ORIGINAL RESEARCH
Coping strategies adopted by women victims of violence
Laís CostaI; Rayane Gonçalves LordesII; Dherik FragaIII; Nathália Miguel Teixeira SantanaIV; Susana BubachV; Franciéle Marabotti Costa LeiteVI
I
Nurse. Federal University of Espírito Santo, Graduate Program in Nursing.
Brazil. E-mail: lais.costa87@hotmail.com
II
Nurse. Federal University of Espírito Santo, Graduate Program in Nursing,
Brazil. E-mail: rayane_lordes@hotmail.com
III
Master student in Nursing. Federal University of Espírito Santo, Graduate
Program in Nursing. Brazil. E-mail: dherik@msn.com
IV
Master in Collective Health. Federal University of Espírito Santo, Graduate
Program in Collective Health. Brazil. E-mail:
nathalia.miguel@hotmail.com
V
PhD in Epidemiology. Federal University of Espírito Santo, Norte do
Espírito Santo University Center. ES, Brazil. E-mail: sbubach@gmail.com
VI
PhD in Epidemiology. Federal University of Espírito Santo, Graduate Program
in Nursing, Vitória, ES, Brazil. E-mail:
francielemarabotti@gmail.com
DOI: https://doi.org/10.12957/reuerj.2018.19334
ABSTRACT
Objective: to examine the coping strategies adopted by women victims of violence. Method: in this quanti-qualitative, descriptive study of 19 women victims of violence, who attended the Multidisciplinary Support Center in Serra, Espírito Santo, in 2013, semi-structured interview and recording were used to collect socioeconomic and violence data. Content analysis was applied to the testimonies. The study was approved by the research ethics committee. Results: the women were predominantly aged 39 years or less, had completed secondary education, had their own income, a family income of 1 to 2 minimum wages, and were Evangelicals. The themes recovered from their accounts were: combating violence by focusing on the problem (42.1%), combating violence by focusing on emotion (26.3%), combating violence by focusing on emotion and religion (21.1%), and combating violence by focusing on emotion and the problem (10.5%). Conclusion: women in situations of violence experienced different manners of coping with this disorder, by focusing on the problem, emotion and religion.
Descriptors: violence against women; psychological adaptation; women's health; nursing.
INTRODUCTION
Violence is defined as the intentional use of force or power through real threat or aggression against oneself, another person, or against a group or community, which results in or is likely to result in injury, death, psychological harm, development problems or deprivation1. This phenomenon is determined in the cultural tradition, social organization, economic structures and in power relations, being practiced against female persons, simply because of their condition of woman, causing a relation based on inequality, discrimination, subordination and abuse of power2.
Since the 1990s, violence against women has been recognized internationally as a public health problem, when it was no longer treated only as violence between spouses or as a private matter and started to be treated as a public health problem. In the world, one in six women suffers domestic violence, and in 60% of cases of violence is perpetrated by the husband or partner3.
In Brazil, the numbers are of violence against women are alarming; one in every five Brazilian women claim to have suffered some kind of violence by men. A study carried out in Vitória, Espírito Santo, showed that in the last year, about 25% of health service users have experienced psychological violence from the intimate partner, and approximately 10% have been victims of physical aggression4. The mortality rate of women victims of aggression has not decreased even after the approval of the Maria da Penha Law in 2007. The mortality rate per 100,000 women (victims of aggression) used to be 5.28 in the period between 2001 and 2006 (before the Law) and was 5.22 in the period between 2007 and 20115.
In the first aggression, women create a positive expectation that they will not suffer violence a second time, and then they do not make a formal complaint in the Women's Police Station6. In this sense, the victim of violence uses silence as a survival strategy in the attempt to prevent further episodes of fighting and conflicts in order to preserve the family7. However, when the victim finds her situation challenging, mobilization of confrontation efforts take place. This situation involves emotions such as excitement, hope and confidence8.
Thus, this article aimed to analyze the coping strategies adopted by women victims of violence to deepen the study of the phenomenon, and in this way, to increase the knowledge of the different paths taken by women in situations of violence, as well as of how to support the implementation of interdisciplinary interventions.
LITERATURE REVIEW
One in five Brazilian women claim to have suffered some form of violence perpetrated by men and at least 6.8 million have been beaten at least once. More than half of the victims do not seek help, and when they do, it is because they considered the situation as urgent, such as threats with firearms and spanking and little more than half of these victims ask for help, and when they do so, this is done by means of another family member or close friend9.
Coping with violence represents for them an attempt to exert some control over the environment and events in the attempt to facilitate a better adaptation to the situation8. It is worth pointing out that, among the strategies adopted, coping reveals distraction, positive reassessment about oneself, definition of limits, life plans and search for social support, especially when leaving the abusive relationship is not feasible10.
The experience of violence involves several feelings, often ambiguous and contradictory. Victimized women live with fear, anger, indignation, and surprise before their partners' aggressive reaction11. It is worth noting that most women remain in their relationships because they feel shame, or because of financial dependence on the aggressor, fear of loneliness, worry about providing for their children and sparing them from suffering, hope that violence will stop, and also because they have not family and social support12.
Besides these factors, women usually remain in violent relationships because they have experienced a family history where there was aggression among parents or people close to them, propitiating the repetition of this model in their own conjugal relationship. This is because they believe in the change of attitude of the husband/partner and/or believe in the inability to live without the husband/partner and without a father for the children13,14. In this context, women in situations of violence often use coping tools and strategies to deal with the problem.
Coping strategies used by women go through gender issues and socio-cultural contexts that, in a transversal way, permeate the meanings, the attitudes adopted and the forms of expression of violence against women that are directly related to the success or failure of the strategies used. Personal or social networks play an important role in the breakdown of violence15, because the help that a person receives from these networks, material resources, among other variables, influences how they assess a situation as stressful or not, and the choice that she will use to deal with the situation16.
METHOD
This is a descriptive study with a quantitative approach carried out at the Multidisciplinary Support Center (MSC) in Serra, Espírito Santo, which assists Family cases, and cases of Domestic and Family Violence against Women. The MSC team consists of four social workers and two psychologists. Qualitative research apprehends the complexity of the phenomenon, bringing to the analysis the subjective and objective aspects of social subjects, according to their worldviews17.
The participants of the study were 19 women victims of violence referred to the MSC, after opening a report in the Police Department of Assistance to Women in the municipality of Serra, in 2013. The inclusion in the study was random and based on the criterion of data saturation, that is, recidivism of information18. Sampling based on saturation is a conceptual tool commonly used in qualitative research in different areas in the Health field. It is used to establish the final sample size in studies, ending data collection when new components cease to appear19.
Women who were in the waiting room, in the order of arrival at the service, were invited to participate in the study. Data were collected at the MSC rooms from November 2012 to July 2013. The inclusion criteria were: women with age above 18 years and who had suffered some type of violence.
Before starting the research, the women were informed about the objectives of the research by reading the Informed Consent Term (ICT). Before accepting it, their signature was requested and then the interviews started. In order to guarantee secrecy of information and anonymity of the participants the statements were codified by the letter I, in the results, referring to the word interviewee, and Arabic numerals, composing the codes I1, I2, I3, I4, according to the sequence in which they were interviewed.
Data were obtained through an interview script with questions of characterization of the participants (age group, educational level, own income, family income, and religion) and an open question about the coping strategies adopted, taking into account the guiding question of the study: When you began to suffer violence, how did you sought to cope this situation? The interview took place in a reserved room, after the working the multidisciplinary team had assisted the women so as not to disturb the flow of the service.
The testimonies were recorded and transcribed verbatim. Treatment of the data occurred by content analysis, composed of three stages: pre-analysis; exploitation of the material and treatment of results; and interpretation 20. The first stage consists of the organization phase, using the method of quick reading; in the second step, data were encoded into the record units; and in the third stage, categorization and classification of the elements was done according to their similarities and differences, and then reunited, according to common characteristics19. Thus, four categories emerged: confrontation violence with a focus on the problem; Confrontation with violence focused on emotion; Coping with violence focused on emotion and religion; and Coping with violence focused on emotion and the problem.
In the quantitative approach, statistical methods were applied, by presenting the absolute and percentage frequency of socio-demographic variables of the participants (in table) and of the thematic categories.
The research project of this study was sent to the Research Ethics Committee of the Federal University of Espírito Santo (UFES) and was approved under Opinion number 195,469.
RESULTS AND DISCUSSION
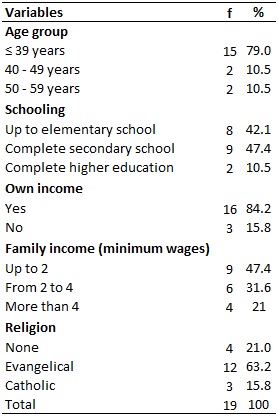
The attributes of the women - age group, education level, individual and family income and religion were analyzed, as shown in Table 1.
TABLE 1:
General characteristics of the victims of violence participating in the
study. Serra, Espírito Santo, 2013.
From the 19 eligible women, it was observed that 15 (79.0%) were aged 39 years or more. A documentary study carried out in Ribeirão Preto also found that the majority of women victims of domestic violence (56.2%) were in the age range between 20 and 39 years21. The prevalence of aggression among young women may occur due to cultural patterns: a beautiful body arouses attention and may provoke in some men insecure and violent authoritarian practices, explaining the predominance of the occurrence of aggression22.
As to schooling, nine participants (47.4%) had completed secondary education, contrary to the observed in other studies in which the majority of the victims of violence presented low level of schooling. A study carried out in Florianópolis exemplifies this relationship, as it identified the predominance of complete and incomplete Elementary Education among victims of violence15. Another research developed in Curitiba also found that 59.7% of women who had suffered all types of violence had incomplete Elementary Education23.
Most participants (84.2%) claimed to have their own income; nine (47.4%) had monthly family income of up to two minimum wages. Although women have low incomes, having their own income reduces their vulnerability to violence because lack of income, or lack of financial autonomy, can hinder decision-making when it comes to breaking up the violent relationship 24. Thus, income is an important tool in decision-making, to break the cycle of violence.
Regarding religiosity, 12 (63.2%) women said to be evangelical. According to an investigation conducted in Fortaleza, 80% of women victims of domestic violence were Catholic and only 11% declared themselves to be evangelicals25. It is worth noting that for evangelical women there is weakness in denunciations because their right to react before violence is understood as lack of faith in the divine promise of transformation of their husband26.
Women who are beaten often use coping strategies to survive the violent relationship within the family15. In the present study, when questioned about when they began to suffer violence, how they tried to cope with this situation, the following thematic categories were revealed: 8 (42.1%) were in the category of coping with violence focused on the problem; 5 (26.3%) presented reports in the category of coping with violence focused on emotion; 4 (21.1%) in coping with violence focused on emotion and religion; and 2 (10.5%) sought coping with violence focused on emotion and on the problem.
The model of coping strategies adopted27 involves four main concepts: coping as a process or interaction that occurs between the individual and the environment; its function is to manage the stressful situation, rather than to control and dominate the problem; these processes presuppose how the phenomenon is cognitively perceived, interpreted and represented in the mind of the subject; the confrontation process is a mobilization of efforts, in which subjects undertake cognitive and behavioral efforts to manage the situation, that is, reducing, minimizing or tolerating the internal or external demands arising from their interaction with the environment28.
Coping with violence focused in the problem
In the coping strategy focused in the problem, we perceived that there is an effort to change the situation experienced, changing the existing problem. This strategy aims to face the situation, and it is considered the most useful and directed to reality, with the objective of minimizing and/or eliminating the source of stress that in this case is the violence suffered29. These findings are evidenced in the statements of two interviewees:
I would try to tell him, or sometimes I said that I could call the police or something. I myself took attitude in everything. (I1)
I tried to talk. (I6)
Another method adopted by women to try to confront the situation was to react to violence. Research reveals that women's aggressions against their partners are considered mild, such as pushing and slaps, while those of men are more serious and violent30. This information was also revealed in this research:
Head down, never, never. Because I'm not a punch bag. If he wants to punch me, I'll go and punch him. It is a way for me to defend myself; if he hurts me, I will also hurt him [...]. (I5)
Women have difficulties in escaping domestic violence. It is only when they realize that all attempts and negotiations are exhausted and that violence can reach an extreme point that they go to confront the problem. The most effective denunciation can be obtained when women understand their vulnerability, the seriousness of the violence, and the benefits and the problems in making that decision12.
The intention of women to report the violence in a police station is based on the possibility of terminating the relationship with the partner, expressing the non-acceptance of the relationship that represents a problem31.
[...] I went to the woman's station [...]. (I8)
I tried to resolve the situation in court. I looked for help in the forum really. (E3)
[...] the only force I sought was the police. That's when I reported him to the Maria da Penha Law. (I2)
I asked the neighbors for help, my neighbor. I cried: 'Help, for God's sake, help me, he's going to kill me... Call the police, help me'. So, who was on my side? Neighbors to help me; I have neighbors who do not go because they are afraid, and called the police. (I10)
I sought help from friends who came to my house and they helped me. Please call the police, and so he was taken away by the police. (I4)
Coping with violence focused on emotion
The focus on emotion reveals strategies with high emotional load resulting from self-defense processes, triggering mechanisms of detachment, escape and avoidance that serve as a shield and avoid the confrontation of the individual with the stressor27.
I would always leave the house, always went to my mother's house. Every time I saw that he was very mad, I would go before he started to fight. (I9)
I would stay in my place, more in my place. I kept it for myself. (I7)
To confront him, I never took an attitude, I would stay on my own, I would stay still, would I confront a person in that state that he was? So that's what I told you, I kept quiet. (I14)
Sometimes I kept quiet; sometimes I left the house, sometimes I stayed at my father's house for a week. I know that, I mean, I tried to leave the house, to forget some of the torment. (I16)
Crying and sitting in the bedroom. (I13)
When focused on emotion, confrontation strategies attempt to replace or regulate the emotional impact of stress on the individual, stemming primarily from defensive processes, causing people to consciously avoid confronting the threatening reality32.
In emotion-focused coping strategies, the person focuses on relieving the emotions associated with the stressful situation, although the problem in itself is not resolved. The women try to prevent their negative emotions from dominating them and making them unable to react to solve their problems. This type of confrontation is also used when a conflict is uncontrollable25.
Coping with violence focused on emotion and religion
As previously pointed out, the emotion-focused confrontation modality is an indicative of the presence of emotional difficulties associated with negative emotions and avoidant behavior, pointing to difficulties in managing the situation33.
Religious practices and/or religiosity promote another meaning and personal strengthening in the life of the most penalized people, and this can cause greater involvement with their reality and search for solutions to everyday problems34. It is noted that this strategy has a relevant role in coping with violence. Belief in God, optimism and positive thinking influence the increase of adaptive responses to difficult situations, as presented in the participants' reports:
I would try to leave, I would run. I sought strength in God. (I11)
I avoided confrontation. Any situation that I saw that our idea was going to cause unrest, I'd let it go. I sought to go to the Church. (I15)
God was my psychologist, my friend, my helper. I was silent, I'd rather shut up to avoid violence. To avoid the issue of physical aggression, I was silent. (I12)
Violence perpetrated by the aggressor is counteracted by the power of prayer26. Certain women say that religion helps in the coping with violence and that through faith they can fight it, since faith will be a strengthening subsidy for reaction and fight against violence35.
I found refuge in God because I had no one to protect me. If I did not have much faith in God, I would not be alive now. I prayed to God a lot and trusted that I would get out of this situation. (I17)
Coping focused on emotion and on the problem
New models of confrontation can be learned36, as well as used and rejected. That means that persons can discard the resources they used and replace them with others more effective to cope with their problem. It is noted in the speeches that some participants of the research sought help to minimize the stress and suffering generated by the violence and sought solutions to the problem. They used what is called coping strategies focused on emotion and on the problem, according to the literature 30,36,37.
Until 1997, I would accept everything. Then, in 1998, I took the first initiative to report him. Then I went back and gave up the report. But now I have decided to continue reporting him, since January 2012. (I19)
A common characteristic among people who practice psychological violence against women is the ability to use children as targets every time they wish to affect the victim37.
I cried, cried, and wept. But I made my decision myself and went to the police, because now he started to threaten the children, not only me, he touched my children and this hurts me. When we were just the two of us, but he started to beat my children, so the story changed. (I18)
The data presented allow us to reflect on the importance of approaching violence against women as a complex phenomenon determined by relational, social, cultural, economic and gender stigma. Health professionals, in individual or collective approaches, should constantly promote debates about ethical issues, about the violation and the promotion of women's rights, allowing the construction of strategies that generate change in the conditions for confrontation, promoting health and citizenship15 .
The intervention in the structure and human resources in the health area can promote change and coping with violence. The inclusion of this content in the training of health professionals contributes to the development of knowledge and skills, reflective criticism, instrumentalizing professionals for collective and individual care. Furthermore, the reorganization of care services aimed at women victims of violence, coupled with the promotion of intersectoral actions, strengthens support networks and multidisciplinary teams38. In this scenario, health education, compulsory notification, as well as stimulating and promoting the women's access health services and their protection against domestic violence become paramount21.
CONCLUSION
Four categories emerged from the analysis of participants' speeches: Coping with violence focused on the problem, Coping with violence focused on emotion, Coping with violence focused on emotion and religion, and Coping with violence focused on emotion and on the problem.
It is perceived that women seek in some way to solve the violence, using as coping strategy the focus on the problem. For them, great effort is required to change the situation experienced. They use the support of family, friends, and public security. Otherwise, they seek internal forces for such confrontation.
Religion is a strategy that deserves attention. The religiosity in the life of women who are battered proved to be of great importance to face this problem. Believing in a superior force increases optimism and positive thinking and influences the responses to stressful situations. Another strategy observed, also adopted by the victims and evidenced in this study, is the use of self-defense, either distancing or escaping the problem.
Violence against women and deprivation from their rights as citizens cannot be considered as normal and need to be unveiled and discussed so as to eliminate this cycle. Public policies are needed to strengthen the existing social support networks.
Finally, the main limitations of this study were the small number of studies discussing ways of coping with violence adopted by women and the small sample studied which prevents the generalization of the results. In this research, only women who sought to break the cycle of violence were studied; thus, the coping strategies listed here refer to this particular group and not the countless victims who are unable to escape domestic violence.
REFERENCES
1. Krug EG, Dahlberg LL, Mercy JA, Zwi AB, Lozano R. World Report on Violence and Health. Rev. Inst. Vet. Trop. Sao Paulo [Online]. 2003 [cited 2017 May 06]; 45(3): 130. Doi: http://dx.doi.org/10.1590/S0036-46652003000300014
2.Oliveira RC, Cavalcanti ECT. Public policies to combat gender violence. Rev. periferia [Online]. 2017 [cited 2017 Dec 06]; 9(2): 121-38. Available from: http://www.e-publicacoes.uerj.br/index.php/periferia/article/view/28829/22114
3. World Health Organization [website]. Fundamental study on domestic violence [cited in May 03, 2017]. Available from: http://www.unric.org/en/women/5651
4.Leite FMC, Amorim MHC, Wehrmeister FC, Gigante DP. Violence against women in Vitória, Espírito Santo, Brazil. Rev. saúde pública [Online]. 2017 [cited 2017 Mar 21]; 51:33. Doi: https://doi.org/10.1590/S1518-8787.2017051006815
5.Garcia LP, Freitas LRS, Silva GDM, Hofelmman DA. Violence against women: feminicides in Brazil. Institute of Applied Economic Research [website]. [cited 2017 Oct 25] Available from: http://www.ipea.gov.br/portal/images/stories/PDFs/130925_sum_estudo_feminicidio_leilagarcia.pdf
6.Marques TM, Coleta MFD. Attribution of causality and reactions of women who have experienced episodes of marital violence. Temas psicol. [Online]. 2010; 18(1):205-18. Available from: http://pepsic.bvsalud.org/scielo.php?script=sci_arttext&pid=S1413-389X2010000100017
7.Diniz GRS, Pondaag MCM. The hidden face of violence against women: silence as a strategy for survival. In: Almeida AMO. Violence, social exclusion and human development: studies on social representations. Brasília (DF): Universidade de Brasília Publisher; 2006. p. 233-59.
8.Peniche ACG, Chaves EC. Some considerations about surgical patients and anxiety. Rev. latinoam. Enferm [Online]. 2000; 8(1):45-50. Doi: http://dx.doi.org/10.1590/S0104-11692000000100007
9.Perseu Abramo Foundation [web site]. The Brazilian woman in the public and private spaces [cited 2017 May 02]. Available from: http://csbh.fpabramo.org.br/o-que-fazemos/editora/livros/mulher-brasileira-nos-espacos-publico-e-privado
10.Parker G, Lee C. Relationship among abuse characteristics, coping strategies, and abused women's psychological health: a path model. J. interpers. Violence [Online]. 2007; 22(9):1184-98. Doi: 10.1177/0886260507303732.
11.Leite FMC, Moura MAV, Penna LHG. Women's perceptions of violence against women: an integrative review of the literature. Av. enferm [Online]. 2013; 31(2):136-46. Available from: http://www.scielo.org.co/pdf/aven/v31n2/v31n2a14.pdf
12.Parente EO, Nascimento RO, Vieira LJES. Coping with domestic violence by a group of women after the police report. Rev. Estud. Fem [Online]. 2009; 17(2):445-65. Doi: http://dx.doi.org/10.1590/S0104-026X2009000200008
13.Ministry of Health (Br). Department of Health Policy. Intrafamily violence: guidelines for practice in service [internet]. Brasília (DF): MS Publisher; 2001. [cited 2017 Oct 21]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/cd05_19.pdf
14.Silva LL, Coelho EBS, Caponi SNC. Silent violence: psychological violence as a condition of domestic physical violence. Interface comun. saúde educ [Online]. 2007; 11(21):93-103. Doi: http://dx.doi.org/10.1590/S1414-32832007000100009
15.Santos ACW, Moré CLOO. Repercussion of violence in women and their forms of coping. Paideia[Online] 2011 [cited 2017 Oct 28]; 21(49):227-35. Doi: http://dx.doi.org/10.1590/S0103-863X2011000200010
16.Moré CLOO. Significant social networks as an instrument of psychological intervention in the community context. Paidéia [Online]. 2005; 15(31):267-97. Doi: http://dx.doi.org/10.1590/S0103-863X2005000200016
17.Nakano AMS. The experiences of breastfeeding for a group of women: from the limits of being the body to the child and of being the body of oneself. Cad. Saúde Pública [Online]. 2003; 19(2):355-63.
18.Fontanella BJB, Ricas J, Turato ER. Sampling by saturation in qualitative research in health: theoretical contributions. Cad. Saúde Pública [Online]. 2008; 24(1):17-27. Doi: http://dx.doi.org/10.1590/S0102-311X2008000100003
19.Caregnato RCA, Mutti R. Qualitative research: discourse analysis versus content analysis. Texto & contexto enferm [Online]. 2006; 15(4):679-84. Doi: http://dx.doi.org/10.1590/S0104-07072006000400017
20.Minayo MCS. Violence: an old-new challenge for health care. Rev. bras. edu. Méd [Online]. 2005; 29(1):55-63. Available from: http://www.educacaomedica.org.br/UserFiles/File/2005/violencia.pdf
21. Bozzo ACB, Matos GC, Beraldi LP, Souza MD. Domestic violence against women: characterization of reported cases in a municipality in the countryside of São Paulo. Rev. enferm. UERJ [Online]. 2017; 25:e11173. Doi: http://dx.doi.org/10.12957/reuerj.2017.11173
22.Guerra C. Uncovering power and violence in gender relations: Uberlândia-MG 1980/1985. [MSc dissertation] São Paulo: University of São Paulo; 1998.
23.Lambrocini LM, Ferraz MIR, Trigueiro TH, Fegadoli D. Profile of violence against women attended at the inn of Maria. Rev. Esc. Enferm. USP [Online]. 2010; 44(1):126-33. Doi: http://dx.doi.org/10.1590/S0080-62342010000100018
24.Fortuna SLA. Strategies for coping with domestic violence: a study on Guarapuava. ex æquo [Online]. 2011 [cited 2017 Jan 10]; 24:139-51. Available from: http://www.scielo.mec.pt/pdf/aeq/n24/n24a11.pdf
25. Adeodato VG, Carvalhoa RR, Siqueira VR, Souza FG. Quality of life and depression in women victims of their partners. Rev. saúde pública [Online]. 2005; 39(1):108-13. Doi: http://dx.doi.org/10.1590/S0034-89102005000100014
26.Vilhena CV. Results of a survey: an analysis of domestic violence among evangelical women. In: Making gender proceedings 9: diasporas, diversities, displacements; 2010 Aug 23-26; Florianópolis, Brazil. Florianópolis (SC): University of Santa Catarina; 2010. p.1-9. [cited 2017 Oct 10]. Available from: http://www.fazendogenero.ufsc.br/9/resources/anais/1280156603_ARQUIVO_ValeriaCristinaVilhena.pdf
27. Lazarus RS, Folkman S. Cognitive appraisal processes. In: Lazarus RS, Folkman S. Stress appraisal and coping. New York (USA): Spring; 1984. p. 22-54.
28.Fernandes G, Inocente NJ. Strategies for coping: a bibliographic survey. In: Proceedings of the XIV Latin American Meeting of Scientific Initiation and X Latin American Meeting of Graduate of the University of Vale do Paraíba; 2013 [cited 2017 Dec 20]. Available from: http://www.inicepg.univap.br/cd/INIC_2010/anais/arquivos/0570_0609_01.pdf
29.Fayram ES, Christensen PJ. Planning: strategies and nursing orders. In: Christensen PJ, Kenney JW. Nursing process: application of conceptual models. St. Louis (MO): Mosby; 1995. p. 164-85.
30.Zaleski M, Pinski I, Laranjeira R, Ramisetty-Mikler S, Caetano R. Violence between intimate partners and alcohol consumption. Rev. saúde pública [Online]. 2010; 44 (1): 53-9. Doi: http://dx.doi.org/10.1590/S0034-89102010000100006
31.Vieira LB, Padoin SMM, Souza IEO, Paula CC. Perspectives for nursing care for women who report violence. Esc. Anna Nery Rev. Enferm [Online]. 2011; 15(4):678-85. Doi: http://dx.doi.org/10.1590/S1414-81452011000400004
32.Neri AL. Keywords in gerontology. Campinas (SP): Alínea Publisher; 2005.
33.Seidl EM. Coping and clinical and socio-demographic aspects of people living with HIV/AIDS. Psicol. reflex. Crit [Online] 2005 [cited in Oct 02, 2016]; 18(2):421-9. Doi: http://dx.doi.org/10.1590/S1413-73722005000300010
34.Faria MGA, David HMSL, Rocha PR. Insertion and religious practice among women: Protective aspects to the use of alcohol and violence. SMAD, Rev. eletrônica saúde mental alcool drog [Online]. 2011; 7(1):32-7. Doi: http://dx.doi.org/10.11606/issn.1806-6976.v7i1p32-37
35.Vinagre M. Crioula notebooks: impact of violence on the lives of black women in the communities of Afro-Brazilian religions. Rio de Janeiro: UNIFEM; 2008.
36.Antoniazzi AS, Dell'aglio DD, Bandeira DR. The concept of coping: a theoretical review. Estud. psicol [Online]. 1998 [cited 2017 Oct 21]; 3(2): 273-94. Doi: http://dx.doi.org/10.1590/S1413-294X1998000200006
37.Fonseca PM, Lucas TNS. Domestic violence against women and its psychological consequences. Bahia Foundation for the Development of Sciences [end-of-course written work]. Salvador (BA): Bahia School of Medicine and Public Health; 2006.
38.Gomes NP, Bonfim ANA, Barros RD, Silva Filho CC, Diniz MF. Confronting conjugal violence in the context of family health. Rev. enferm. UERJ. 2014; 22(4):477-81.