ORIGINAL RESEARCH
Assessing quality of life in the work of general hospital nurses
Leiliane Nascimento dos SantosI; Claudia Teresa Frias RiosII; Ana Hélia de Lima SardinhaIII; Miriam Alves dos SantosIV; Carlos Alberto da Silva Frias JuniorV
I
Undergraduate Nursing student, Federal University of Maranhão, Department
of Nursing. São Luís, Maranhão, Brazil. Email:
leiliane_n_santos@hotmail.com
II
Nurse. PhD in Public Health. Adjunct Professor, Federal University of
Maranhão. São Luís, Maranhão, Brazil. Email: ctfrios@hotmail.com
III
Nurse. PhD in Pedagogical Sciences. Associate Professor, Federal University
of Maranhão. São Luís, Maranhão, Brazil. Email: anahsardinha@ibest.com.br
IV
Undergraduate Nursing student. Federal University of Maranhão. Department
of Nursing. São Luís, Maranhão, Brazil. Email: miriamalves1990@gmail.com
V
Physician. Master in Public Health. Assistant Professor, Federal University
of Maranhão. São Luís, Maranhão, Brazil. Email: frias.jr@uol.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2017.18286
ABSTRACT
Objective: to assess quality of life in the work of nurses at general hospitals in São Luís, Maranhão. Method: in this exploratory, descriptive study, data were collected from January to May 2014 by the standardized Abbreviated Quality of Working Life Questionnaire (QWLQ-BREF) and subjected to descriptive analysis. Results: the 202 nurses interviewed were predominately aged 30 to 39 years, brown, married, with 1-2 children, specialists, care workers, working in an intensive care unit, on the morning shift, working 30 hours weekly and with other employment, and had been in the institutions surveyed for longer than 10 years. Quality of life at work returned a 59.72% rate on the results scale. Conclusion: existing quality of working life at the general hospitals studied achieved satisfactory levels and performed appropriately.
Keywords: Nursing; life quality; work; general hospitals.
INTRODUCTION
In recent years the theme work-related quality of life (WRQoL) of health professionals has attracted growing interest in view of the importance of personal, environmental and organizational factors involved in the work context that directly influence the quality of care provided1.
In the case of nursing professionals in the exercise of their functions, they are usually subjected to numerous negative factors in their work environment which are often characterized as unhealthy and may interfere with their professional practice and quality of life (QoL)2.
In view of the wide representation of women among nursing professionals and the specificities of the feminine gender, as moterhood, breastfeeding, generating, caring and providing for family members, as well as the various roles women take on, we chose to perform this study with nurses3-5.
Researchers point out that poor QoL in one or more dimensions (for example, physical and/or emotional) of health team professionals may compromise service dynamics, generating inadequate service provision, with negative consequences for the institution and, especially, for users2-6. Other studies also point out that QoL indexes can provide information and personal and collective encouragement, with reflections on the excellence of the structure and the service1,2.
A research on these elements allows us to know how people feel about various (both internal and external) aspects of the company and, based on that, to manage this data, transforming this information into the bases for the construction of strategies that promote the increase of quality of life at work2.
In view of the above, the objective of the present study was to evaluate the work-related quality of life of nurses in general hospitals of São Luís - MA.
LITERATURE REVIEW
There are few concepts attributed to good QoL. It is difficult to reach an unanimous opinion among people in the same community, and it is nearly impossible in an entire society. However, there are some elements that are present in most opinions: safety, happiness, leisure, health, stable financial condition, family, love and work7.
The concept of QoL was introduced in the health area in the early 1970s through five strands: epidemiologically based studies on happiness and well-being, which consisted of research on how people felt about themselves and about everything around them; search for social indicators, such as indicators of development, health and education; insufficiency of the objective measures of health outcome, since the existing measures evaluate rather the disease instead of the patient himself; positive psychology, which besides illness, deals with variables of human life such as courage, hope, wisdom, spirituality and creativity; patient satisfaction and humanization of health care, seeking to re-establish the interaction between physicians and clients as the main factor in the success of treatments8.
Since the 1980s, there has been an outbreak of studies on worker's health, which is now conceived as a field of knowledge. As a consequence, the scientific productions related to the theme have increased. Thus, occupational health has come to be understood as an important strategy not only to guarantee workers' health, but also to contribute to motivation and satisfaction at work, productivity, product quality and, consequently, general improvement in the quality of life of individuals and of society as a whole9.
After the Industrial Revolution, women left private spaces (home, husband, children) and came to act in public spaces, assuming various professions. Women initially sought out activities consistent with their abilities. Thus, they assumed professions such as teaching and nursing, for which they considered themselves more prepared, and also because they were the most accepted by society. However, the woman-work-family relationship was never harmonious; conflicts were always present10.
The same study also emphasizes that the multiple roles assumed by the majority of women in professional practice tend to take them to certain situations where they feel powerless and frustrated by not being able to reconcile their many tasks. Moreover, when they arrive at their working place, they have to face difficulties that are often not on their responsibility to solve10,11.
In the nursing work in hospitals, it can be observed that nurses may be exposed to intensely unhealthy work environments, both in the material and subjective sense. Because they are subjected to precarious working conditions and poor quality of life, they are exposed to situations in which the preservation of health may be impaired12.
Considering also that they spend a great deal of time at work, due to the multiplicity of jobs and long working hours, the attempt to reconcile domestic problems with labor ends up becoming a constant source of stress and setbacks1.
In this way, the hospital, in general, is recognized as an unhealthy, a source of distress, and a dangerous environment for those who work there. It is known that the nursing team represents the largest workforce in hospitals and is continuously subjected to situations generated by the activities inherent to their role, involving innumerable negative elements promoted by an environment that is characterized by the presence of illnesses2.
Since nursing is responsible for human care, it is extremely important to seek actions aimed at the care of these professionals, in the sense of promoting their health and improving their professional performance13,14.
METHODOLOGY
This is an exploratory descriptive research with a quantitative approach carried out in hospitals characterized as General Hospitals linked to the Unified Health System (SUS), according to the National Registry of Health Establishments (NRHS) in São Luís - MA, of which six hospitals stand out: one in the federal level, two in the state level, and three in the municipal level. The sutyd was held in the period from January to May 2014.
The NRHS also makes names, functions and other data of employees of the health facilities available. Therefore, a list with the names of all nurses presented in alphabetical order, with their workload in the general hospitals above mentioned was consulted. The list had a total of 510 nurses, but as there were repetitions of the names of some professionals who worked there, 459 nurses working in the selected hospitals were included in this study. The NRHS listing was out of date at the moment of data collection, resulting in the exclusion of 200 nurses who were still registered but who were retired, exonerated or removed from hospitals.
According to the exclusion criteria, the following cases did not participate in the survey: one nurse who had been working for less than a year, 45 who were on vacations, sick leave, premium or mathernity leave, and 11 who refused to participate in the research. Therefore, the research sample consisted of 202 nurses.
Two questionnaires were used to collect data: the first, a questionnaire for the identification of socio-demographic and professional aspects, composed of 12 items and structured with multiple questions; and the second, a specific and short-term instrument for assessing work-related quality of life (QWLQ-bref)15.
The short version - QWLQ-bref consists of 20 questions taken from the orginal 78 that make up the Quality of Working Life Questionnaire ( QWLQ-78). There are four questions in the physical/health domain, three in the psychological domain, four in the personal domain and nine in the professional domain16.
The analysis of the results of the QWLQ-bref follows the same form as that of the questionnaire that originated it - QWLQ-78, in which the author of the instrument prepared a classification scale for the WRQoL. In this classification, satisfactory rates of QoL start at the score 5511.
The questionnaire was applied during the work shift of the participants, after scheduling, following a pre-established scale. The data collected composed the database for later analysis.
For the treatment of socio-demographic data, the Epi Info™ was used. This software allows the data to be managed and analyzed in an organized way, with provision of reports and statistics. For the analysis of the data of the QWLQ-bref, a tool for calculation in the Microsoft Excel software for Windows was applied16.
According to the recommendations of Resolution 466/12 of the National Health Council (NHC), nurses were clarified about the purpose of the research, and those who agreed to participate signed two copies of an Informed Consent Form, one kept by the participant and the other given to the researcher. The project of this research was appraised and approved by the Ethics Committee in Research with Human Beings of the Federal University of Maranhão Foundation, under Opinion nº 509,129.
RESULTS AND DISCUSSION
The research data revealed that 75 (37.1%) subjects in the sample were between 30 and 39 years old and 54 (26.7%) were between 40 and 49 years old, indicating that the functional team is composed of people with more experience. However, a balance in this distribution is still important, considering that younger people bring new ideas, up-to-date knowledge, and they renew the energy in the institution17. It is also noteworthy that 36 (17.8%) nurses were in the age group 50-59, which confirms the dictates of contemporary society - individuals must remain active and productive, delaying retirement as much as possible.
It was verified that, in relation to color/race, the group of self-reported brown people - 110 (54.5%) - predominated in the sample, followed by white - 66 (32.7%) - and black - 13 (6.4%).
Information on the marital status of the nurses in this study indicated a predominance of married women, 94 (46.5%), over single women, which were 70 (34.7%). These results coincide with those of other surveys conducted with nursing professionals, in which the majority was married18,19. In another article, marital status influenced the psychological domains, level of independence, social relations and environment, in which individuals who had companions presented better quality of life (QoL) scores compared to those who did not5.
The majority had 1 to 2 children - 109 (54%) and 65 (32.2%) did not have children. Nurses who are mothers may face difficulties in reconciling the maternal and professional roles, as well as other women in the labor market; but in the case of nursing, the conditions of the profession such as long hours and night shifts particularize this condition by the experience of personal conflicts, because the women can not give the due attention to their children or devote more time to the profession. However, the same research reveals that nurses who are mothers presented better QoL, emphasizing that being a mother is a source of pleasure and personal fulfillment, and personal achievements are determinant in the concept of QoL10,12.
With respect to vocational training, this article points out that 174 (86.1%) participants had specialization, and only 1 (0.5%) had PhD degree. When nurses active in the area of care seek further degrees, they are looking for professional qualification through the search of knowledge; this also has to do with the search for better financial conditions to achieve better living conditions18.
The data on the time working in the nursing area indicate that 116 (57.4%) nurses had been working for more than 10 years. Still, 78 (38.6%) had been working in the same institution for more than 10 years, indicating a low rate of turnover. It is known that the longer a professional works in a single unit, the more knowledge about norms and routines of such unit gains the person. There are certain situations that are better handled and the adaptation is already consolidated, which promotes more safety to the nurses. On the other hand, novice nurses do not have mastery, confidence and complete knowledge of the situations they face, and because of that, they end up tending to isolate themselves, and do not project themselves in the face of challenging situations for fear of for not knowing how to overcome the difficulties18,20.
Of the nurses studied, 123 (60.9%) perform care activities, that is, they carry out activities directly linked with patient care.
Information was obtained regarding the sectors where the professionals work as a way of obtaining reliable data about WRQoL. This aspect is relevant, considering that the nurses' perception about their quality of life is influenced by the specificities of each sector.
The intensive care unit (ICU) has a larger number of active nurses - 42 (20.8%) - as well as the morning shift - 80 (39.6%). These findings are closely related to the number of employees in each sector and the accessibility to employees. Research with nursing professionals working in closed hospital sectors indicates that they suffer with the demand at work, emergency situations, occupational hazards, precariousness of material resources, lack of qualified personnel, work overload, interpersonal relational conflicts and progressive exposure to these factors considered as stressors, leading to physical and emotional burnout, interfering with the quality of life21.
On the other hand, another study emphasizes that ICUs present also factors that reduce stress and tension, among them the closer interpersonal relationships between professionals and the more direct contact with users, which is something that increases self-realization and self-esteem, as well as a more organized environment, better equipped with quality material resources, and well-qualified human resources. Greater possibility of personal and professional aknowledgement is possible in ICUs22 .
Most of the professionals acted in the morning shift in this research. This can be explained by the ease of access to the institution and professionals in this time of the day. Nighttime data collection was hampered by the need to staying late into the night, waiting for the nurses to complete the procedures and slow down the work pace to respond to the questionnaire. It is known that in the night service the number of employees is reduced, and this implies further burden to nurses. As morning shifts have a greater number of employees, nurses were more accessible and available to participate in the research.
The data show that 82 (40.6%) nurses had a workload of 30 hours a week at the institution where they work, and 90 (44.6%) had at least one additional job. Still, more than half - 131 (64.9%) - of the nurses studied have a workload of at least 60 hours per week. The issue of excessive workload is exacerbated by the fact that nurses face professional precariousness, including low wages that lead them to take on more than one job in order to maintain an adequate standard of living18,19.
It is understood that there is a great gap between the desired WRQoL and the experienced WRQoL. The later is marked by double work shifts per day and, in some cases, even triple work shifts, and other factors such as overload of activities; low wages; lack of material resources; poor physical-functional structure; reduced staffing; and physical and psychological illness of the nursing professionals that lower the WRQoL23,24.
As for the evaluation of the nurses' WRQoL, 202 QWLQ-bref. questionnaires were given to be answered among participants of this research; however, 198 were returned with answers, but 4 were returned non-answered. In this case, it is important to note that not all of them were fully answered by the nurses; this caused some missing values , responsible for the divergence observed in the total frequencies. This resource allowed the use of all returned questionnaires, despite those partially answered, without affecting the statistical analysis; an average of 198 observations out of a total of 202 respondents was obtained for each variable of the QWLQ-78 questionnaire.
WRQoL was assessed by the mean of the four domains considered in the instrument, standard deviation, coefficient of variation, minimum value, maximum value and amplitude, of each domain - physical/health, psychological, personal and professional domain - and overall quality of life at work.
For the analysis of frequencies and descriptive measures of the questions, the scores are given on a Likert-type scale, from 1 to 5, where 1 and 2 represent a negative evaluation, 3 intermediate evaluation, and 4 and 5 express a positive evaluation. As a parameter for analysis of the obtained data, the following scores and concepts were observed: scores up to 22.5 were considered very unsatisfactory; between 22.5 and 45, unsatisfactory; between 45 and 55, neutral; between 55 and 77.5, satisfactory; and above 77.5, very satisfactory16.
According to the findings of this research, the WRQoL of nurses working in the general hospitals of São Luís - MA, evaluated by the instrument QWLQ-bref, presented the mean score of 59.72% (3.38 ± 0.47), which represents an opinion of satisfaction.
It is worth emphasizing that stress in the opinion of some authors represents an important aspect in the physical/health domain, since the various symptoms, such as headaches, stomach pain and lower back pain, certainly decrease the workers' ability to concentrate in the task, thus reducing their WRQoL25,26. The professional domain addresses organizational aspects and attitudes that can influence the workers' quality of life. They are dependent on the working conditions, the benefits offered by the company and their social responsibility. Therefore, they do not depend solely on themselves to improve their WRQoL in these aspects15.
The psychological domain - 59.72% (3.38
![]() 0.62), which addresses all aspects related to personal satisfaction,
motivation at work and self-esteem of workers, and the personal domain -
67.68% (3.70 ± 0.53), which covers family aspects, personal religious
beliefs and cultural aspects that influence the work of professionals, both
remained above the total WRQoL result.
0.62), which addresses all aspects related to personal satisfaction,
motivation at work and self-esteem of workers, and the personal domain -
67.68% (3.70 ± 0.53), which covers family aspects, personal religious
beliefs and cultural aspects that influence the work of professionals, both
remained above the total WRQoL result.
A graphical simulation with a scale varying from 0 to 100% of average scores of each domain and the WRQoL of the nurses working in the General Hospitals of São Luís - MA are shown in Figure 1.
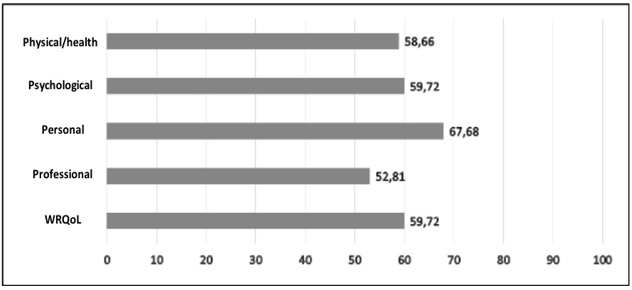
FIGURE 1:
Average scores of domains and WRQoL of nurses. São Luís – MA, 2014.
According to the Results Scale of the QWLQ-bref, the nurses working in the general hospitals of São Luís - MA presented a satisfactory WRQoL, with a score of 59.72%. Although the professional domain was in the neutral range, most domains were within the satisfactory range of the scale (55 to 77.5). Another study diverges from the present result in that its participants were dissatisfied at work and the causes were mainly related to the lack of recognition of the profession, the difficulties of interaction and low remuneration27.
The average obtained in the four domains revealed a WRQoL score in the institutions of 3.389, which in the scale of results of the instrument is classified as satisfactory, equivalent to the score of 59.72% obtained on the centesimal scale of the same method. However, this result is close to a neutral range.
CONCLUSION
In conclusion, the WRQoL within the general hospitals studied reached satisfactory scores.
Among the domains, the one that had more relevance was the personal, followed by the psychological, physical/health and the professional. Based on the results of this research, it can be inferred that nurses enjoy good social, family and cultural relations, although the institutional interventions to promote good results were close to the neutral range in the scale of results of the QWLQ-bref.
The present study had limitations, because the list acquired from the register of nurses working in the general hospitals linked to SUS, provided by the NRHS, was outdated.
It is recommended that this study be replicated to all nursing staff, or even to other health professionals, with a qualitative approach, so as to survey more information about QoL and its relation to work. It is hoped that this article may contribute to the improvement of WRQoL among the hospital nursing workers.
REFERENCES
1.Kimura M, Carandina DM. Desenvolvimento e validação de uma versão reduzida do instrumento para avaliação da qualidade de vida no trabalho de enfermeiras em Hospitais. Rev esc enferm USP. 2009; 43(Esp): 1044-54.
2.Pizzoli LML. Qualidade de vida no trabalho: um estudo de caso das enfermeiras do Hospital Heliópolis. Ciênc saúde coletiva. 2005; 10(4): 1055-62.
3.Spiller APM, Dyniewiez AM, Slomp MGFS. Qualidade de vida de profissionais da saúde em hospital universitário. Cogitare enfermagem. 2008; 13(1): 88-95.
4.Almeida RS, Araújo MAN. Qualidade de vida dos profissionais de enfermagem na unidade de terapia intensiva de um hospital de grande porte do município de Dourados-MS [monograph]. Universidade Estadual do Mato Grosso do Sul; 2010.
5.Fernandes JS, Miranzi SSC, Iwamoto HH, Tavares DMS, Santos CB. Qualidade de vida dos enfermeiros das equipes de saúde da família: a relação das variáveis sociodemográficas. Texto contexto – enferm. 2010; 19(3): 434-42.
6.Paschoa S, Zanei SSV, Whitaker IY. Qualidade de vida dos trabalhadores de enfermagem de unidades de terapia intensiva. Acta Paul. Enferm. 2007; 20(3): 305-10.
7.Gonçalves A, Vilarta, R. Atividade física e qualidade de vida: explorando teoria e prática. Rio de Janeiro: Editora Manole; 2004.
8.Fleck MPA. Problemas conceituais em qualidade de vida. Porto Alegre: Artmed. 2008; 21(1): 19-28.
9.Neves MJAO. Influência do trabalho noturno na qualidade de vida do enfermeiro. Rev enferm UERJ. 2010; 18(1): 42-47.
10.Spindola T, Santos RS. Mulher e trabalho – A história de vida de mães trabalhadoras de enfermagem. Rev. Latino-am. Enfermagem. 2003; 11(5): 593-600.
11.Chaves LD, Ramos LH, Figueiredo EN. Satisfação profissional de enfermeiros do trabalho no Brasil. Acta Paul Enferm. 2011; 24(4): 507-13.
12.Elias MA, Navarro VL. A relação entre o trabalho, a saúde e as condições de vida: negatividade e positividade no trabalho das profissionais de enfermagem de um hospital escola. Rev Latino-Am Enfermagem. 2006; 14(4): 517-25.
13.Silveira MM, Stumm EMF, Kirchner RM. Estressores e coping: enfermeiros de uma unidade de emergência hospitalar. Rev Eletr Enferm. 2009; 11(4): 894-903.
14.Zavala QOM, Klijn TMP.Qualidade de vida no trabalho da equipe de enfermagem. Rev bras enferm. 2014; 67(2): 302-5.
15.Reis Junior DR. Qualidade de vida no trabalho: construção e validação do questionário QWLQ-78 [master degree]. Universidade Tecnologia Federal do Paraná; 2008.
16.Cheremeta M, Pedroso B, Pilatti LA, Kovaleski JL. Construção da versão abreviada do QWLQ-78: um instrumento de avaliação da qualidade de vida no trabalho. Revista Brasileira de Qualidade de Vida. 2011; 3(1): 1-15.
17.Moura LLF. Qualidade de vida no trabalho: uma aplicação prática do modelo de walton no contexto de uma empresa em Picos [monograph]. Universidade Federal do Piauí, 2011.
18.Oliveira FDM. Qualidade de vida de enfermeiras e sua relação com o cuidado clínico de enfermagem [master degree]. Universidade Estadual do Ceará; 2013.
19.Cacciari P, Haddad MCL, Vannuchi MTO, Marengo RA. Caracterização sociodemográfica e ocupacional de trabalhadores de enfermagem readaptados e readequados. Rev enferm UERJ. 2013; 21(3): 318-23.
20.Valadares GV, Viana LO. Vivendo o choque da realidade: a inserção do enfermeiro na especialidade. Rev enferm UERJ. 2009; 17(1): 81-5.
21.Carvalho DV, Lima FCA, Costa TMPF, Lima, EDRP. Enfermagem em setor fechado – estresse ocupacional. Rev Min Enferm. 2004; 8(2): 290-4.
22.Pereira MER, Bueno SMV. Lazer – Um caminho para aliviar as tensões no ambiente de trabalho em UTI: uma concepção da equipe de enfermagem. Rev Latino-Am Enfermagem. 1997; 5(4): 75-83.
23.Neumann VN, Freitas EA. Qualidade no trabalho: Percepções da equipe de enfermagem na organização hospitalar. Rev Min Enferm. 2008; 12(4): 531-7.
24.Farias SNP, Zeitoune RCG. Qualidade de vida no trabalho de enfermagem. Esc Anna Nery; 2007;11(3): 487-93.
25.Nahas MV. Atividade física, saúde e qualidade de vida: conceitos e sugestões para um estilo de vida ativo. 2. Ed. Londrina: Midiograf, 2001.
26.Limongi-França AC. Qualidade de vida no trabalho: conceitos e práticas na sociedade pós-industrial. São Paulo; Atlas; 2004.
27.Versa GLGS, Matsuda LM. Satisfação profissional da equipe de enfermagem intensivista de um hospital de ensino. Rev enferm UERJ. 2014; 22(3): 409-15.