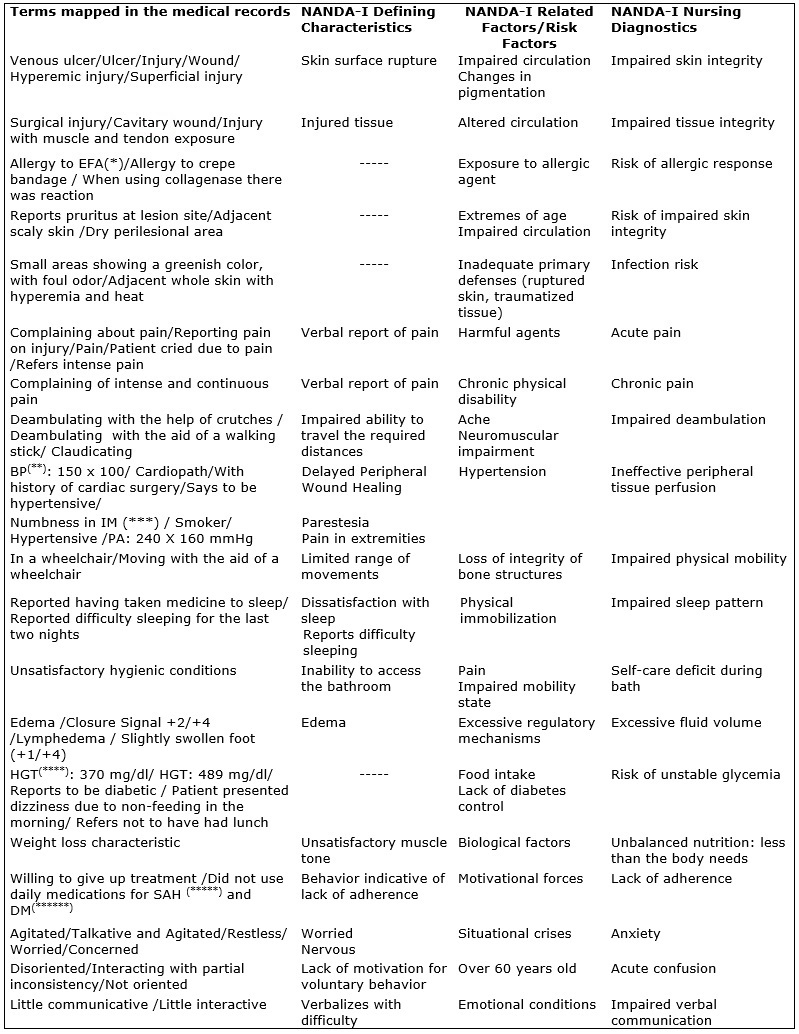
After the mapping of the 81 charts, 309 descriptive terms of nursing diagnoses have emerged, which, after the crossing with the NANDA Nursing Diagnostic Classification, have resulted in 19 nursing diagnoses according to Image 1. This represents the average of 3.8 (±0,2) nursing diagnoses by the analyzed medical records.
IMAGE 1:
Cross-sectional mapping of the nursing diagnoses, according to NANDA-I, in
patients' charts of an outpatient clinic specialized in wound treatment.
Niterói, RJ, 2013.
It is noteworthy that, for the mapping of the Impaired Skin Integrity and the Impaired Tissue Integrity diagnoses, the skin layer has been compromised as a discriminatory criterion3, in view of the similarities between the defining characteristics of both. Thus, the registry of the records describing the involvement of the epidermis alone have been mapped as Impaired Skin Integrity, while those that portrayed the involvement of subcutaneous and muscular tissue have been mapped as Impaired Tissue Integrity.
The methodological limitation of this study is acknowledged; it retrospectively analyzed nursing records from different professionals who work in an outpatient clinic specialized in the treatment of wounds in a university hospital. However, it was possible to minimize the limiting impact, since the cross-mapping has been performed based on clear and objective rules of analysis between the descriptive terms and the defining characteristics and related risk factors of NANDA-I. In addition, it should be highlighted that this institution seeks to comply with the recommendations of the SNA for the implementation of the Nursing Process, which provides some standardization of the nurses' clinical reasoning.
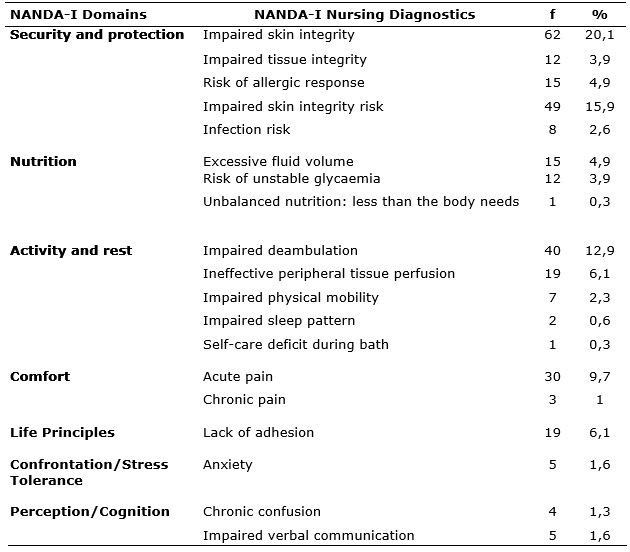
The diagnoses have been organized according to NANDA-I domains, as shown in Table 1. It is observed that the domain Security and Protection predominated with 47.4%; and mapped diagnoses, followed by the Activity at Rest domain with 22.2%. The most prevalent diagnoses were Impaired Skin Integrity (20.1%), Impaired Skin Integrity Risk (15.9%) and Impaired Deambulation (12.9%).
TABLE 1:
Nursing domains and diagnoses, according to NANDA-I, mapped in medical
records of outpatient patients specialized in wounds. Niterói, RJ, 2013.
(N=309)
The results of this research show the magnitude of nursing actions in the context of wounded patients, since the presence of diagnoses distributed in seven of the 13 NANDA-I domains is observed.
It is evident that patients with wounds presented with priority the nursing diagnoses related to the tissue and skin lesions, as it has been observed in this research. However, it should be noted that these diagnoses impose limitations on patients in several areas of life and on the health-disease continuum3. This indicates the need to instrumentalize the nurses so they can search for clinical evidence that considers the bio-psychosocial and economic aspects of the patient.
In this study, this reality has been observed through the mapping of diagnoses such as Anxiety, Chronic Confusion, Lack of Adhesion, Deficit in Self-Care for Bath, Impaired Verbal Communication and Impaired Sleep Pattern. However, the reduced percentage of these diagnoses leads to a reflection on the need to systematize healthcare through the implementation of clinical protocols based on the integrality of care.
Thus, in line with the world trend, the results of this study intend to elicit advanced nursing practice, based on the implementation of concrete strategies based on specialized and humanistic knowledge, acquired through the development of skills and competences in specific areas to the professional performance14.
Regarding diagnoses directly related to the context of wounds, it is observed that Impaired Skin Integrity and Impaired Tissue Integrity are broad diagnoses, since they have been mapped through the variability of signs and symptoms. This demonstrates the importance of analyzing the defining characteristics in the clinical context of the nurses' performance, in order to determine accurate diagnoses that will enable assertive interventions and, consequently, to promote satisfactory results 7.
The diagnosis Risk of Impaired Skin Integrity, mapped by signs and symptoms such as pruritus and scaling in the areas adjacent to the wounds, shows that the performance of the nurse specialist in wounds, besides looking for a treatment, also aims at preventing the worsening or the appearance of new lesions.
Also, in the treatment context, the multiplicity of primary coverage reveals the need for the clinical reasoning of the specialist nurse who, after evaluation, will indicate the most adequate coverage for each stage of the healing process. In this context, the replacement of the dressing applied to the lesion confers the risk of developing hypersensitivity to the product15. Thus, it justifies the need for periodic nursing appointments, in which the application of the stages of the nursing process will enable continuous reevaluations in order to identify changes in responses16. It becomes evident, due to the presence of the diagnosis of Allergic Response Risk and Risk of Infection, for which the breakdown of the skin barrier is already an indication of risk17 , revealing once again the importance of health surveillance skills, in which the nurse, through the implementation of the stages of the nursing process, is capable of promoting health, preventing and treating complications and rehabilitating patients in the different scenarios of their professional activity16.
Thus, identifying the interrelationship of the diagnoses Impaired Deambulation and Ineffective Peripheral Tissue Perfusion, as factors directly related to skin problems8, points, once again, to the contextual complexity. It happens due to the presence of wounds in the lower limbs, which is closely linked to circulatory deficits, which will motivate changes in mobility4. It is known that these are more common in the elderly18, often with comorbidities such as diabetes mellitus and systemic arterial hypertension8, which contribute to deficits in the blood supply of the peripheral regions, frequently identified in patients with wounds12,13.
In the same way, the diagnoses Chronic Pain and Acute Pain, very prevalent in patients with wounds3, are recognized as those that contribute to the appearance of other manifestations such as: fatigue, sleep disorders, stress, limitations to daily life activities and sense of worthlessness9. Endorsing, once again, the complexity of the clinical reasoning of nurses who, for the success of the wound treatment, will need to have a broad and personalized view, based, above all, on the integrality of care.
The Excessive Liquid Volume diagnosis, identified by the presence of edema in the lower limbs as a defining characteristic, related to chronic venous insufficiency, is closely associated with the presence of venous ulcers 19. The recognition of this diagnosis becomes important for the determination of the intervention that will be used, through compressive therapies and the elevation of the lower limbs, in order to potentiate the healing through the favoring of the venous return20.
CONCLUSION
The retrospective data collection from not always complete records of different professionals in customer records is a methodological limitation intrinsic to the cross-mapping. However, it is recognized that these are initial studies that may contribute to the advancement of scientific knowledge in specific areas of professional performance in what refers to the implementation of the nursing process based on terminology
The results of this research show that 309 denotative terms of nursing diagnoses have been cross-mapped with 19 diagnoses belonging to seven NANDA-I domains.
The most frequent nursing diagnoses were Impaired Skin Integrity and Impaired Skin Integrity Risk. Although these are directly related to wounds, the presence of diagnoses in different domains of NANDA-I and their interrelationships point to the need for integral care in healthcare delivery, based on the systematized clinical protocols and based on a terminology of the nursing language and complete records. Thus, it becomes possible to translate the nursing approach, which will result in improved quality of the healthcare and professional prestige, preventing underreporting, disseminating innovative knowledge, promoting health products and technologies that will contribute to an advanced nursing practice.
REFERENCES
1.Wong VW, Gurtner GC. Tissue engineering for the management of chronic wounds: current concepts and future perspectives. Exp Dermatol. 2012; 21(10): 729-34.
2.Charlesworth B, Pilling C, Chadwick P, Butcher M. Dressing-related trauma: clinical sequelae and resource utilization in a UK setting. Clinicoecon Outcomes Res. 2014; 28(6): 227-39.
3.Soares PPB, Ferreira LA, Gonçalves JRL, Zuffi FB. Impacto das úlceras arteriais na qualidade de vida sob a percepção dos pacientes. Rev Enferm UFPE. 2013; 7(8): 5225-31.
4.Lara MO, Pereira Júnior AC, Pinto JSF, Vieira NF, Wichr P. Significado da ferida para portadores de úlceras crônicas. Cogitare Enferm. 2011; 16(3): 471-7.
5.Zaho G. Delayed wound healing in diabetic (db/db) mice with Pseudomonas aeruginosa biofilm challenge – a model for the study of chronic wounds. Wound Repair Regen. 2010; 18(5): 467-77.
6.Conselho Federal de Enfermagem (Br). Resolução COFEn 358/2009. Dispõe sobre a sistematização da assistência de enfermagem e a implementação do processo de enfermagem em ambientes, públicos ou privados. Brasília (DF): COFEn; 2009.
7.Campos DM, Tosin MHS, Blanco L, Santana RF, Oliveira BGRB. Diagnósticos de enfermagem sobre alterações urinárias na doença de parkinson. Acta Paul Enferm. 2015; 28(2): 190-5.
8.NANDA Internacional. Diagnósticos de Enfermagem da NANDA: definições e classificação 2012-2014. Tradução de Regina Machado Garcez. Porto Alegre (RS): Artmed; 2012.
9.Lima MSFS, Carvalho ESS, Silva EA, Silva Gomes WS, Passos SSS, Santos LM. Diagnósticos de enfermagem evidenciados em mulheres com feridas crônicas. Rev Baiana Enferm. 2012; 26(3): 585-92.
10.Cavalcante AMRZ, Moreira A, Azevedo KB, Lima LR, Coimbra WKAM. Diagnóstico de enfermagem: integridade tissular prejudicada identificado em idosos na estratégia de saúde da família. Rev Eletr Enf. 2010; 12(4): 727-35.
11.Ribeiro MA, Lages JS, Lopes MH. Diagnósticos de enfermagem relacionados à pele: definições operacionais. Rev Latino-Am Enfermagem. 2012; 20(5): 863-72.
12.Rodrigues ALSR, Oliveira BGRB, Futuro DO, Secoli SR. Efetividade do gel de papaína no tratamento de úlceras venosas: ensaio clínico randomizado. Rev Latino-Am Enfermagem. 2015; 23(3): 458-65.
13.Oliveira BGRB, Castro JBA, Granjeiro JM. Panorama epidemiológico e clínico de pacientes com feridas crônicas tratados em ambulatório. Rev enferm UERJ. 2013; 21(esp.1):612-7.
14.Zanetti ML. Prática avançada de enfermagem: estratégias para formação e construção do conhecimento. Rev Latino-Am Enfermagem. 2015; 23(5): 779-80.
15.Frade MAC, Coutinho Netto J, Gomes FG, Mazzucato EL, Andrade TAM, Foss NT. Curativo de biomembrana vegetal e hipersensibilidade. An Bras Dermatol.2011; 86(5): 885-91.
16.Poortaghi S, Salsali M, Ebadi A, Rahnavard Z, Maleki F. Findings from a nursing care audit based on the nursing process: a descriptive study. Nurs Midwifery Stud. 2015; 4(3): e30181.
17.Ercole FF, Franco LMC, Macieira TGR, Wenceslau LCC, Resende HIN, Chianca TCM. Risco para infecção de sítio cirúrgico em pacientes submetidos a cirurgias ortopédicas. Rev Latino-Am Enfermagem. 2011; 19(6): 8 telas.
18.Freitas MC, Pereira RF, Guedes MVC. Diagnósticos de enfermagem em idosos dependentes residentes em uma instituição de longa permanência em Fortaleza-CE. Cienc Cuid Saude. 2010; 9(3): 518-26.
19.Trayes KP, Studdiford JS, Pickle S, Tully AS. Edema: diagnosis and management. Am Fam Physician. 2013; 88(2): 102-10.
20.Abreu AM, Oliveira BGRB. Estudo da bota de unna comparado à bandagem elástica em úlceras venosas: ensaio clínico randomizado. Rev Latino-Am Enfermagem. 2015; 23(4): 571-7.