ORIGINAL RESEARCH
Intra-hospital management of hazardous chemical waste handled by nurses
Taiza Florencio CostaI; Vanda Elisa Andres FelliII; Maritza Consuelo Ortiz SanchezIII; Simone Cruz Machado FerreiraIV; Zenith Rosa SilvinoV; Deise Ferreira de SouzaVI
I
Nurse. Ph.D. in Sciences. Professor, Universidade Federal Fluminense.
Brazil. E-mail: taizaflorencio@hotmail.com
II
Nurse. Ph.D. in Nursing. Senior Professor, Universidade de São Paulo.
Brazil. E-mail: vandaeli@usp.br
III
Nurse. Ph.D. in Nursing. Professor, Universidade Federal Fluminense.
Brazil. E-mail: morsa_peru@yahoo.com
IV
Nurse. Ph.D. in Nursing. Associate Professor, Universidade Federal
Fluminense. Brazil. E-mail: s.cruz.ferreira@uol.com.br
V
Nurse. Ph.D. in Nursing. Full Professor, Universidade Federal Fluminense.
Brazil. E-mail: zenithrosa52@gmail.com
VI
Nurse. Ph.D. in Health Care Sciences. Professor, Universidade Federal
Fluminense, Brazil. E-mail: dfsnit@hotmail.com
VII
Thanks to the Coordination for the Improvement of Higher Education
Personnel, who supported the research
Human resource management in Nursing in assistance, ethic, political,
and financing context at general public teaching hospitals in the
municipality of São Paulo.
Universidade de São Paulo, 2014.
DOI: https://doi.org/10.12957/reuerj.2018.19376
ABSTRACT
Objective: to evaluate the stages in management of hazardous chemical waste handled by nursing staff. Method: in this descriptive study, data was collected from September to December 2012 at São Paulo University Hospital, by applying the Hazardous Chemical Waste Management Information Sheet for formaldehyde and ortho-phthalaldehyde waste in the obstetric center and endoscopy, respectively. The study was approved by the research ethics committee. Results: data analysis showed that 3 (13%) of the 23 (100%) required specifications were met, predominantly identification, followed by segregation, and that none on internal waste transportation were met. The institution needs to comply with general identification specifications regarding the total number of evaluations of formaldehyde and orthophthaldehyde waste containers. Conclusion: this study also yielded important guidelines for preparation of the hospital care Hazardous Chemical Waste Management Plan.
Descriptors: Nursing work; chemical waste; occupational health; environmental health.
INTRODUCTION
The use of chemical products in hospital attention brings out substantial benefits to the population as well as serious concerns as to the generation of hazardous chemical waste (HCW), since shortcomings in its management can bring forth damage to human and environmental health.
Management of hazardous chemical waste (MHCW) comprises intra and extra health facility-related management steps. Intra-hospital steps concern segregation, packing, identification, inner transportation, and storage in waste shelters.
The concern in this research ranges from segregation up to inner transportation, since such steps are central to the success of the remaining ones in the process, including those of extra hospital nature. In that context, assessing HCW management implies the concern with whether or not nurses' activities may harm their health. Thus, attention is required to bring down workplace hazards1.
Resolution no. 306/2004 of the Board of Directors of the National Agency of Sanitary Surveillance (ANVISA) provides for the Technical Rules to Waste Management of Health Services and lays down that each and every waste generator of health services must make a Management Plan for Health Services Waste (MPHSW), including the HCW belonging in the group of chemical waste (CW) known as B Group. Management of HSW is regarded as the management action of waste insofar as its intra and extra facility aspects are concerned, from generation to final disposal. The following intra-hospital steps are included as follows2: Segregation: it is the sorting out of waste at the time and place of generation; Packing: it consists of packing the waste sorted out; Identification: it is the measures that allow for the identification of the waste. Thus, the B Group is identified by the risk symbol associated with it; Inner transportation: it consists of waste transportation from generation points up to the place meant for outer or temporary storage.
Formaldehyde and orto-phtalaldehyde stand out among the hazardous chemical waste consumed in hospital environment. Proper management of the waste generated by health facilities is crucial to health promotion, quality of living, and environmental preservation3. Thus, this research has aimed at assessing the steps to formaldehyde and orto-phtalaldehyde management – HCW handled by Nursing.
LITERATURE REVIEW
As a conserving, disinfecting, and sterilizing agent to human tissue, formaldehyde becomes one of the HCW and, if handled unsafely at any of the management steps, it can be absorbed by oral, skin, and inhaling passages in view of its active principle. It may show high levels of irritability to the eye mucous and breathing tract, causing possible cell harm leading to carcinogenicity. It also aggravates damages to wildlife4,5.
Orto-phtalaldehyde is a high level disinfecting agent, developed for the reprocessing of heat-sensitive odonto-medical and hospital articles. It replaces glutaraldehyde, as it is dialdehyde with proven action against vegetative micro life, B and C hepatitis virus, and in special, against heat-resistant and glutaraldehyde resistant micro bacteria.
Whether in product form or whether in waste form, orto-phtalaldehyde can cause skin sensitiveness, eye and breathing irritation, and it can harm the environment, calling for careful handling of both product and waste 6.
In this context, upon considering the relevance of intra-hospital HCW of formaldehyde and orto-phtalaldehyde handled by Nursing this research has aimed at the assessment of the compliance of the Technical Rules to Management of Health Services Waste by means of the items found on the Information Form to the Management of Hazardous Chemical Waste in Hospitals (IFMHCW-HOSP) 7 That form was generated from the data analysis in the dissertation entitled Management of hazardous chemical waste handled by Nursing at a teaching University Hospital, which evinced Nursing's ignorance of the MHCW generated upon patient's assistance.
Still, the same research has identified an existing gap between product directions for use and safety information on how to go about waste, a fact observed even on products with a Safety Information Form for Chemical Products7.
METHODOLOGY
This is a quantitative and descriptive piece of research whose central aim is the assessment of management of segregation, packing, identification, and inner transportation steps to two types of HCW. The research was conducted at the Teaching Hospital at the Universidade de São Paulo. (HU-USP) It involved the HCW of formaldehyde and orto-phtalaldehyde respectively generated at the Obstetric and the Endoscopy Center. Data collection made use of an IFMHCW-HOSP7, concerning the MHCW on the intra-hospital level. The research has been approved by the Committee on Research Ethics of the HU-USP nº 1183/12, under the Certificate of Presentation to Ethics Appreciation (CAAE) nº 0132.0.196.198-11. Collection in the HCW containers allowed for skipping the signing of the Free and Informed Consent (TCLE). Data were collected from September to December, 2012, totaling 16 assessments.
Upon data collection, by means of the IFMHCW-HOSP, formaldehyde and orto-phtalaldehyde were assessed as for the directions recorded on the CW collectors stored in the outer waste shelter. Stability, corrosivity, reactivity, toxicity, environmental information, active principle, classification, segregation directions, packing, identification, and inner transportation were assessed. Data were systemized, entered on database, put through statistic analysis, and shown on tables according to absolute and relative frequency.
RESULTS AND DISCUSSION
Upon assessment of the intra-hospital management system of formaldehyde and orto-phtalaldehyde waste, on the basis on the IFMHCW-HOSP, compliance to 3 (13%) out of 23(100%) necessary standards was evinced (eight standards on segregation and packing steps; 11 on general identification on the collector, and four standards on inner transportation) to proper management of the 132 liters of orto-phtalaldehyde waste generated monthly out of endoscopy, and 75 liters of formaldehyde waste out of the surgical center.
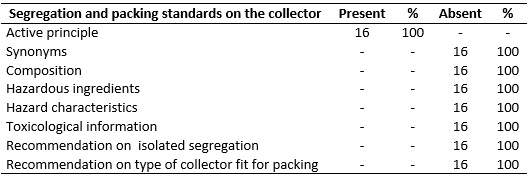
Over the 16 assessments observed on the segregation and packing steps, just 1 (12.5%) standard, out of the eight (100%) on the waste collectors met the directions on the IFMHCW-HOSP, represented by the information on the active principle on the label of the CW pack; the remaining ones were not met, as shown on Table 1.
TABLE 1:
Segregation and packing standards concerning total number of assessments on
waste containers of formaldehyde and orto-phtaladehyde. Brazil, 2012.
(N=16)
Data evinced that segregation and packing of the HCW under analysis are on-going, which turns out to be a positive factor; however, there appear non-compliances as for the mandatory information, such as synonyms, waste composition, hazardous ingredients, hazard characteristics, toxicological information, directions as for its isolation from other waste (directions for isolated segregation), and the compatibility with the collector (direction as for the type of collector fit for packing).
According to technical norm P4.262, of the Environmental Company of the São Paulo State (CETESB), HCW segregation must be predicted upon its generation, according to its classification and final destination 8.
Liquid waste must be packed in collectors made with material compatible with the waste generated; it must still meet endurance and hardness standards, and must be isolated, having a sealant screw2,9,10.
CW such as glutaraldehyde and other aldehydes such as orto-phtalaldehyde must be segregated, stored in hard plastic containers, identified and assessed as to incineration directions at chemical plants with an environmental license for that practice11.
Research shows that a few factors are associated to inefficiency on segregation, such as the lack of collectors adequate to waste disposal, and deficient training of professionals dealing with waste segregation at generation point12,13.
Research usually dwells more strongly on the segregation step of the HSW according to physical, chemical, and biological characteristics, risks involved and their physical status, since the other steps depend on the sorting out of the waste at time and place of generation7. Despite the emphasis found in research on the waste segregation step, shortcomings at that step generate the mix of different waste with disinfecting waste14.
There have been reports showing that many health institutions in several countries, there is no segregation of infecting, flammable, and toxic waste, and other material which requires special handling. Additionally, there is lack of identification, of collectors, of carts for inner transportation, and inner waste shelter15-17.
This way, research is likely to approach HCW in a general way among infecting and piercing-cutting waste.
Because of risks, chemical products must be segregated as the HCW whenever the following can be observed: change in temperature, expiration, accidental rupture, interdiction to use, illegible identification, loss of seal, which might compromise the product, alteration of color, and/or presence of an alien body.
This research still allowed for observing the HCW segregation instances the institution encompasses, that is, basically expired and/or contaminated medicine, chemotherapeuticals, glutaraldehyde, formaldehyde, and xylol, all of which usually handled by Nursing7. Segregation of o rto-phtalaldehyde, as a substitute for glutaraldehyde, requires specific care on account of its hazardousness.
Research on the Plan for Waste Management from Health Services at hospital units in the Metropolitan Region of the Lowlands in Santos evinced that Group B waste, in most part, was represented by either expired or non-utilized medicine18.
In quite a few places, a do-or-die behavior comes upfront: either all waste is segregated as hazardous or none is sorted out19.
As for the HCW packing, the MPHSW showed the HU-USP has adopted the orange CW plastic collector in hard polyethylene, resistant to perforations on any of the points on its surface, with a screw cap that ensures efficient closing and risk symbology7.
The same research reports that at the outer shelter for the HCW, the orange collector is prevailingly used for packing medicine bottles, as antibiotics, besides bottles, syringes, needles, and other material derived from assistance to patients treated with anticancer agents; remarks are still made that formaldehyde and orto-phtalaldehyde waste was packed in the original product pack6.
As for waste volume, there is a series of relevant data related to the management of hospital HSW, with special emphasis on the quantity of waste generated by means of weighing before disposal20.
The MPHSW of the same institution in this research shows HCW segregation records from 2001 to 2006. Still on the same Plan, assistance sectors are reported as the generating places for HCW handled by Nursing, in addition to Pharmacy and pathologic anatomy services, clinic lab, blood center, maintenance, specialized hygiene service, and audiometry7.
This research also confirms the segregation of formaldehyde and orto-phtalaldehyde (substitute for glutaraldehyde), generated at both the obstetric center and the endoscopy service at the HU-USP.
Pieces of research have evinced that the quantity of HSW generated, including the HCW, varies according to hospital and assistance types. Knowledge of real quantities of waste generated is hard to determine and is seldom obtained. Therefore, estimated values are used, for the more complex the service, the higher the chances for production of high HSW volumes7,21-23.
The MPHSW must be elaborated on the basis of the characteristics and the volume of waste, as major indicators in management of hazardous waste, including for HCW.
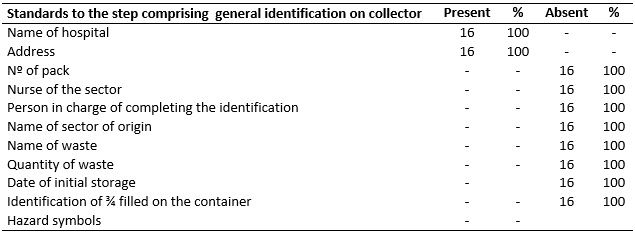
As for general identifications on waste collectors for the first 16 assessments, out of the 11(100%) standards on the referred step, just 2 (18.18%) met the requirements on the IFMHCW-HOSP, represented by the information name of hospital and address on the referred collectors, as shown on table 2:
TABLE 2:
Standards on general identification concerning the total number of
assessments on waste collectors of formaldehyde and orto-phtalaldehyde.
Brazil, 2012. (N=16)
Concerning identification of the HSW, it must be highlighted that it must be on the collectors for inner and outer collection, on the packing bags, on inner and outer transportation containers, and on storage places 2.
Characterization of collectors by means of colors and identification by symbols turns out to be a world-wide practice, with a prevailing packing of human tissues in red containers, of infecting and the piercing-cutting waste in yellow containers, and the remaining in orange containers. 24,25.
In Brazil, the infecting waste is packed in opaque white bags; the piercing-cutting waste in yellow boxes; and the chemical waste in orange collectors, all of which with their respective risk symbology7.
For waste identification, the realm institution in this research has a flyer called Waste Identification with information concerning the waste type, data of the generating institution, addressee, and symbology.
CW must be carefully identified on the container as for labeling corresponding to product name, physical and chemical properties, volume, packing date, hour, type of transportation, in addition to the hazard symbol which may identify hazard properties6,21,23.
This research finds that under information on container concerning general institutional data and inner transportation has effects especially on inner facility management and later on outer facility management.
Attention must be paid to Norms P4.262 by CETESB, CVS 21 by the Center of Sanitary Surveillance (ANVISA), and NBR 14725-2 by the Brazilian Association of Technical Norms (ABNT)7,24,26.
This research has shown that lack of information on the collector, concerning segregation and packing may compromise the remaining management, with special emphasis on treatment and final disposal.
In the 16 assessments of inner transportation, not one out of the 4 standards (100%) could be identified– date, hour, type of collector cart, and identification of the HCW.
For inner transportation, RDC Nº 306/2004 by ANVISA defined inner transportation as the transportation of waste from its generation point up to the inner or outer shelter2.
Physical and human resource-related difficulties often cause inner transportation of HSW to be conducted either by hand or with inadequate use of transportation cart16.
The inner transportation step must be represented on blueprint, attached to the MPHSW, favoring the identification of waste generation places by groups, their respective flows, from generation up to outer shelter.
Besides the lack of standard records on collectors and carts, the blueprint for inner transportation was also missing on the MPHSW of the HU-USP. Thus, comprehensive analysis of transportation flow adequacy for the HCW derived from the identified products failed to be made.
Blueprint, symbology, and color captions favor the drawing of the waste flow, making it easier to manage the HSW and subsidize the MPHSW21.
The use of the FIGERQP-HOSP at the institution in this study made it possible to assess the standards necessary to intra-hospital management of formaldehyde and orto-phtalaldehyde, handled by the Nursing of the Obstetric Center and Endoscopy Service.
CONCLUSION
By means of the IFMHCW-HOSP, this research has shown that the MHCW of formaldehyde and orto-phtalaldehyde displays a series of non-compliances with the standards for the management of segregation, packing, identification, and inner transportation of formaldehyde and orto-phtalaldehyde waste. Such non-compliances may bring forth several problems, among which detrimental effects over nursing workers' health as well as the environment.
However, it must be highlighted that major standards in the management of CW have been met by the realm institution in this research. The potential of the Committee for the Management of Health Services Waste of the HU-USP stands out. It has acted together with the general management of the institution as well as with the public agencies to conduct necessary adjustments to the compliance with the remaining standards to better both the labeling system on HCW collectors and the adequacy of the Hazardous Chemical Waste Management Plan, as part and parcel of the MPHSW.
REFERENCES
1.Carvalho EC, David HMSL. A aplicação da precaução e da prevenção no ambiente de trabalho. Rev. enferm. UERJ. 2016; 24(3):e26180.
2.Ministério da Saúde (Br), Agência Nacional de Vigilância Sanitária. Resolução da Diretoria Colegiada - RDC nº 306, de 07 de dezembro de 2004. Dispõe sobre o Regulamento Técnico para o gerenciamento de resíduos de serviços de saúde. Brasília (DF): ANVISA; 2004.
3. Governo Estadual (SP), Companhia Ambiental do Estado de São Paulo. Informações toxicológicas. FIT-Ficha de Informação Toxicológica [site de Internet]. São Paulo: CETESB; 2013 [cited 2017 Aug 28]. Available from: https://cetesb.sp.gov.br/laboratorios/servicos/informacoes-toxicologicas/
4.Coggon D, Harris EC, Poole J, Palmer KT. Extended follow-up of a cohort of british chemical workers exposed to formaldehyde. J. Natl. Cancer Inst. 2003; 95(21): 1608-15.
5.Felli VEA, Baptista PCP. Saúde do trabalhador de enfermagem . São Paulo: Manole; 2015.
6.Psaltikidis EM, Leichsenring ML, Nakamura MHY, Bustorff-Silva JM, Passeri LA, Venâncio SI. Desinfetantes de alto nível alternativos ao glutaraldeído para processamento de endoscópios flexíveis. Cogitare enferm. Rev. 2014; 19(3):465-74.
7.Costa TF, Felli VEA, Baptista PCP. A percepção dos trabalhadores de enfermagem sobre o manejo dos resíduos químicos perigosos. Esc. Enferm. USP. 2012; 46(6):1453-61.
8. São Paulo (Estado), Companhia Ambiental do Estado de São Paulo. Norma técnica P4.262, de agosto de 2007. Dispõe sobre o gerenciamento de resíduos químicos provenientes de estabelecimentos de serviços de saúde [site de Internet]. São Paulo: CETESB; 2007 [cited 2017 Oct 30]. Available from: https://www.cetesb.sp.gov.br/wp-content/uploads/2013/11/DD_224_DO.pdf
9.Ministério do Trabalho e Emprego (Br). Norma Regulamentadora nº 32, de 11 de novembro de 2005. Dispõe sobre a segurança e saúde no trabalho em serviços de saúde. Brasília: Gabinete Ministerial; 2005.
10.Lei nº. 12.305 de 2 de agosto de 2010. Institui a Política Nacional de Resíduos Sólidos; altera a Lei nº. 9.605, de 12 de fevereiro de 1998; e dá outras providências. Diário Oficial da União [site de Internet]. 3 ago 2010 [cited 2017 Aug 05]; Seção 1. p. 3. Available from: http://www.planalto.gov.br/ccivil_03/_Ato2007-2010/2010/Lei/L12305.htm
11.Felli VEA, Costa TF, Baptista PCP, Guimarães ALO, Anginoni BM. Exposição dos trabalhadores de enfermagem às cargas de trabalho e suas consequências Rev. Esc. Enferm. USP. 2015; 49(esp 2):98-105.
12.Bdour A, Altrabsheh B, Hadadin N, Al-Shareif M. Assessment of medical wastes management practice: a case study of the northern part of Jordan. Waste Manag. 2007; 27(6):746-59.
13.Oweis R, Al-Widyan M, Al-Limoon O. Medical waste management in Jordan: a study at the King Hussein Medical Center. Waste Manag. 2005; 25(6):622-5.
14.Ferreira V, Teixeira MR. Healthcare waste management practices and risk perceptions: findings from hospitals in the Algarve region, Portugal. Waste Manag. 2010; 30(12):2657-63.
15.Tudor TL, Woolridge AC, Phillips CA, Holliday M, Laird K, Bannister S, et al. Evaluating the link between the management of clinical waste in the National Health Service (NHS) and the risk of the spread of infections: a case study of three hospitals in England. Int. J. Hygiene Environ. Health. 2010; 213(6):432-6.
16.Soysal A, Simsek H, Soysal D, Alyu F. Management of health-care waste in Izmir, Turkey. Ann. Ist. Super Sanita. 2010; 46(3):299-302.
17.Tsakona M, Anagnostopoulou E, Gidarakos E. Hospital waste management and toxicity evaluation: a case study. Waste Manag. 2007; 27(7):912-20.
18.Costa AMP. Elaboração e avaliação da implantação de um modelo básico de plano de gerenciamento de resíduos de serviços de saúde em unidades hospitalares da Região Metropolitana da Baixada Santista [dissertação de mestrado]. São Paulo: Universidade de São Paulo; 2001.
19.Garcia LP, Zanetti-Ramos BG. Gerenciamento dos resíduos de serviços de saúde: uma questão de biossegurança. Cad. Saúde Pública. (Online)2004;20(3):744-52.
20.Jang YC, Lee C, Yoon OS, Kim H. Medical waste management in Korea. J. Environ. Manage. 2006; 80(2):107-15.
21.Bendjoudi Z, Taleb F, Abdelmalek F, Addou A. Healthcare waste management in Algeria and Mostaganem department. Waste Manag. 2009; 29(4):1383-7.
22.Sales JEY, Silva EB. Guia de descarte de produtos químicos perigosos de laboratório. São Paulo: UNESP; 2016.
23.Takayanagui AMM. Risco ambiental e o gerenciamento de resíduos nos espaços de um serviço no Canadá: um estudo de caso [tese de livre docência]. Ribeirão Preto (SP): Universidade de São Paulo; 2004.
24.Secretaria de Estado da Saúde (SP). Centro de Vigilância Sanitária. Portaria CVS nº 21, de 10 de setembro de 2008. Aprova a Norma Técnica sobre Gerenciamento de Resíduos Perigosos de Medicamentos em Serviços de Saúde. São Paulo: Centro de Vigilância Sanitária; 2008.
25.Oliveira LL, Souza PM, Clementino FS, Paiva SC, Rocha FDLJ. Resíduos dos serviços de saúde: desafios e perspectivas na atenção primária. Rev. enferm. UERJ. 2014;22(1):29-34.
26.Associação Brasileira de Normas Técnicas. NBR 14725-2: Produtos químicos: informações sobre segurança, saúde e meio ambiente: parte 2: sistema de classificação de perigo. Rio de Janeiro: ABNT; 2009.