FIGURE 1 : Description of the studies included in the integrative review, according to title, author (s), journal (year, volume), and type of research. 2005-2015.
REVIEW ARTICLES
Evidence and analysis of vulnerability of people with Diabetes Mellitus: potential for care
Anna Carolina dos Santos ChavesI; Lina Márcia Miguéis BerardinelliII; Nathália Aparecida da Costa GuedesIII; Clícia Vieira CunhaIV; Mauro Leonardo Salvador Caldeira dos SantosV
I
Nurse. Master's Student in the Graduate Program in Nursing at the School of Nursing at the State University of Rio de Janeiro, Scholarship holder from the
Coordination for Improvement of Higher Education Personnel, Brazil. Email: carolchavesrj@gmail.com
II
Nurse. Associate Professor, Department of Medical-Surgical Nursing and the Graduate Program of the School of Nursing at the State University of Rio de
Janeiro. Scholarship for the Production, Technical and Artistic Incentive Program (Prociência), State University of Rio de Janeiro. Brazil. Email: l.m.b@uol.com.br
III
Nurse. Master's Student in the Graduate Program in Nursing at the School of Nursing at the State University of Rio de Janeiro, Scholarship holder from the
Coordination for Improvement of Higher Education Personnel, Brazil. Email: nathyyguedes@gmail.com
IV
Nurse. Master's Student in the Graduate Program in Nursing at the School of Nursing at the State University of Rio de Janeiro, Brazil. Email: cliciarebello@gmail.com
V
Nurse. Associate Professor III Nursing School Aurora Afonso Costa at the Fluminense Federal University. Niterói. Brazil. Email: mcaleo@uol.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2015.18416
ABSTRACT
This study to demonstrate and examine the vulnerabilities of people with type 2 Diabetes Mellitus as described in scientific nursing production used integrative review guided by the question: How is the vulnerability of people with type 2 diabetes mellitus expressed in the nursing literature? The Virtual Health Library, Latin American and Caribbean Health Sciences Literature, Medical Literature Analysis and Retrieval System Online, and the Cumulative Index to Nursing and Allied Health Literature were searched, using the combination of keywords 'vulnerability', 'nursing', and 'Diabetes Mellitus type 2', for articles published from 2005 to 2015. When the 8 articles selected were grouped by subject area, two categories emerged: vulnerability and the human condition; and coping with diabetes with health education. It is believed that an understanding of the vulnerabilities will contribute to rescaling health care for people with diabetes mellitus, in such a way as to incorporate the tenets of comprehensive care, including the dimensions of bio-psycho-social welfare.
Keywords: Type 2 Diabetes Mellitus; health vulnerability; nursing; health promotion.
INTRODUCTION
In the different transition processes of the cycles of life, humans are exposed to vulnerabilities, each of them, if expressed differently, depending on the age group, the contexts where they live, and may bring implications for people of all orders. The implications may have an impact on health, wellness and quality of life, causing individual, social disorders, financial expenses, creating moments of progress and setbacks, in which individuals become vulnerable to the various conditions that can hamper the control and improvement of disease1,2.
That way, the vulnerability to disease spread differently, depending on the region, social groups and individuals to be evaluated, so that is related to the social group, the level of education, and access to health services, among others2.
Given its multifaceted concept of vulnerability expressed grave concern, the transversality this theme in different fields of knowledge, in particular, the area of health that come care based on linking humanistic theories in the light of human development in the confrontation of their health situations, especially with regard to the health of people with Chronic Noncommunicable Diseases (NCDs)1.
In this sense, the vulnerability addition to consist of a set of biological, epidemiological, social and cultural factors, their interaction can enlarge or reduce the risk or protection given disease, condition or injury. It is linked to individual and collective, intrinsic and extrinsic factors that may cause increased susceptibility to health disorders or greater coping capacity of the individual to the disease2,3. Therefore, it has three interrelated components: individual, social and institutional programmatic2.
The individual component includes the quality of the information that the individual has on the problem, the ability to develop and incorporate information in their daily lives, as well as the interest and the possibilities of turning them into practices that are aimed at the protection and prevention. The social component refers to the obtaining of such information, which depend not only the individuals, but also of access to means of communication, education, availability of resources and overcoming cultural barriers. The programmatic component includes the resources that individuals need not to expose themselves to situations of higher risk, public policies of prevention and control of diseases, provision of inputs required for protection, commitment of the institutions and programs at different levels of care2.
Vulnerability differs from risk, by its non-probabilistic character, since the risk attempts to express mathematical chances of illness of an individual, when carrier of specific features, and vulnerability expresses the potential for illness/not related to any individual who was living under a particular set of conditions3,4.
In the field of health, the diabetes mellitus (DM) is a major chronic problem of greater repercussions on the global health discussions. Substantially proven data have shown that the people are vulnerable and require follow-up, however, in nursing, not always the results disseminated scientific production in the area they have pointed to the evidence and actions needed in order to minimize the health problems of these people3 .
DM is a metabolic disorder of heterogeneous etiologies characterized by hyperglycemia and disturbances in the metabolism of carbohydrates, proteins and fats, resulting from defects of and/or insulin secretion action4,5.
The latest estimate disclosed in April 2013, indicates that in Brazil there is more than 12 million people affected by the disease. Being in the year 2010, responsible for the deaths of 54 thousand Brazilians, this number four times greater than the deaths caused by Acquired Immunodeficiency Syndrome (AIDS) (12 000), and by traffic accidents (42 thousand), for example6.
In 2014, the World Health Organization (WHO) recorded that the prevalence of the disease was around 8.3% of the world's population and that in 2030 it will be the seventh cause of death5,6. The International Diabetes Federation (IDF) projects that by the year 2035 the world disease cases reach a level alarming of 592 million6. In this sense it is considered a public health problem of global prevalence, booming in virtually all regions of the planet, setting up progressively as a pandemic from the last decades of the twentieth century5,6.
Although type 2 diabetes mellitus (DM2) is a disease that mainly affects older adults, it can be seen that, with the increase of obesity, the age of onset of the disease affects younger age groups, which suggests that diabetes will become one of the most common diseases in the productive age population 5,7. Generating moments of progress and setbacks, in which individuals become vulnerable to the various conditions that can hamper the control, monitoring and improvement of disease.
Thus, this work aims to contribute by pointing out the evidence of the vulnerability of people with type 2 diabetes mellitus described in scientific literature of nursing in nurses, expanding the theoretical discussions, along with reflections to enhance the practice of health care, as well as new objects of research.
To this end, the objectives of the study are: highlight and analyze the vulnerability of people with type 2 diabetes mellitus in the nursing scientific production.
METHODOLOGY
This is an integrative review, the method studying various approaches, bringing together theoretical and empirical literature in order to expand the understanding and understanding of a particular phenomenon or health problem8. So that the categorization of studies and the provision of the findings can be performed through the construction of an instrument which enables the systematization of research, demonstrating a significant amount of data to be analyzed and facilitate the individualized assessment of each work8,9.
In addition, it allows the generation of updated knowledge about a particular research problem and ensure that the knowledge is valid to be transferred to the practice; so the construction of the integrative review should follow methodological rigor standards, which will enable the reader, to identify the characteristics of the analyzed studies and provide basis for advancement in nursing10.
Thus, the following steps were followed: question to revising, establishing the sampling criteria; presentation of the search features; data analysis; interpretation of results and, finally, presentation of the review9,10.
The selected question was: How do you express the vulnerability of people with type 2 diabetes mellitus in the nursing literature? The following were established the criteria for the selection of studies, these being: full article available online , periodic qualified, results of research, experience reports, reviews, and news, in Portuguese, English or Spanish available in electronic media, the cut-off time of the last 10 years (2005-2015). Productions that were excluded fell not on the theme proposed and in the temporal, repeated articles, abstracts of conference proceedings, dissertations, theses, monographs, books, reports, among other documents.
The data were collected in April 2015, in the Virtual Health Library (VHL), in integrated mode with the database of nursing (BDENF), Latin American literature and Caribbean Health Sciences (LILACS), and Medical Literature Analysis and Retrieval System Online (MEDLINE); and Cumulative Index to Nursing and Allied Health Literature (CINAHL) through the Capes Journals using the combined keywords: vulnerability, nursing and type 2 Diabetes Mellitus.
The study of integrative review, as an instrument of evidence-based practice, is characterized as an approach that addresses both the clinical care and for the education based on knowledge and observation of clinical practice quality10.
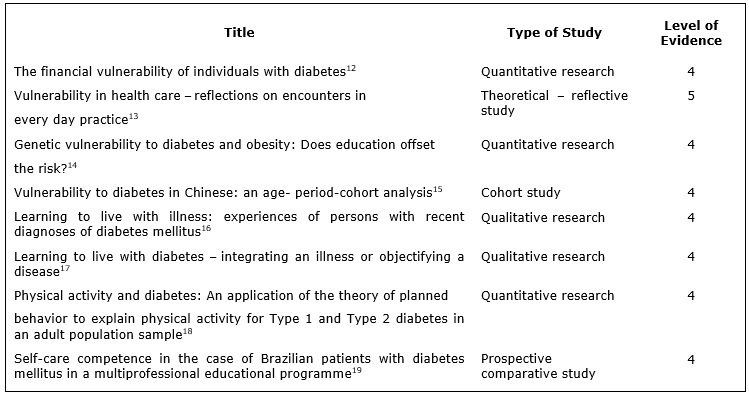
The evidence are classified in hierarchical form for the evaluation of research or other sources of information, is based on the categorization of the Agency for Healthcare Research and Quality (AHRQ) of the United States of America. The classification covers six levels described below: Level 1 - meta-analysis of multiple controlled studies; Level 2 - individual study with experimental design; Level 3 - study of nearly experimental design to study without randomization with one group pre and post test, time series or case-control; Level 4 - study of non-experimental design as correlational descriptive and qualitative research or case studies; Level 5 - report cases or data obtained systematically, verifiable quality or program evaluation data; Level 6 - opinion of respected authorities based on clinical competence or opinion of expert committees, including information not interpretations based on research; regulatory or legal opinions10.
After the selection of the articles, they were arranged in an instrument in order to extract the data from each selected publication, consisting of the following information: Title, authors, periodical published year, volume, research/methodology type, database used10.
Then, the data were organized from the thematic analysis, which is to find the units of meaning that make up a communication whose presence or frequency mean something to the targeted analytical objective, and the theme is the meaning unit that emanates naturally from a text analyzed according to criteria relating to the theory that serves to guide the reading11. To carry out the analysis the data contents were organized and structured with the following the sequential phases: the pre-analysis, exploration of the material and the processing of results11.
RESULTS AND DISCUSSION
In VHL database, 8 articles were found, but only 2 were relevant to theme, however they were not available in their entirety. In the CINAHL database 177 articles were found, being only 8 were available in their entirety and were within the chosen theme. Thus, the final sample consisted of 8 studies, all from the CINAHL database.
Thus, there is a small number of papers available on the vulnerabilities of people with type 2 diabetes mellitus.
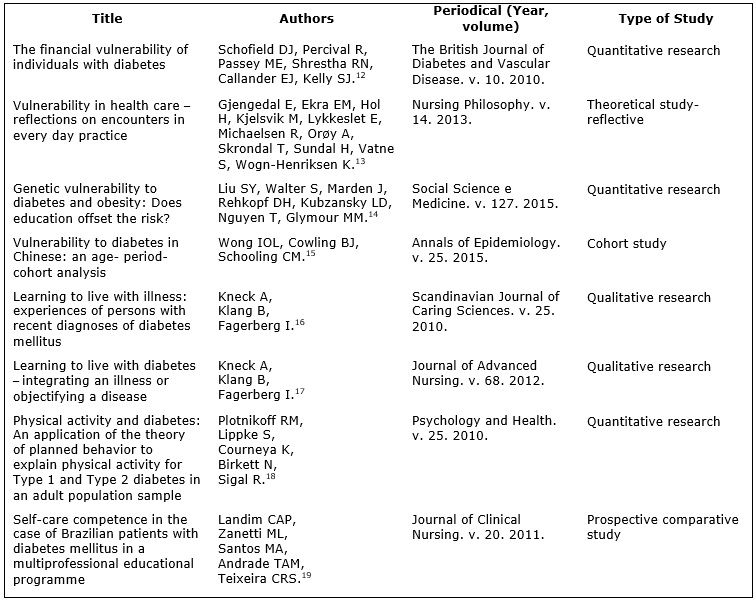
The eight articles were presented according to the title, the authors, periodical, and database and research design12-19as shown in Figure 1.
FIGURE
1
: Description of the studies included in the integrative review, according to title, author (s), journal (year, volume), and type of research. 2005-2015.
Regarding the year of publication, a number of major publications in the year 2010 with three studies12, 16,18, one in 201119, 2012 17, 201313followed by two in 201514,15. As to the authorship of published studies, the authorship of an article to economics12, medicine15, physical education18and 5 nursing articles13, 14, 16, 17,19.
In relation to the methodological research design, in every database and virtual library there are three articles of quantitative research12,14,18 two qualitative research articles13,16, a theoretical study17, a cohort19and a comparative 15. Levels still were observed evidence of each study, as shown in Figure 2.
FIGURE
2: Description of the studies included in the integrative review, according to the research design and evidence levels. 2005-2015.
After the selection of the material, thematic analysis was performed by reading floating and Constitution of the corpus of the articles. The analysis aimed to organize and summarize the data to respond to the problem proposed in this study. In addition, the interpretation sought to associate the described in articles with knowledge more extensive, already obtained on the subject11. From then on, the proximity between the articles and the repetition of themes among them, two categories emerged: Vulnerability and the human Condition and Coping with diabetes Health Education. These categories are discussed below.
Vulnerability and the human condition
The vulnerability of individuals with DM2 was the most prominent theme among the works analyzed, showing diverse perspectives about his concept. Being a term commonly used to describe individuals or groups of individuals12-16. Consisting of the set of biological, epidemiological, social and cultural factors whose interaction enlarges or reduces the risk or protection of a particular disease, condition or injury20-24.
Vulnerability is affected by personal factors as well as environmental and social factors. Trends in society indicate that a growing number of vulnerable people creates additional demands on a healthcare system12-15,25.
People or vulnerable groups are defined as being at risk of physical, psychological and/or health impairment. Although everyone is potentially at risk of physical problems, and in need of psychological health and/or protection, some groups of people have a higher probability of becoming ill. These groups are usually identified as those with low income, unemployed, homeless, chronically ill and people with disabilities, people with AIDS, pregnant adolescents, children, vulnerable seniors, immigrants and refugees, and the mentally ill13- -26 15,24.
Under the phenomenological perspective, it is related to our particular state, and makes us vulnerable when we are exposed to damage, and is related to many intrinsic and extrinsic factors. Often associated with groups of people, like children and adults suffering from chronic diseases13, 14,16.
As with all chronic non-communicable diseases, DM represents an interaction of genetic, lifestyle and environmental factors, whose elucidation facilitates the prevention and control of the disease12-17.
The articles indicated that diabetes prevention must be a priority in order to reduce personal costs of lost savings and wealth, in addition to the load already recognized of excessive morbidity and health care costs associated with the disease and mortality12-15,24. The vulnerability to DM2 was applied for genetics, lifestyle and financial12-15.
It is evident that the vulnerability is not mere reduction of self-determination capacity, but a deeper sense of vulnerability, which is a proper framework that articulates, instead, independently, fairly, prudently, with otherness15, 16, 25,26.
The vulnerability in the individual with diabetes is multifactorial and multifaceted, not just restricted to a question of reduction of the capacity of self-determination13,14. Changing in every circumstance the individual, and may have insights and varying degrees between different individuals and situations14,17.
Understanding the vulnerability of people with DM 2 should be based on plurality of spaces in which people live, as well as the diversity of choice of individuals13, 14, -27 16,24. This understanding will subsidize the mobilization of health professionals and civilian population in search of better living conditions and health with a view to social transformation.
Coping with diabetes with Health Education
Note-this category the articles highlight that despite technological advances in health, a minority of people who live with the DM 2 reach the goals established for the control of the disease. The inability to achieve these objectives increases the risk of developing medium to severe complications, as well as experience the diabetes suffering and anguish17-18.
About that, there is wide variation between countries, governing the Organization of patient education and its integration in the treatment of diabetes. Research over the past decades have indicated that one of the most important aspects of care DM today is the active involvement of people in their own care 17-19,27 -29.
The teaching-learning process includes an internal dialog between the individual and the life, where the focus of motivation should focus on apprehending a new reality and understanding of self, of what can be possible change in lifestyle changes17, 18, 29,30. However, there is dissonance between the level of knowledge acquired and a change in habits and attitudes of patients with DM related to self-care. These findings indicate that the educational programs are not consonants, and thus to improve competences are recommended for diabetes and self-management18.
Self-management consists of a continuous process of facilitation of knowledge, skills and abilities necessary for self-care in diabetes, being a process of teaching people to manage their disease. They add that this process incorporates the needs, goals, and life experiences of the person 17-19,28 -31.
Health education is another factor that affects the vulnerability. Higher levels of education are directly associated with better health. People who have more education tend to access the health system and also practice preventive healthcare actions16-19,29.
Health care professionals are important contributors to this growth process. In nursing, protect patients from harm is an essential element and makes possible the human development16-18,30.
Prevention and health promotion must be a priority, as well as all the programmatic actions, and host all spontaneous demand or not of the individual or group. Focusing on autonomy, built from the perceptions and experiences of the participants, considering the life stories of the people, their values, beliefs and also the current situation that allows monitoring and reconstruction of the health situation of individuals18-20.The training is delegation of responsibility, and the professionals participating as facilitators of this process21- -30 24,28.
DM represents a challenge for both for the person who has, as for family members and health professionals, and therefore, imperative that the health team to adopt new perspectives for the individual and collective care and possible through groups, focused on autonomy of the individual18, 22,24. Health protection strategies in groups are commonly used, and they provide psychological support to deal with the vicissitudes of the treatment, promoting greater acceptance of diabetes and, therefore, an attitude. Being a space for reflection and co-construction of knowledge, encouraging the active search of information and guidance about the disease, aiming at the development of autonomy of individuals16-18; 27-31.
CONCLUSION
This review enabled us to identify the scientific evidence about the vulnerabilities of people with type 2 diabetes mellitus, contemplating the purpose initially proposed and their development.
The literature, in General, has pointed out that the difficulties presented by the diabetic people, for obtaining a good metabolic control, are related to their adherence to a food plan, increased physical activity and follow-up of drug therapy.
The findings are suggestive that also are needed new studies in order to have a better clarification of the vulnerability of the dimensions that are exposed to people with type 2 diabetes mellitus.
It is believed that a better understanding of these vulnerabilities could contribute to resize the health care model with people affected by diabetes, incorporating the assumptions of comprehensive care that include biological, psychological, social and spiritual well-being dimensions among others, advocated the health promotion program.
It emphasizes the need for studies involving other methodologies in order to expand the scope of the vulnerability in type 2 DM, like the narratives of life of individuals in order to produce a crawl in the speeches of subjects and capture qualitative information. In this sense, illuminating the focus of educational practices in health, establishing links with people, involving the protagonists and their families in self-care more efficiently. In addition to expanding the national and international scientific literature on the theme.
REFERENCES
1.Berardinelli LMM, Santos I, Santos MLSC, Clos AC, Pedrosa GS, Chaves, ACS. Cronicidade e vulnerabilidade em saúde de grupos populacionais: implicações para o cuidado. Rev enferm UERJ; 18: 553-58, out.-dez. 2010. Disponível em: http://www.facenf.uerj.br/v18n4/v18n4a09.pdf.
2.Ayres J R CM. Vulnerabilidade e avaliação de ações preventivas. São Paulo: Casa da Edição; 1996. Editoração eletrônica.
3.Ministério da Saúde (Br). Plano de ações estratégicas para o enfrentamento das doenças crônicas não transmissíveis (DCNT) no Brasil 2011-2022. 2011. [citado em 05 mar. 2015]. Disponível em: http://portal.saude.gov.br/portal/arquivos/pdf/cartilha_plano.pdf.
4.Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Estratégias para o cuidado da pessoa com doença crônica: diabetes mellitus / Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica. – Brasília: Ministério da Saúde; 2013.
5.IDH Atlas de Diabetes – Sixth edition. Bruxelas, 2014. Available from: ttps://www.idf.org/sites/default/files/EN_6E_Atlas_Full_0.pdf.
6.Sociedade Brasileira de Diabetes. São 12 milhões de diabéticos no Brasil. São Paulo; 18 abr. 2012.
7.Basarglini, RA. As representações sociais e as experiências com diabetes: um enfoque socioantropológico. Rio de Janeiro (RJ): Fiocruz; 2011. 248p.
8. Souza MT, Silva MD, Carvalho, R. Revisão integrativa: o que é e como fazer [Internet]. 2010; 8(1):102-6. [citado em 02 fev. 2015]. Disponível em: http://apps.einstein.br/revista/arquivos/PDF/1134-Einsteinv8n1_p102106_port.pdf .
9.Ganong LH. Integrative reviews of nursing research. Res Nurs Health 1987 Mar; 10(1):1- 11. Acess for EBSCO host ®.
10.Galvão CM, Sawada NO, Mendes IAC. A busca das melhores evidências. Rev Esc Enferm USP; São Paulo [Internet]. 2003; 37: 43-50. [citado em 02 fev. 2015]. Disponível em: http://www.scielo.br/pdf/reeusp/v37n4/05.pdf.
11.Minayo MCS. O desafio do conhecimento - pesquisa qualitativa em saúde. 14th ed. São Paulo: Hucitec; 2014.
12.Schofield D, Percival R, Passey M, Shrestha R, Callander E, Kelly S: The financial vulnerability of individuals with diabetes. Br J Diabetes Vasc Dis 2010, 10 (6): 300-304.
13.Gjengedal E, Ekra EM, Hol H, Kjelsvik M, Lykkeslet E, Michaelsen R, Orøy A, Skrondal T, Sundal H, Vatne S, Wogn-Henriksen K. Vulnerability in health care – reflections on encounters in every day practice. Nurs Philos. 2013; 14 (2):127-38.
14.Liu SY, Walter S, Marden J, Rehkopf DH, Kubzansky LD, Nguyen T, Glymour MM. Genetic vulnerability to diabetes and obesity: does education offset the risk? Soc Sci Med. 2015; (127): 150-58.
15.Wong IOL, Cowling BJ, Schooling CM. Vulnerability to diabetes in Chinese: an age-period-cohort analysis. Annals of epidemiology. 2015; 25 (1):34-39.
16.Kneck A, Klang B, Fagerberg I. Learning to live with illness: experiences of persons with recent diagnoses of diabetes mellitus. Scand J Caring Sci. 2011, 25:558–66.
17.Kneck A, Klang B, Fagerberg I. Learning to live with diabetes--integrating an illness or objectifying a disease. J Adv Nurs. 2012 Nov; 68 (11): 2486-95.
18.Plotnikoff RC, Lippke S, Courneya K, Birkett N, Sigal R. Physical activity and diabetes: An application of the theory of planned behaviour to explain physical activity for type 1 and type 2 diabetes in an adult population sample. Psychology & Health. 2010; (25): 7-23.
19.Landim CA, Zanetti ML, Santos MA, Andrade TA, Teixeira CR. Self-care competence in the case of Brazilian patients with diabetes mellitus in a multiprofessional educational programme. J Clin Nurs. 2011; 20 (23-24): 3394-403.
20.Barra DCC, Lanzoni GMM, Maliska ICA, Sebold LF, Schlindwein BH. Processo de viver humano e a enfermagem sob a perspectiva da vulnerabilidade. Acta Paul Enferm. 2010; 23: 831-6
21.Oviedo AD, Boemer MR. A pessoa com diabete: do enfoque terapêutico ao existencial. Rev esc enferm USP [Internet]. 2009 Dec [cited 2015 Oct 01] ; 43 (4): 744-751. Disponível em: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S008062342009000400002&lng=en .
http://dx.doi.org/10.1590/S0080-62342009000400002 .
22.Silva KL, Sena RR, Grillo MJC, Horta NC, Prado PMC. Educação em Enfermagem e os desafios para a promoção de saúde. Rev Bras Enferm. 2009; 62: 86-91.
23.Espindola BC, Saboia VM, Valente GSC. Programa educativo em saúde qualidade de vida de indivíduos com diabetes tipo 2: estudo comparativo. UFPE On Line; 2015; 9: 351-9.
24.Santos EI. Vulnerabilidade de enfermeiros no cuidado a pacientes com HIV/AIDS: um estudo de representações sociais [dissertação de mestrado]. Rio de Janeiro: Universidade do Estado do Rio de Janeiro; 2012.
25.Berardinelli LMM, Santos I, Santos MLCS, Lima TCL, Missio AC, Berardinelli LM. Identificando vulnerabilidade para complicações cardiovasculares em idosos: uma estratégia para o cuidado. Rev enferm UERJ. 2011; 19: 541-6.
26.Montez JK, Friedman EM. Educational attainment and adult health: Under what conditions is the association causal? Soc Sci Med. 2015; 127: 1-7.
27.Felipe GF, Silveira LC, Moreira TMM, Freitas MC. Presença implicada e em reserva do enfermeiro na educação em saúde à pessoa com hipertensão. Rev enferm UERJ. 2012; 20: 45-9.
28. Landim CAP, Milomens KMP, Diógenes MAR. Déficits de autocuidado em clientes com diabetes mellitus gestacional: uma contribuição para a enfermagem. Rev Gaúcha Enferm. 2008; 29: 374-81.
29. Luna NSA, Baeza MR, Castell EC, Santos FC, David HL, Castillo MMA. Intervención educativa: implementación de la agencia de autocuidado y adherencia terapéutica desde la perspectiva del paciente diabético. Rev enferm UERJ. 2013; 21: 289-94.
30. Manoel MF, Marcon SS, Baldissera VDA. Estratégias educativas para pessoas com hipertensão arterial e diabetes mellitus. Rev enferm UERJ. 2013; 21: 403-8.
31.Xavier ATF, Bittar DB, Ataíde MBC. Crenças no autocuidado em diabetes: implicações para a prática. Texto Contexto - Enferm. 2009; 18(1): 124-30.