FIGURE 1: Professional data of the surveyed nurses. Rio de Janeiro, 2016.
ORIGINAL RESEARCH
Teaching and learning in the gynecological brachytherapy nursing appointment: the nurses' perspectives
Cláudia Regina Gomes de AraujoI; Ann Mary Machado Tinoco Feitosa RosasII; Harlon França de MenezesIII; Benedita Maria Rêgo Deusdará RodriguesIV
I
Nurse. PhD in Nursing. University Hospital Clementino Fraga Filho. Rio de
Janeiro, Brazil. E-mail: clauregingomes@hotmail.com
II
Nurse. PhD. Associate Professor. Anna Nery Nursing School, Federal
University of Rio de Janeiro. Rio de Janeiro, Brazil. E-mail: annmaryrosas@gmail.com
III
Nurse. Master student in Nursing. Anna Nery Nursing School, Federal
University of Rio de Janeiro. Rio de Janeiro, Brazil. E-mail: harlonmenezes@hotmail.com
IV
Nurse. PhD in Nursing. Full Professor. Rio de Janeiro State University. Rio
de Janeiro, Brazil. E-mail:
benedeusdara@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2016.18737
ABSTRACT
Objectives: to identify nurses' expectations in teaching and learning in the gynecological brachytherapy nursing appointment and to discuss the links between the intentionalities expressed by these professionals. Method: this descriptive study, based on Sociological Phenomenology, was conducted from January to May 2012. The participants were six nurses working in two radiotherapy referral services. Data were obtained by phenomenological interview. Results: analysis of the declarations yielded two concrete categories of lived experience: Contemplating the uniqueness of each subject in treatment; and Giving due value to the technical care. Conclusion: the lived experience of nurses is that of professionals with the sensitivity to adapt individual care to the technology, where teaching and learning in the nursing appointment provides nurses with input to understanding each client with their own degree of understanding, which is what demands personalized care, so that there is quality of life in the treatment.
Keywords: Nurse's role; nursing care; radiotherapy; brachytherapy
INTRODUCTION
Gynecological brachytherapy is a method in which ionizing radiation is applied directly into the tumor through intra-cavitary applicators and has been used in cervical neoplasias since the 1960s. However, this technique was only introduced in Brazil in the 1990s. This is an invasive and painful procedure that requires anesthesia and is used to complement uterus or vagina cancer-fighting treatments1,2.
The experience of providing care in the radiotherapy service at a university hospital showed that the implementation of the nursing consultation (NC) to customers who are subjected to such treatment has benefited them. When they have the nursing consultation before gynecologic brachytherapy, the situation of coping with the therapy becomes milder.
Scholars argument that the NC represents a soft-hard technology that favors self-care because it allows customers to develop their own skills to improve their quality of life. Through the NC, nurses exercise complete autonomy to develop comprehensive health care promotion strategies to customers, families or communities, fulfilling their main function as health educators3.
The educational process that takes place during the CE helps customers to optimize self-care as well nurses in planning care. With the consultations, nurses can identify the individual needs of customers, learning how each one acts and reacts before the treatment, customizing the assistance. Given the above, it is necessary to understand the guiding question: how do nurses experience teaching and learning in nursing consultations during application of gynecological brachytherapy?
Scholars indicate that the medical literature does not report exactly what undergoing this type of treatment means for the client and does not specify the necessary attention of the healthcare team to provide detailed guidance on the procedure4. Thus, while it is understood that the technical information reported in the literature is important, concern with emotional aspects of customers is also fundamental.
In a bibliometric review, there was a predominance of studies concerned with nursing care to clients submitted to radiotherapy, whether to prevent, identify and treat complications and side effects, or to report the experiences of customers and their families in face of the diagnosis and treatment of cancer5.
These themes cause unease among nurses. Thus, these professionals should be sensitive when providing comprehensive health care to cancer patients beyond their questions on the professional practice. This would lead to the production of new knowledge, contributing to organizational changes and the spread of new technologies5,6.
Thus, studies of this nature are justified by the fact that research on the exchange of experiences and knowledge in nursing consultations during gynecological brachytherapy is scarce, as well as by the importance of listening to nurses about their educational needs, in order to direct nursing actions towards the reasons that lead customers to seek nursing consultations.
In this context, the objective of this study was to identify the expectations of nurses in teaching and learning in nursing consultations for gynecological brachytherapy and discuss the connections between the intentionalities expressed by these professionals.
Theoretical-methodological reference
This is a qualitative, descriptive and phenomenological research based on the theoretical-philosophical and methodological framework of Alfred Schütz 7. The choice of this approach is due to the recognition of the importance of knowledge on each client, understanding that every nursing consultation constitutes a teaching-learning opportunity, fruit of the interpersonal relationships of this meeting.
Austrian Alfred Schütz (1899-1959) sought support in social science methodology and phenomenology to achieve his purpose of establishing the foundations of a comprehensive phenomenological sociology, thus developing his theory, which proposes the analysis of mutual social relations involving people8.
Schütz discusses the structure of reality and emphasizes the social relationship as a fundamental element to interpret the meanings of individuals' actions in the everyday world. For this, he chooses the understanding that comes from the everyday life of human existence, considered the social world, as essential. This study highlights the characteristics of each relationship, whose actions occur consciously, as they are intentional, discussing the relationship between consciousness and action, which has a meaning for the individual9.
Thus, men act according to goal-directed motivations pointing to the future called "reasons for", and the reasons for their actions rooted in past experiences, in the personality developed throughout the life called "reasons why"8.
We understand that in this reference, reality is constructed by men from their inter-subjective experiences. The author, with his ideas, founds a sociology of knowledge that starts from the common sense of everyday life and the cognitive processes through which is established and applied, treating inter-subjectivity as intra-mundane data on which stands any activity of personal relation and of social science itself.
The study was conducted in two reference scenarios in radiotherapy: the first scenario was a clinic of the radiotherapy department of a general, public and university hospital located in Rio de Janeiro municipality, and the second scenario was a radiotherapy clinic of a philanthropic hospital specialized in oncology in the city of Barretos, São Paulo. Both services have their attention focused mainly on clients of the Unified Health System, receiving people from all states of Brazil.
The technique used was phenomenological face to face interview, where interviewer and interviewee face each other and are subject to verbal and non-verbal influences aiming at accessing the experience of human beings through any movement of understanding10.
Interviews took place from January to May, 2012, in rooms of those institutions. Nurses were asked about professional data and the guiding question was: what does it mean for you to teach and learn from customers during the NC in brachytherapy?
The participants were six nurses who work with clients undergoing gynecologic brachytherapy through nursing consultation, no matter the time they have exercised the profession and this activity.
Interviews were recorded in full-length, with the aid of a digital recorder and then were transcribed by the authors. Anonymity of participants was guaranteed by replacing the names of respondents by color names that are unique, as each individual.
This study was conducted according to the Resolution nº 466/2012 of the Ministry of Health (MOH), and approved by the Ethics Committee in Research involving human beings of the institutions where the research was conducted under the Opinions nº 127/2011/Rio de Janeiro and nº 551/2011/São Paulo. All nurses agreed to participate in the study and signed two copies of the Informed Consent.
For analysis of the interviews, the steps of Social Phenomenology11-14 were developed: listening to the recorded content of interviews; transcription; full-length text reading; grouping speeches according to affinity (common ideas); capture of the reasons for, through clippings of speeches that responded to the research question; rereading the text in full-length, in order to confirm that these ideas (specific categories of the experience) expressed the reasons for participation in nursing consultation; identification of relations of categories between themselves, reaching the typical action.
The specific categories of the experience that emerged from the testimonies of participants were: meeting the uniqueness of the patients in treatment and valuing the technical care.
RESULTS AND DISCUSSION
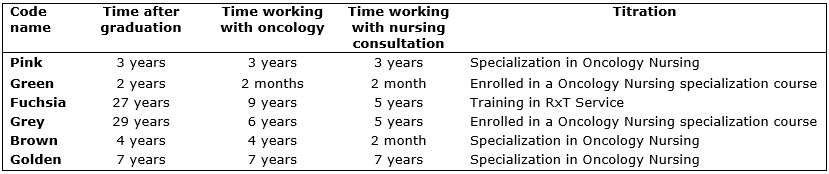
To illustrate the profile of participants, the Figure 1 was drawn up with their professional characteristics.
FIGURE 1: Professional data of the surveyed nurses. Rio de Janeiro, 2016.
The time elapsed since conclusion of the nurses' graduation course ranges from 2 to 29, and the time of experience with nursing consultation to customers in question ranges from 2 months to 7 years. There was recognition of the need for training by the interviewed nurses, and all of them had degrees specialized for care to oncological clients. The commitment with the profession, with care and with nursing consultation appeared in all speeches, regardless of the time elapsed since graduation.
Nurses reported they consider educational activities important, and that this should take place according to the needs of customers. For them, customers' self-care must be taught in a specific way, so that they may have quality of life during and after treatment.
The exploration and analysis of reports of the interviewed participants resulted in two categories which are interpreted below.
Meeting the uniqueness of the patients in treatment
The category emerged from the experience lived by nurses that said that customers should receive individualized care. After all, when the customer is guided according to their basic needs, she tends to understand the disease and to care satisfactorily of herself, passing through the treatment with the least possible adverse events.
Perceptions, interpretations and health actions are constructed in culture and in the individuality of every being. Self-knowledge, while facing a chronic and degenerative disease such as cancer, arises in the flow of the confrontations experienced, and leads one to reflect on the own life. However, this reflection is inserted in a meeting with oneself dangling in the various psychological stages of living with cancer. This process of exercising the thinking and feeling transforms the being, and self-knowledge emerges as an effect of this exercise, helping health by contributing to the balance of the being, a woman with cancer15.
Thus, when social action of care is directed towards the motivations of the other team members, this is harmonizing itself with the intentionalities4. Thus, the nursing staff must act in order to minimize these effects and serve as a link, working on achieving specific care and education of patients and families. Nursing consultation in the radiotherapy sector deserves special attention because this is the most specific activity performed by nurses in the sector. Patients seek the nursing consultation as a means of information for the practice of self-care and of facing the treatment. Thus, the NC makes nursing care personalized16.
Given the above, the complexity of the process of teaching and learning that takes place in nursing consultations to the client in question becomes evident. Furthermore, it is noteworthy that the way the customer presented herself at the moment of consultation influences the quality of what will be taught and learned. Hence the importance of respecting the individuality of each human being. The statements below illustrate how nurses showed interest in personal impressions of customers about experiencing cancer.
Teaching and learning that happens in nursing consultation is very important; we learn a lot from patients. Each one has their own perception of the treatment, their experiences are singular. This enriches us and helps us to plan the care for these patients. (Pink)
I learn from the personal account of each of them. Some may have had skin lesions, other difficulties passing urine; each one reacts differently. Consequently, it is during brachytherapy that I learn what they went through before that, and what they are going through at that moment and this will help me to direct care for this treatment. (Fuchsia)
Empathy was cited by the interviewed nurses as a key element in the relationship with clients. We cannot forget that cancer changes the life of those who fall ill, making people to learn to think according to their new life experience. Therefore, nurses should follow the reasoning of clients about their sensations arising from the reality, which is to have the disease. In the reports, the emergence of partnership among parties in the NC was registered. After all, change in the educational process is necessary, as the following reports show:
We learn a lot from the experience of patients, with all that concerns their routine. Mainly because there are cases where they (patients) only relate their experiences to the nurses, then the need of acknowledging the importance and the value of this exchange. (Green)
It has been rewarding to see customers feeling less anxious at the moment of undergoing treatment. It is good to see that the consultation was of great benefit for both, us as nurses and for clients. This interaction helps us to know if we are on the right track. (Grey)
Indeed, the uniqueness of the human being can only be understood when you have direct contact with them. Nursing professionals get to know the universe of clients with whom they get in contact when they show to be interested in their specific biography. The combination of these singularities will bring forth the typical (common) of the clientele, helping to build the model of care to be offered. This means that private interests may be in the same context of the interests of a group 7. Here is a reflection:
Teaching and learning are very important. In some situations, the doubt that a customer brings us may be the doubt of others. And with the knowledge that each customer brings us, we can go on learning to work in the various points of doubt and solve the problems, or try to mitigate them. That's why I think it's important that every form of care originates from the customers' needs. (Grey)
The partnership mentioned by the nurses in the conduct toward customers is derived from a trustful, typically face-to-face relationship, in which both subjects expose their views, in inter-subjectivity. Nurses, knowledgeable of the priorities of clients and their intentions regarding treatment, tend to bring the care to what was reported by them.
To do this, it is necessary to consider the strength of our neighbors, respecting their privacy, according to the report:
One cannot compare the patient A with the patient B, because the treatment may be the same, but the response will be different in each one of them. And by knowing the symptoms of a patient I can help another, who knows? What I have in mind is this: we have to respect the experience that each patient brings. (Brown)
Thus, it is clear that the intentional action of nurses must be developed including appreciation of the other, giving voice to the other. Hence the importance of taking into account the body of knowledge of those who are receiving care. The above reasoning also explained when professionals put themselves in the place of others. There is empathy and inter-subjectivity in their speech, even when declaring that they would not like that situation for themselves:
Wow, of course we have much involvement with patients, it is natural... I'm a woman and wouldn't like to be in their place... In the course of the applications, they start losing the fear and learn to have more confidence in us. Then it becomes easier to care for them. I feel like a person very much involved with them, even because I'm woman, just like them. (Fuchsia)
A practical example, experienced by the author, was punching the client's vein. She said it was for punching there (showed the place) because it was easier in the site she was indicating. This, in the practice of care, means giving voice to the other. Thus, the behavior of those who are cared for will be adjusted to their well-being and the nurse's behavior is modified according to the needs of each client.
Valuing the technical care
Of course due to the scientific knowledge acquired during their training, it was noticed in the nurses a concern about the technicism of the nursing care offered. Nevertheless, professionals showed interest in the personal impressions of customers undergoing treatment, as the following reports show:
It ends up becoming an exchange with the patients. We explain what we know about treatment, about how they should take care of themselves and they tell us how they are feeling with regard to treatment, they speak about physical reactions, too. (Green)
Thus, we guide on the procedure, explain how many people will be in the room, we say that there is an anesthesiologist, the resident in anesthesia, nursing staff, the radiation oncologist, the X-Ray technician; everything is explained... We know how difficult it is for patients [...] (Fuchsia)
Currently, according to the implementation of the Systematization of Nursing Assistance (SNA), it is essential that nurses show concern about the technological aspect of care, since advances in this endeavor move forward and evolve continuously. Thus, the registration of the nursing care rationale should happen in order to disseminate knowledge of the techniques and the consequent consolidation of the specific body of knowledge of the nursing staff.
Care to cancer clients is complex. This illness has special characteristics that require responsibilities from nurses that are private, as well as technical and scientific knowledge, and interpersonal relationship skills. Through the implementation of the SNA, nurses can use clinical reasoning and critical judgment to identify and survey problems and help in choosing the best care decisions according to the real needs of each client 17-19.
However, according to the lines, it appears that combining technical with humanized care is feasible. Thus, one can develop the social action and put himself in the other's place, at the same time. Just give voice to the neighbor, respecting his experience7. In the following speeches, it is clear that performing the technical care and displaying interest in the individuality of the client as is feasible. In this case, that care refers to the guidance on the exercise of vaginal dilation, a concern shown by the nurses:
We cannot forget that there is personal life after this treatment. That even if the patient thinks she will not have a sexual partner, she can find someone in the future. Sexual dysfunction is a serious thing. (Pink)
Some are more reserved, but others already use this as an excuse, the procedure, to leave issues about sexual life aside. We end up entering in women's issues, so many of them simply won't talk about it. Then, we remember the psychological aspect, and we forward these customers to psychology, if they wish so. It's very difficult for them. (Brown)
Thus, it is important to stress that the establishment of a nursing care protocol must occur in order to allow nurses to adapt their rationale to the needs and reality of each client, respecting their uniqueness. The following statement portrays this, in which it became clear that each client has something to teach, signaling that care and education must take place according to the customers' needs:
It is important that we adapt to patients. We have protocols, that of course we have to follow, but with exceptions. We end up, not circumventing these protocols, but adapting them to each patient. I see that, the more we act in this area, the more we learn from the customers. And the more we learn, the more lessons have to pass to them. (Brown)
Analyzing the above statements in the light of Phenomenology7, by combining the concern for the individuality of clients and the scientific aspect of care, nurses can tailor reasons for these customers for consultation with the reasons why of professionals for the care, generating reciprocal perspectives. Learn how to teach/learn is a challenge for nurses. This transforms knowledge into a relevant human conduct of their professional practice, translated as care.
The challenge is in teaching the practice of consultation and understanding that each nurse will manifest his/her own way of reflecting on this care. Therefore, it is observed that the impact of education and nursing practice consultation will be different for each nurse carrying out the consultation and for every customer assisted.
Thus, this is about understanding how the customers' relationship with the institution and its sectors takes place, since the treatment requires interdisciplinary knowledge of the multidisciplinary team. Therefore, this way, holistic care in nursing education will be implemented in fact, which should be grounded on the understanding and care of the humans beings in their entirety, satisfying their basic needs.
It is evident that teaching and learning are not simple tasks. For them to happen, it is necessary that the intentions of those who teach and those who learn be in line with each other. Respecting the potential of the other, with limitations or not, is necessary, recognizing that all learning pace is valid, provided the goal among the subjects be achieved. It is essential that everyone involved in that process may recognize that they have something to teach and to learn, without vanity. The process is ever-changing, because the experience of human beings changes, likewise their priorities (relevance).
CONCLUSION
In the study, we identified that nurses are understood as professionals with sensitivity to adapt individual care to technology. This allows a flexible interpretation of nursing actions recommended in the various protocols adopted in health institutions, through assistance, teaching, research and outreach in oncology.
Concern for the technical care combined with the individuality of the client should culminate in actions that occur in the nurses' daily life, while taking care of the customer submitted to gynecological brachytherapy. It is about developing a view that allows the evaluation of this kind of customers as a whole, seeking in their general situation elements that may be indicative of any failure of treatment at that time. Moreover, this aspect has in several occasions contributed to reduced duration of anesthesia, which has been observed in practice. Thus, queries allow the reduction of anxiety and assist the customers in understanding the treatment.
Professionals must know the social and clinical profile of clients and the meaning they attribute to their experiences, considering that each patient is unique and requires empathy and solidarity. From this perspective, there are great chances that the products of nurses' actions become the satisfaction of customers' needs on reciprocity of intentions.
New studies on the context of nursing consultations and their constructs related to the specificities of providing care in brachytherapy should be encouraged, expanding research scenarios, with participation of the subjects involved in the process of falling ill from cancer.
REFERENCES
1.Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Instituto Nacional de Câncer. Radioterapia e Braquiterapia de alta taxa de dose. Rio de Janeiro: INCA; 2009.
2.Silva RMV, Pinezi JCD, Macedo LEA, Souza DN. A atual situação da braquiterapia de alta taxa de dose em colo do útero realizada no Brasil. Radiol Bras. 2014; [cited 2015 Aug 29]; 47 (3): 159-64. Available from: http://www.scielo.br/pdf/rb/v47n3/0100-3984-rb-47-03-0159.pdf
3.Oliveira SKP, Queiroz APO, Matos DPM, Moura AF, Lima FET. Temas abordados na consulta de enfermagem: revisão integrativa da literatura. Rev Bras Enferm. 2012; 65(1):155-61.
4.Panzetti TMN, Santana ME, Costa MSCR. Research on cancer nursing cervical the period 2008 to 2013. J. Health Biol Sci. 2015; 3 (1): 46-51.
5.Ferreira SMA, Gozzo TO, Panobianco MS, Santos MA, Almeida AM. Barriers for the inclusion of sexuality in nursing care for women with gynecological and breast cancer: perspective of professionals. Rev Latino-Am Enfermagem. 2015 [cited 2015 July 20]; 23(1):82-9. Available from: http://www.scielo.br/pdf/rlae/v23n1/pt_0104-1169-rlae-23-01-00082.pdf
6.Rosa LM, Misiak M, Marinho MM, Ilha P, Radünz V, Fermo VC. Radiotherapy and brachytherapy in nursing: a bibliometrical review. Cogitare Enferm. 2015 [cited 2015 July 23]; 20 (2):408-16. Available from: http://ojs.c3sl.ufpr.br/ojs/index.php/cogitare/article/view/38866
7.Schutz A. Sobre fenomenologia e relações sociais. Petrópolis (RJ): Vozes; 2012.
8.Zeferino MT, Carraro TE. Alfred Shütz: from theoretical-philosophical framework to the methodological principals of phenomenological research. Texto Contexto Enferm. 2013 [cited 2015 Jun 20]; 22(3): 826-34. Available from: http://www.scielo.br/pdf/tce/v22n3/v22n3a32.pdf
9.Jesus MCP, Capalbo C, Merighi MAB, Oliveira DM, Tocantins FR, Rodrigues BMRD, Ciuffo LL. The social phenomenology of Alfred Schutz and its contribution for the nursing. Rev esc enferm USP. 2013 [cited 2015 July 05]; 47(3):736-41. Available from: http://www.scielo.br/pdf/reeusp/v47n3/0080-6234-reeusp-47-3-00736.pdf
10.Paula CC, Padoin SMM, Terra MG, Souza IEO, Cabral IE. Driving modes of the interview in phenomenological research: experience report. Rev Bras Enferm. 2014 [cited 2015 July 05]; 67 (3): 468-72. Available from: http://www.scielo.br/pdf/reben/v67n3/0034-7167-reben-67-03-0468.pdf
11.Monteiro ACM, Rodrigues BMRD, Pacheco STA. O enfermeiro e o cuidar da criança com câncer sem possibilidade de cura atual. Esc Anna Nery. 2012; 16 (4): 741-6.
12.Vieira LB, Padoin SMM, Oliveira IES, Paula CC. Intencionalidades de mulheres que decidem denunciar situações de violência. Acta Paul Enferm. 2012 [cited 2015 Sep 14]; 25 (3): 423-9. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-21002012000300016&lng=en . http://dx.doi.org/10.1590/S0103-21002012000300016 .
13.Umpiérrez AHF, Merighi MAB, Muñoz LA. Percepções e expectativas dos enfermeiros sobre sua atuação profissional. Acta Paul Enferm. 2013 [cited 2015 Sep 14]; 26 (2): 165-71. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-21002013000200010&lng=en . http://dx.doi.org/10.1590/S0103-21002013000200010 .
14.Rossi CS, Rodrigues BMRD. Típico da ação do profissional de enfermagem quanto ao cuidado familial da criança hospitalizada. Acta Paul Enferm 2010 [cited 2015 Sep 14]; 23 (5): 640-5. Available from: http://www.scielo.br/pdf/ape/v23n5/09.pdf
15.Rosa LM, Radünz R. Therapeutic itinerary in breast cancer: a contribution to the nursing care. Rev enferm UERJ. 2013 [cited 2015 Sep 05]; 21 (1): 84-9. Available from: http://www.facenf.uerj.br/v21n1/v21n1a14.pdf
16.Leite FMC, Ferreira FM, Cruz MSA, Primo CC, Lima EFA. Nursing diagnosis related to the adverse effects of radiotherapy. Rev Min Enferm. 2013 [cited 2015 Sep 05]; 17 (4): 946-51. Available from: http://www.reme.org.br/artigo/detalhes/897
17.Nascimento LKAS, Medeiros ATN, Saldanha EA, Tourinho FSV, Santos VEP, Lira ALBC. Sistematização da assistência de enfermagem a pacientes oncológicos: uma revisão integrativa da literatura. Rev Gaúcha Enferm. 2012; 33 (1): 177-85.
18.Ministério da Saúde (Br). Portaria nº 2.439, de 08 de dezembro de 2005. Institui a Política Nacional de Atenção Oncológica: promoção, prevenção, diagnóstico, tratamento, reabilitação e cuidados paliativos, a ser implantada em todas as unidades federadas, respeitadas as competências das três esferas de gestão. Brasília (DF): Secretária de Atenção à Saúde; 2005.
19.Amador DD, Gomes IP, Coutinho SED, Costa TNA, Collet N. Concepção dos enfermeiros acerca da capacitação no cuidado à criança com câncer. Texto contexto-enferm. 2011; 20 (1): 94-101.