FIGURE 1: Network support to disabled people. Brasil, 2014.
ORIGINAL RESEARCH
Support network for persons with physical disabilities
Paula BrignolI; Soraia Dornelles SchoellerII; Denise Maria Guerreiro Vieira da SilvaIII; Julia Estela Willrich BoellIV; Soraia Geraldo Rozza LopesV; Sabrina da Silva de SouzaVI
I
Nurse. Master in Nursing. Neonatal Intensive Care Unit of Carmela Dutra
Maternity Hospital. Florianópolis, Santa Catarina, Brazil. E-mail: paulabrignol@gmail.com
II
Nurse. PhD in Nursing. Professor, Federal University of Santa Catarina.
Florianópolis, Santa Catarina, Brazil. E-mail: soraia.dornelles@ufsc.br
III
Nurse. PhD in Nursing. Professor, Federal University of Santa Catarina.
Florianópolis, Santa Catarina, Brazil. E-mail:
denise_guerreiro@hotmail.com
IV
Nurse. Master in Nursing. PhD student, Federal University of Santa
Catarina. Florianópolis, Santa Catarina, Brazil. E-mail: juliaestela_8@hotmail.com
V
Nurse. PhD in Nursing. PhD student, Federal University of Santa Catarina.
Florianópolis, Santa Catarina, Brazil. E-mail: soraia.gr.lopes@gmail.com
VI
Nurse. PhD in Nursing. University Hospital Professor Polydoro Ernani São
Thiago. Florianópolis, Santa Catarina, Brazil. E-mail:
enfermeirasabrina@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.18758
ABSTRACT
Objective: to identify the social support networks of people with physical disabilities living in a city in southern Brazil. Method: in this exploratory, qualitative, descriptive study, data was collected from May to September 2014 by semi-structured interviews of 10 disabled persons, and their statements were then subjected to directed content analysis based on the network functions described by Sluzki. The study was approved by the Research Ethics Committee (No. 216.396). Results: the social support networks comprised family members and health professionals at differing levels of proximity. The types of support offered were: company/social support, emotional support, cognitive guidance, material and service assistance, and access to new contacts. Conclusion: it was possible to identify the social support networks of people with physical disabilities, and they were found to attenuate the limitations imposed by the disability.
Keywords: Social support; rehabilitation, disabled persons; health professionals.
INTRODUCTION
Disability is a broad term that includes physical disabilities, activity limitations, and restriction of social participation1,2. The National Policy for the Health of Persons with Disabilities proposed the concept of physical/motor deficiency as the complete or partial alteration of one or more segments of the human body, with impairment of physical function in the form of paraplegia, paraparesis, monoplegia, monoparesia, tetraplegia, tetraparesia, triplegia, triparesis, hemiplegia, hemiparesis, ostomy, amputation or absence of limb, cerebral palsy, dwarfism, and limbs with congenital or acquired deformity3.
According to the World Health Organization (WHO), there is a prevalence of over one billion people with some form of disability in the world. Deficiency needs to be addressed at different levels, such as those of clinical, rehabilitative, social and political nature, so that the inclusion of people with disabilities becomes more effective in society1.
Data from the 2010 demographic census described the prevalence of different types of disability - visual, auditory, motor/physical, mental/intellectual - in Brazil. There are approximately 46 million people with at least one type of disability in the country. Physical disabilities rank second among the most frequent deficiencies, with a prevalence of 7% in the Brazilian population. Regarding the age group, the physical disability again appears in second place with 5.7% in the population between 15 and 64 years2.
The impact caused in the life of persons with physical disability is of an extensive proportion. Health professionals have recently seen the need to study the relationship between daily life, physical disability and health care, which in turn, has fostered discussions in several circles. This help the clients and the professionals involved in their care understand the complexity of the impact of the physical disability causes on these individuals4,5.
The daily life of people with disabilities no longer represents only a life without diseases or complications arising from the chronic condition, but has come to be seen as the search for personal satisfaction, social inclusion and coping with their new condition backed by a well-structured and active support network4.
The support network consists of the structure from which social support comes; it is the set of bonds and their roles related to the individuals, either by ties of kinship, friendship or acquaintance, or by a framework of relations of a particular individual or a framework of connections between a group of people6.
By being part of a support network, persons bring with them their own characteristics and particular views of the world, including interests, abilities, desires and frustrations. There are also other forces arising from the interaction between individuals, such as: atmosphere, communication, participation, goals, objectives, homogeneity, group size, norms and controls6.
The functions of the network, according to Sluzki, are described in categories and organized in: social companionship/social support - the practice of joint activities or just staying together; emotional support - positive emotional exchanges, understanding the individual, sympathy, empathy, encouragement and support; cognitive guide and advice - relationships with the aim of exchanging personal or social knowledge, as well as clarifying perspectives and providing models of behavior; material and service aid: specific aid based on specialist information or physical assistance, including health services; and, access to new contacts - connection with people and networks that were not part of the social network of people with disabilities6.
The relevance of knowing the support networks for people with physical disabilities is based on the understanding that health professionals need to promote their role as an integral part of the network, and with this, mobilize the other members of the network, enhancing their contribution to the health care of these people. Thus, this study aimed to know the support network of people with physical disabilities residing in a municipality in the south of Brazil.
LITERATURE REVIEW
The support network of people with disabilities influences the perception of care and the incapacity of people with disabilities7. The level of perception of people with physical disabilities about their support network is strengthened by family relationships and also by close people8-10.
A study carried out with people with intellectual disabilities investigated the structural and functional characteristics of the support network and showed that the network was composed of family members, co-workers, friends, neighbors and health professionals. The frequency of contact between the network and the person with disabilities was high, happening at daily basis. The functionality of the network was pointed out by affective support and the exchange of information provided6,11,12.
Besides the aforementioned members, the support network of deaf people is composed of institutions, neighbors and distant relatives, with different degrees of involvement within this network. The efforts of health professionals to implement strategies and actions aimed at strengthening social networks of support and social protection are important, highlighting the need to expand access to information for the autonomy of individuals and families in their daily life10,13.
Some demographic variables may be related to the support network. In the case of gender, the search for formation of the support network is relatively higher for women and also for individuals who have a caregiver. However, regarding age and the time living with the deficiency, these issues are not related to the support network nor to the support provided13.
Depressive symptoms are one of the consequences of the deficiency and these tend to increase the limitations imposed by the condition. The presence of the support network decreases the emergence of these symptoms and also the risk of presenting them13.
From the foregoing, it must be considered that the support network of people with disabilities contributes significantly to their daily life, significantly contributing to reduce functional losses, preserving the emotional system, and helping to cope with the condition, that is, primary functions for re-establishing the quality of life and of living with the limitations imposed by the disability. Thus, knowing the support network of people with disabilities becomes necessary to propose new health care strategies for this population, for the planning of actions and social inclusion.
METHODOLOGY
This is a descriptive study with qualitative approach carried out in a municipality in the South of Brazil, from May to September 2014.
The study participants were 10 people with physical disabilities residing in a municipality in the South of Brazil. They were intentionally selected from a list provided by a nongovernmental entity that assists this population. The number of participants was defined by the researchers based on the consistency of the data obtained with these participants. The inclusion criteria used were: to be a person with physical disability for more than one year; to be older than 18 years; having the ability to communicate verbally. As exclusion criteria were determined: to have some cognitive, auditory and/or multiple deficiencies associated.
Data collection took place through a semi-structured interview on the day and time pre-scheduled with the participants, who were contacted by telephone based on the list provided. The interviews were conducted in the home environment and, with the participants' consent, recorded in digital format and later transcribed. The transcripts were carried out by the researcher and an assistant who received specific training.
The data analysis was guided by the proposal of directed analysis, which consists in observing already established models of data categorization14. The categories of Sluzki were used as reference for this analysis: social companionship/emotional support, social support, cognitive guide and advice, social regulation, material help and services and access to new contacts. The pre-analysis and the material exploration were carried out. The categories social companionship and social support were joined by their proximity of meanings among the research participants. The report gave rise to the following categories of support network: companionship/social support, emotional support, cognitive guidance and advice; material help and services; and access to new contacts.
Ethical issues followed the norms and guidelines regulating research involving human beings, defined by Resolution 466/2012 of the National Health Council, Ministry of Health. The project was approved by the Ethics Committee under opinion nº. 216.396 of the Federal University of Santa Catarina. In order to ensure the participants' anonymity, their identities were replaced by the letter P followed by sequential numbers from 1 to 10. The participants were instructed about the objectives and the method of the research. They accepted to participate by signing the Informed Consent Term (ICF).
This study is part of the larger project entitled The condition of physically disabled people in Florianópolis: epidemiological profile, quality of life, support networks and work process , financed by the Program of Support to Nuclei of Excellence (PRONEX) linked to the Foundation for Research Support and Innovation in the State of Santa Catarina (FAPESC), and it is part of the Master dissertation entitled Support Network for physically disabled people, presented to the Graduate Program in Nursing, Federal University of Santa Catarina.
RESULTS AND DISCUSSION
Among the participants of this research, three presented paraplegia caused by roadway injury or chronic disease; three had tetraplegia caused by iatrogenic or shallow water diving; and four had amputation, three in lower limbs and one in upper limbs, caused by cancer or roadway injury. Of these, five participants were married, five were single. Among the occupations, seven were retired, one was a secretary, one was a clerk in a print company, and a disabled athlete. In terms of education, one had completed higher education, three had incomplete higher education, three had complete high school, two had incomplete high school and one had incomplete elementary education.
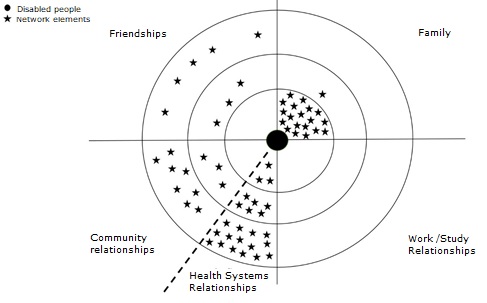
The support network of people with physical disabilities was recorded in a network map, based on the Sluzki model, and divided into quadrants, where we find family, friendships, study/work relations and community relations, which are subdivided into relations with health systems6. The model is formed by concentric circles; the circle placed closest to the center represents intimate relationships. This is followed by the circle that represents the intermediate relations, the relations with the lowest degree of commitment, and the outer circle represents occasional relations. The support network for the study participants is formed by family members, friends and also relations with the community and with health systems. The components of the support network of the interviewees are shown in Figure 1.
FIGURE 1: Network support to disabled people. Brasil, 2014.
The study participants received support mostly from family members and health professionals, with varying degrees of proximity and different types of support. The main source of support of people in chronic condition are the relatives, but the support received from friends, neighbors and co-workers was also emphasized as indispensable to overcome the difficulties. In order to family members and health professionals be able to contribute to the integration of the chronic disabled patient, it is necessary to know the other participants in the support network, to share experiences in an effective way and form a bundle of relationships that benefit the disabled person.15
Social companionship/support
In this category, the participants defined support as the constant presence of the network, the daily supply of basic necessities and the possibility of returning to daily activities. They pointed to the network as family members, friends, people from the place of residence and health professionals, in different degrees of affinity.
My family, my mother was always on my side helping me, she was the one who did the dressing, she was everything, my mother, then I went so, healing, improving gradually, but my mother always helped me in everything. (P4)
My family, I have the full support from my family, my parents, my sister. (P1)
Then, my husband left his job to stay home with me so I would not stay home alone. (P5)
The network from this point of view, admittedly, has an important role to face the new condition, serving as a subsidy for the discovery of new activities, besides the inclusion of the disabled person in activities that allow physical and psychological independence.
It is important for everything. For your self-esteem, for yourself! (P2)
My husband [...]. I think it's everything to me. It´s me and him, one leaning on the other. (P3)
Fundamental to my rehabilitation, and especially my psychological rehabilitation. (P10)
The findings corroborate with specialized literature on the importance of networking in the interaction and access to new experiences. The practice of sports, the engagement in associations, environmental accessibility and even the feedback of health services, when necessary, make it possible to advance physical and psychological emancipation16,17.
Health professionals, just like family members, are main actors involved in the support network for disabled persons, even with distinct roles in care. Both perform actions that benefit the adaptation and the experience of the person who experiences physical disability. The emphasis given to health professionals is related to their dual role as a support network for people with disabilities and for their families10.
Emotional support
Support is referred to as emotional support and concern for physical, psychological and material well-being. This is linked to the possibility of changing or reversing the current situation, to a more adequate and comfortable one to the disabled person needs.
My father would stay at home taking care of the house, and when I got home, everything was clean, because I could not get an infection, at the time I was undergoing chemo. (P1)
My brothers would call me all the time. We meet to barbecue, we are always together. (P2)
Everything at home, really, everything! They help me take care of the children, the house, my house is now clean. I have decent food today. This is how it is today. (P8)
The influence of the support offered by the network of people with physical disabilities is described in the scientific environment as a support to face the challenges arising from the new condition, which may be physical, environmental, social and psychological barriers. This support is defined as an important and essential factor in the disabled person movement, so that they can overcome the challenges imposed by their condition18,19.
Emotional support is gained through the help of those around them, constructing positive attitudes that reinforce the esteem and confidence of the subjects, permeated by attitudes that seek feelings of comfort. The family is referred to as an important source of emotional support, offering security and psychological support6,11.
Cognitive guide and advice
Support is seen as a way to get new contacts, to exchange information and experiences to obtain new ways of facing the problems of the present condition. It helps people with disabilities take a more active stance with their family network, leading them to discover new ways of coping.
I did not do occupational therapy, but we used to talk a lot of things with who had already done it and I would try it at home and it use to work. (P7)
When I understood the sequelae of the injury and especially the possibilities of starting to do again practically all the activities I used to do before the injury. (P10)
The exchange of information between people with disabilities and the members of their support network prompt a different perspective of the condition, providing a way to face the different paths in the course of their disability. Currently, the studies discuss the use of technological resources, such as virtual social networks, research pages that add new forms of both formal and informal exchange of knowledge with the purpose of acquiring subsidies to face the condition20,21.
Material help and services
Support is referred to as the exchange of information with specialists, or specific help from health professionals, leading them to engage in their treatment, discussing doubts and questioning professionals, and assuming responsibility for their own condition.
Some things they would give me at the Rehabilitation Center, but a few things like, sometimes gloves that I need to do procedures like that, they would give me. (P6)
I was hospitalized in the Hospital; I have been treated until now, the orthopedist does the follow up, I did an x-ray of the spine, to see how the surgery was. I do treatment with the urologist, ophthalmologist too. (P6)
Because I think that the Government gives everything to us, gives all the support, but, there are a lot of people that keep waiting at home, and that doesn't work, they go after it. (P9)
The demand for health services, both those specialized in disabilities and basic health care, allows the commitment to treatment and the search for constitutionally acquired rights. Health services must provide for the needs of people with disabilities so that they may remain healthy, able to re-enter society by reducing environmental, physical and psychological barriers22-24.
Access to new contacts
Access to new contacts represents the connections with people or networks that until then were not part of the individuals' social network. Support is referred to as a network of contacts that leads to needs acquired after the disability, such as: new therapies, treatment facilities, information about their current condition and even rights guaranteed by law through associations or non-governmental organizations.
Health institutions (hospitals and rehabilitation centers) could provide access to information more quickly and effectively to the newly injured person. I, for example, went because of an invitation from a friend to this sport institution for disabled people. (P10)
They sent me from the Public Hospital to the rehabilitation, and from there they indicated me to a University Physiotherapy Center . And then I met a man who makes prosthesis there at Kobrasol, then he pointed me to make the card. (P2)
The presence in different activities makes it possible to increase the support network for people with disabilities. This, in turn, results in new contacts that lead them to exchange information and subsidize the search for different treatments and new ways to accelerate the rehabilitation process. The search for health care rights and treatments contributes to the increase of independence and the coping with the new condition25,26.
Ordinance nº 793 of the Ministry of Health27 guarantees health care for people with disabilities in the care network. Among the guidelines that stand out are: guarantee of access to quality of services; availability of comprehensive care and multiprofessional assistance; expansion of access and service qualification to this population, besides assurance to health care in specialized rehabilitation centers.
CONCLUSION
The support network provides support to people with physical disabilities, minimizing the limitations, contributing to the confrontation, enabling the search for new treatments, providing physical, psychological and financial independence, which positively impacts the emotional aspects, the new acceptance of the new physical condition and in the relationship with the world and the people that surround them. Family, friends and health professionals are part of the support network.
The family was considered the main source of support by the participants. The family as a support network is a differential that reflects positively on the daily lives of people with disabilities. Also, health professionals were mentioned as strong components in the support network for people with disabilities. They contribute with scientific knowledge and interventions necessary to adapt to daily life and face the challenges of living with a physical disability.
In this sense, the support network establishes strategies that assist disabled persons to deal with the situations imposed by the acquired condition, including access to the health services necessary to reestablish their well-being. However, it should be noted that many of the original family and social ties become fragile, thus evidencing the need to create a support network to cope with this condition. Furthermore, there is not always an effective interaction between the members of the support network. This could be promoted by professionals in order to optimize the support and attendance of the needs of people with disabilities.
The reduced number of participants represents a limitation of the study. It prevents the generalization of the findings. It is worth emphasizing that care for physical disabled individuals in their multiple dimensions is a vast field of knowledge to be explored. Thus, further studies dealing with this part of the population are important.
REFERENCES
1. World Health Organization. World report on disability. The World Bank. Lexicus Translation Services. São Paulo: SEDPcD; 2012.
2.Oliveira LMB. Census Primer 2010-People with Disabilities. Brasília (DF): Human Rights Secretariat of the Presidency of the Republic (SDH/PR); 2012 [cited on 21 Nov 2016]. Available at: http://www.pessoacomdeficiencia.gov.br/app/publicacoes/cartilha-do-censo-2010-pessoas-com-deficiencia
3. Ministry of Health (Br). Secretariat of Health Care. National Policy on the Health of Persons with Disabilities. Brasília (DF): Ministry of Health, 2008 [agitated on October 16, 2016]. Available In: http://bvsms.saude.gov.br/bvs/publicacoes/politica_nacional_saude_pessoa_deficiencia.pdf
4.Schoeller S, Bitencourt R, Leopardi M, Pires D, Zanini M. Changes in the lives of people with acquired spinal cord injury. Rev Eletr de Enf. [online]. 2012 [cited on 21 Nov 2016]; 14 (1): 95-103. Available at: http://www.fen.ufg.br/revista/v14/n1/v14n1a11.htm.
5.Interdonato GC, Greguol M. Quality of life and habitual practice of physical activity in adolescents with disabilities. Growth. 2011; 2 (21): 282-95.
6.Sluzki CE. The social network in systemic practice: therapeutic alternatives. 3rd ed. Translated by Claudia Berliner. São Paulo: House of the Psychologist; 2006.
7.Zheng QL, Tian Q, Hao C, Gu J, Lucas-Carrasco R, Tao JT, et al. The role of quality of care and attitude toward disability in the relationship between severity of disability and quality of life: findings from a cross-sectional survey among people with physical disability in China. Health qual life outcomes. 2014; 12 (25): 1-10.
8.Kara B, Aikikel CH. Predictors of coping in a group of Turkish patients with physical disability. J clin nurs. 2011; 21 (7-8): 983-93.
9.Van Asselt-Goverts AE, Embregts PJCM, Hendriks AHC, Wegman KM, Teunisse JP. Do social networks differ? Comparison of the social networks of people with intellectual disabilities, people with autism spectrum disorders and other people living in the community. J Autism Dev Disord. 2015; 45 (5): 1191-203.
10.Alves TJL, Pires PNA MNA, Servo MLS. A look at the role of nurses in the care of people with disabilities: integrative review. Rev enferm UFPE [online]. 2013 [cited on 13 Nov 2016]; 7 (br): 4892-8.
11.Souza SS, Silva DMGV. Going through the experience of treatment for tuberculosis. Texto contexto - enferm. [online] 2010 [cited on 21 Oct 2016]; 19 (4): 636-43. Available at: http://www.scielo.br/pdf/tce/v19n4/05.pdf.
12.Bittencourt ZZLC, Françozo MFC, Monteiro CR, Francisco DD. Ciênc. Saúde coletiva [online]. 2011 [cited on Oct 20, 2016]; 16(suppl 1): 769-76. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232011000700007&lng=en.
13.Fauth EB, Gerstorf D, Ram N, Malmberg B. Changes in depressive symptoms in the context of disabling processes: role of demographic dharacteristics, cognitive function, health, and social support. J gerontol b psycho soc sci. 2012; 67 (2): 167-77.
14. Hsieh HF, Shannon SE. Three approaches to qualitative content analysis. Qual Health Res. 2005; 15 (9): 1277-88.
15.Di Primio AO, Schwartz E, Bielemann VLM, Burille A, Zillmer JGV, Feijó AM. Social network and supportive links of families of children with cancer. Texto contexto - enferm. [online]. 2010 [cited on 21 Nov 2016]; 19 (2): 334-42. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-07072010000200015&lng=en.
16.Rattray N. Wheelchair basketball teams the second families in highland Ecuador. Review of Disability Studies: An International Journal. 2014; 9 (2 & 3): 92-103.
17.Borges AMF, Brignol P, Schoeller SD, Bonetti A. Perception of people with spinal cord injury over their condition. Rev Gaúcha Enferm. [online]. 2012 [cited on 02 Nov 2016]; 33 (3): 119-25. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1983-14472012000300016&lng=en.
18.Amendola F, Oliveira MAC, Alvarenga MRM. Influence of social support on the quality of life of the family caregiver of people with addiction. Rev Esc Enferm USP. [online]. 2011 [cited on 18 Oct.2016]; 45 (4): 884-9. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0080-62342011000400013&lng=en .
19.Gonçalves TR, Pawlowski J, Bandeira DR, Piccinini CA. Evaluation of social support in Brazilian studies: conceptual aspects and instruments. Ciênc saúde coletiva. [online]. 2011 [cited on Oct 18, 2016]; 16 (3): 1755-69. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232011000300012&lng=en.
20.Ko HC, Wang LL, XU YT. Understanding the different types of social support offered by audience to diary-like a-list and informative bloggers.
Cyberpsychology behav soc netw. [online] 2013 [cited in 17 Oct 2016]; 16 (3): 194-9. Available at: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3603495/.
21.Raghavendra P, Wood D, Newman LA, Lawry J. Why are not you on facebook? Patterns and experiences of using the internet among young people with physical disabilities. Technol disabil. 2012; 24 (2): 149-62.
22.Dezoti AP, Alexandre AMC, Tallmann VAB, Maftum MA, Mazza VA. Social network to support child development according to the family health team. School Anna Nery. [online]. 2013 [cited on 20 Oct 2016]; 17 (4): 721-9. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1414-81452013000400721&lng=en.
23. Alvarenga MRM, Oliveira MAC, Domingues MAR, Amendola F, Faccenda O. Social support network of the elderly attended by Family Health teams. Ciênc. Saúde coletiva. [online]. 2011 [cited on Oct 23, 2016]; 16 (5): 2603-11. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232011000500030&lng=en.
24.Girondi JBR, Santos SMA, Nothaft SCS. Perspectives of physical disability in the elderly: vulnerabilities in health. Rev Enferm UERJ. 2015; 23 (2): 172-7.
25. Mesquita RB, Morano MTAP, Landim FLP, PC Collares, Pinto JMS. Network of social support and health of elderly chronic lung disease. Ciên saúde coletiva. [online]. 2012 [cited on Oct 21 2016]; 17 (5): 1125-33. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232012000500006&lng=en.
26.Holanda CMA, Andrade FLJP, Bezerra MA, Nascimento JPS, Neves RF, Alves SB et al. Support networks and people with physical disabilities: social insertion and access to health services. Ciênc. Saúde coletiva. [online]. 2015 [cited on 03 Nov 2016]; 20 (1): 175-84. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232015000100175&lng=en.
27. Ministry of Health (Br). Ordinance No. 793, of April 24, 2012. Establishes the Network of Care for Persons with Disabilities under the Unified Health System. Brasília (DF): Cabinet Ministerial, 2012 [cited on October 12, 2016]. Available at: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2012/prt0793_24_04_2012.htm.