FIGURE 1: Social representation of professional autonomy of nurses to non-nurse health professionals -Rio das Ostras-RJ, 2015.
RESEARCH ARTICLES
Social representations of nurses' professional autonomy among non-nursing health personnel
Érick Igor dos SantosI; Yasmin Rayanne AlvesII; Antonio Marcos Tosoli GomesIII; Raquel de Souza RamosIV; Aline Cerqueira Santos Santana da SilvaV; Caren Camargo do Espírito SantoVI
I
PhD student and Master in Nursing from the State University of Rio de Janeiro Assistant Professor, Department of Nursing, Fluminense Federal University,
Rio das Ostras. Rio de Janeiro, Brazil, E-mail: eigoruff@gmail.com
II
Nursing Student of the last period at the Fluminense Federal University, Rio das Ostras. Rio de Janeiro, Brazil, E-mail: yasmin_bz_@hotmail.com
III
Post-Doctorate in Nursing and Professor at the Rio de Janeiro State University Nursing School. Brazil. Email: mtosoli@gmail.com
IV
PhD in Nursing from the State University of Rio de Janeiro. Nurse of the National Cancer Institute and the Pedro Ernesto University Hospital, Rio de
Janeiro. Rio de Janeiro, Brazil, Email: kakelramos@gmail.com
V
PhD in Nursing from the Federal University of Rio de Janeiro. Assistant Professor, Department of Nursing, Fluminense Federal University, Rio das Ostras.
Rio de Janeiro, Brazil, Email: alinecer@globo.com
VI
PhD student in Nursing from the State University of Rio de Janeiro. Graduate Course professor at the Gama e Souza Nursing School, Rio de Janeiro. Brazil.
Email: carencamargo.enf@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2015.17944
ABSTRACT
This exploratory, qualitative, descriptive study examined the social representations of nurses' professional autonomy held by non-nursing health personnel at a public hospital in the Lakes Region of Rio de Janeiro State in 2015. On an approach structured by Social Representations Theory and Method, 53 health professionals responded to a free evocation form by verbalizing the first 5 words suggested them by the stimulus-term nurses' professional autonomy. EVOC 2003 software was used. The probable central core of the representation comprised the evocations care, team and responsibility, which expressed strongly image-rich and evaluative dimensions. Most of the subjects acknowledged that nurses have professional autonomy. It was concluded that the group's position is essentially favorable to the object represented. But the shortage of affective and practical dimensions reveals that this representation is still in the process of consolidation.
Keywords: Professional autonomy; nursing; nurses; psychology, social.
INTRODUCTION
In nursing, professional autonomy is a complex theme, whose need for more detailed exploitation stems from the current configuration of the work of nurses within hospitals, which increasingly has gained new contours, new demands, challenges and technologies, but which sometimes hold practices still centered in the biomedical model1-5.
The profession, in their historicity, used knowledge from common sense to define their doing, but this feature has been minimized by the continuous pursuit of theoretical and technical-scientific improvement, embodied, above all, by the development and application of nursing theories, in which they represent an important trait of the knowledge of nursing itself3-6.
Given the political, scientific and legal transformations of nursing, nursing itself, the nurse and the autonomy of the professional nurse have been increasingly reflection objects discussed for both nursing professionals as for other health professionals6-10.
Defined as the guiding question of this study is, "What are the social representations of the professional autonomy of nurses from the perspective of non-nursing health professionals?" The objective sought to analyze the representations of the professional autonomy of nurses produced by non-nursing health professionals.
This study is relevant for contributing to the understanding about the visibility of nursing, especially of the nurse in their health care practice, their work and the results achieved over time6-9. The investigation of professional autonomy, even in the psychosocial level, is able to provide the substrates to increase its concreteness in health institutions8-10.
LITERATURE REVIEW
In the healthcare field, professional autonomy lies in an arena of theoretical discussions, methodological and policy involving, on the one hand, the trend of multi work, inter- and transdisciplinary, namely the defense of the provision of assistance to users of the Unified Health System (SUS) almost exclusively as a team and the result of collective work. On the other hand, there is the urgency imposed on the health professions in the current century¹ for establishing and disclosing their professional identity, putting in evidence their specificities, potential and limits of action and decision making, or suffer losses by possible new knowledge production inertia and finally disappear in the total number of fields of knowledge which already have historical tradition or are emerging, but that meet effectively and quickly to current social needs2.
Means for the expression of professional nursing autonomy when it professional, endowed with moral and intellectual independence, enjoys the ability to govern themselves by their own means and makes decisions as freely as possible, establishing, under mainstay of technical and scientific knowledge, their individual or collective practice3-5. The conceptual approach of professional autonomy is hampered by its non-linear relationship with other concepts of equal complexity, power, freedom, independence, self-identity/role and nursing, per si.
Theoretical-conceptual complexity aside, it should be noted that the professional autonomy to be treated in this research is an object of resignification of the health professionals. It is assumed that, in the context of the hospital there is coexistence assignment of meaning for the professional nurse autonomy by health professionals, be they nurses or not, as well as for patients who experience the care. It is argued, therefore, that the professional autonomy of the nurse is an object of social representation for generating a body of knowledge, affectivity, attitudes and practices related to nursing, professional identity, their decision-making and freedom of action³.
THEORETICAL-METHODOLOGICAL REFERENTIAL
This is a descriptive study, exploratory, qualitative approaches and delineated by means of the theory of social representations8 in its structural approach8.11 -13.
The survey was conducted in the period between March and April 2015 in a municipal hospital located in the Lakes Region of the State of Rio de Janeiro-RJ, Brazil. The institution has a maternity ward, internal medicine, obstetrics clinic, surgical clinic, pediatrics, intensive care center, surgical center and sterile material center.
All healthcare professions were included (except nursing) and have more of a professional, since it is necessary to have more than one subject so that there is social interaction required for the effect of symbolic exchanges, which constitutes itself as a premise elaboration of social representations 11-13.
The defined inclusion criteria were qualified as a degree in any area of health; worked for at least six months in the scenario; find themselves working in the graduate training area at the time of data collection and be over eighteen, with no age boundary. Since the exclusion criteria were the presence of cognitive limitations or communication that make it impossible to collect data; interns, residents or others who do not have employment with the institution and being a nurse.
The convenience sample was defined considering the totality of professionals by area, being subtracted those who met the criteria for exclusion were unavailable or refused to participate in the research, without losing sight of the minimum number of subjects required for retrieval of representations on the structural theory approach11-13.
Afterwards, they participated effectively through the sociodemographic questionnaire to characterize the subjects and the technique of free evocation, 9 physiotherapists, 3 psychologists, 8 nutritionists, 6 social workers and 27 doctors, totaling 53 health professionals. Social service and psychology were considered linked to healthcare professions and, therefore, included in the survey sample, by their professional practice in the context of the study setting have character as close to the nurse as for the others. Afterwards, the social service and psychology, as the remaining areas, work on a daily basis in partnership with the nursing staff (in general) and more specifically with the nurse, which provides a space-time of symbolic exchanges in favor of the preparation of representations8.
In compliance with the provisions of resolution No. 466 of December 12, 2012, of the National Council of Health/Ministry of health, the research was submitted to the Committee of ethics in research with human beings (CEPq) of Fluminense Federal University (UFF) and the Rio de Janeiro State University (UERJ), since this study is configured as part of an inter-institutional project between both universities. The study then obtained an approval according to the opinion No. 924,334 (UFF) and No. 939676 (UERJ).
Free evocations were collected with the term inducer professional nursing autonomy. The free evocations collected allowed highlighting the structure of social representations11-13 prepared by the participants. Data collection took place between March and April 2015.
The analysis of the collected material was a first step in standardizing the expressed terms evoked with the same meaning employed a software that could unite them and calculate them much more accurate. Then, we used the software EVOC 2003- Ensemble des programmes permettant l' analyse des evocations, which calculates and reports on the simple frequency of occurrence of each word evoked, the average occurrence of each word by order of evocation, and the average of the weighted average of all the ordered evoked terms12,13.
The presentation of the data was performed by means of the technique of the four quadrants, that is structured through 4 sets of elements. Those located in the upper left quadrant correspond to the possible nuclear elements of the representation, including possibly more significant elements from the perspective of the study subjects. The elements located in the lower left quadrant form the elements of the contrast of the representation, which are low frequency, but elements that have low average order of evocation, i.e. are readily evoked. In the upper right quadrant are the elements that have high frequency, although they are less readily evoked. In the lower right quadrant are the elements of second periphery, less frequent and less readily evoked, which means they are probably the most peripheral elements and more away from the core of the representation12.13.
According to the structural approach and the central nucleus theory of social representations, the four houses is divided into two separate systems, which are a central and the other peripheral. The central system is formed by the central core. However, the peripheral system by the other three quadrants. In short, the central system assigns stability, organization and sense the representation identified. On the other hand, the peripheral system is flexible, integrates new information on the structure of the representation, protects the core, this is not necessarily a consensus within the group and the elements that are participants are more focused on practical and concrete situations.
It starts with the theoretical premise of the structural approach of the social representations theory that the terms that meet at the same time, the criteria of having the highest frequencies, as well as being mentioned first (readily evoked) would have greater importance in social thought participants and would be the likely members of the central core of the representation12,13.
RESULTS AND DISCUSSION
Participant profiles
The participants are mostly female (75.5%), age range of 25 to 34 years (41.5%), profess the Catholic religion (45.5%), with companion (62.3%), with higher level degree of specialist (81.1%) of average income between BR$ 6,000 and BR$ 11,000 (34%), without professional nursing in family (62.3%) and reported having already worked professionally with the nurses in the three levels of health care (49.1%). 69.8% of participants report they have been attended by nurses and 56.5% had access to information about nursing outside the workplace. When asked whether the nurse has professional autonomy 60.4% answered yes and 39.6% answered no.
The representation structure
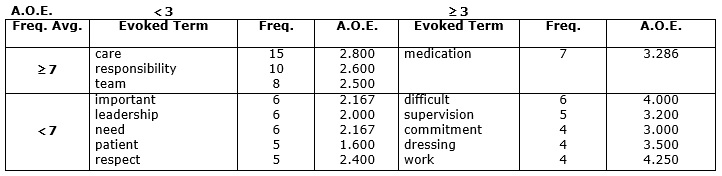
For the term, professional autonomy of nurses, 265 words were evoked, among which 147 were different. The minimum frequency set was 4, being excluded from the composition of the four words with less frequency. The average rate calculated from the remaining terms was 7. The average order of evocation (AOE) was 3.0, on a scale of 1 to 5. Achieving the necessary calculations occurred in the software itself, based on Zipf's Law. The painting of four houses (Figure 1) has been prepared from the previously set parameters. See Figure 1.
FIGURE 1: Social representation of professional autonomy of nurses to non-nurse health professionals -Rio das Ostras-RJ, 2015.
The upper left quadrant is formed by possibly core elements, namely: care, team and responsibility, indicating strong imagery and evaluative dimensions of representation, and, above all, normative character. The normative character of the central core is connected to the system of values of the studied group, consisting of a fundamentally social dimension of the core. However, the functional character focuses on the representation and constitution of the core most important elements for the realization and justification of a task, that is, elements linked to an action11-12.
The core has three functions: generator, organizer and stabilizer, determining, respectively, the meaning, the internal organization and stability of representation. The generating function gives the meaning of the other elements of the representation13.
The word care, expressing the imagery dimension possibly originates in the classic analogy between nursing and care, historically constituted, since care is an integral part of the epistemological foundations of nursing7-9. The word team, outlines again a dimension of representation and imagery indicates that the subject falls within the autonomy of the professional nurse in collective rather than individual context. In this case, probably the subject move the attribute to have professional autonomy nurse to nursing staff, regardless of the legal framework that assigns legitimacy to decisions taken by the nurse on the nursing care.
The term responsibility points to an evaluative dimension of representation, indicating the processes of qualification and attribution of meaning of the autonomy of the professional nurse. The subjects express the idea that the professional autonomy of nurses, in this case, is something that requires commitment.
It highlights that care and responsibility have the highest frequency among the all words mentioned, with 15 and 10, respectively. The evocations that form the core of the representation of the professional autonomy of nurses shows to be a favorable group essentially positioning with respect to professional autonomy of nurses.
The lower left quadrant is also known as contrast zone, which encompasses evocations of low average Order Evocation (AOE), i.e. words readily evoked, but that have low frequency. In it, the words have been identified important, leadership, need, patient respect.
The terms important and need reveal a positive attitude dimension of the subject, which reinforces the inference that there is an effort on the part of the subjects in evaluate professional nurse autonomy and position themselves.
Since the evocation leadership, dimension possibly imagery is tied to the word team this central core, since, by definition, the figure of the leader is always located where there is a set of people under the leadership of a team.
New imagery of dimension has been identified in the representation term patient, which is the one that shows the target care within the hospital. This shows the connection between these two terms present in the framework of four houses. Highlights that the evocation patient has the smaller AOE, which means that this is the most readily evoked in the structure of the representation.
For its part, the word respect indicates the perception on the part of the participants that the conquest of greater degree of professional autonomy on the part of nurses is from the conquest of respect in the presence of other people.
The first periphery is composed by term medication, which shows new dimension of professional nurse imagery. The administration of medications by nurses appears to present as a realization of being autonomous, since this is a common procedure in the hospital environment and highly visible to other health professionals.
The second periphery, below and to the right, is formed by terms less readily evoked and less frequently, so the less important elements for the group studied. It verifies the presence of the terms commitment, dressing, difficult, supervision and work. The termcommitment probably with the term responsibility, which indicate qualities of professional autonomous nurses. The terms dressing and supervision in association to the term medication, point to a more pragmatic and procedural autonomy, revealing the extent of its representation and practice implementing it into the technical aspects of nursing. The evocation work can indicate both the condition for the scope of autonomy, which is the fruit of work on the part of the nurse, as the fact that the workload is intense in the profession. It is, thus, an evaluative dimension of the representation. Finally, it identified the term difficult, which shows a negative attitude dimension arising in latency, but still with low and AOE low frequency.
Theoretical look at the organization of the social thought of the participants
The data indicates be the professional autonomy of the nurse a representative object for health professionals, even though this representation is found still in development. This is because they were identified the three basic components of a representation, representational field, the development of knowledge about the object and a group placement favorable or unfavorable about the same (attitude)12-15. Other studies previously identified the bundling of the nursing profession taking care/caring, especially among nursing professionals, users of health services covered in doctor's waiting rooms of clinics and seropositive patients for HIV14-16.
It shows rich representational field identified, which features numerous and diverse set of images for the professional nurse autonomy and express their realization, revealing a representation with elements of strong imagery, such as dimension care, team, leadership, patient medication. Another representational highly expressive dimension in this research was the attitude. The participants seem to position themselves favorably to nursing and to their professional autonomy, qualifying it to saying the words respect, responsibility, work, need, important commitment. The similarity of these evocations, but with less intensity (less frequently and larger AOE), difficult expresses a dimension too, being a term evaluative essentially negative that appears on peripherally quadrant.
In the structure of the representation was identified the shortage of affective and practical dimensions, which could mean that the representation, despite already owning a likely central core, not yet definitively established and is likely to include new elements according to the context in which those involved included and attach meaning to the nurse, the nursing and their professional autonomy. It is possible, therefore, that it is a non-autonomous representation, and it may be linked to other objects of similar representation.
In the face of crushing social organization of the subject, it should be noted that, in the process of writing a proper positioning on the professional autonomy of the nurse, the subject turn to assessment of professional practices of nurses (more tangible expression of profession) to subsequently displaced them and rebuild them through images that have some meaning to them. In other words, to observe the nurse practice or to ensure the safe and correct execution of dressings, nursing supervision and administration of drugs, other health care professionals develop a positive evaluation of the professional autonomy of the nurse, the satisfactory characteristics and valuing its importance, high dependence and need for respect, constructs a new knowledge formulated on the subject. The result of the (re) construction of the representation object is to convert them into images related to the care / caring a work in teams, which requires leadership, whose aim is the figure of the patient and only in the latter finds purpose.
Three techniques or procedures performed by the nursing staff were evoked by the participants, which is the administration of medicines, bandages and nursing supervision. It is noteworthy that the first two, despite their notorious complexity, are often carried out by technicians or nursing assistants instead of nurses, which could cause confusion of roles by subjects along the representation formulation. However, the evocation of the term supervision refers to the glimpse of nurses specifically, since the supervision of nursing is a private assignment of this professional.
Nursing appears as a social practice ontologically anchored in concern and empathy for each other. Their religious foundations require the profession social expectations as the action of taking care with much dedication, seriousness and commitment, that influence the formation of an identity of nursing and the nurse5,7.
The health work has taken multiple arrangements in recent centuries, and its centrality moved the figure of a professional only for sharing knowledge and co-responsibility among everyone involved in the action of assisting/caring/serving15-16. At the same time, focuses on the setting-health and obviously on nursing, the immediate need to define its own role that they assign essentiality and justify government investment in the area.
The likely objectification11,13 among health professionals from the professional autonomy of nurses in the care team conducted responsibly challenges for higher education institutions (HEIs) to train professionals ready to understand and legitimize the epistemological bases of nursing ethical care targeted and humanized. Equipped with the critical thinking and scientific prowess, in accordance to the technological transformations inherent in the health sector and, lastly, aware and disseminators of a stand-alone profession image, able to govern and make decisions compatible to current social needs assistance. In other words, it is suggested that the undergraduate nursing course curricula to enter or strengthen discussions on professional nursing autonomy, placing it across the course, a vocational training effort focused on the establishment of successful practices that culminate problem-solving and social transformation. In this way, it will be possible to achieve more positive social visibility10 and permanence in the healthcare professions in which political-governmental investments are fundamental.
Finally, from the knowledge of the representations set by social groups involved in nursing care, it will be possible to rethink the technological model of work (education and work), establishing new bases for higher education on the process of caring in nursing, from the requirements negotiated between the subject and the health institutions17,18.
CONCLUSION
It is concluded that composed the likely core of the social representation of nursing for health professionals-nurses the evocations care, team and responsibility, expressing strong imagery and evaluative dimensions. Most of the subjects recognized the existence of professional nurse autonomy, while in the central core of studied showed that there is a positive attitude on the part of health professionals with respect to this object. On the other hand, if the majority of the participants stated that the nurse has professional autonomy, the minority that claims the opposite was still an alarming number.
Despite having achieved its objective, this study has limitations provided for its realization in just a single context, with low number of subjects and the presence of certain degree of social normativity, that is, the data were collected in a context that could have influenced. The completion of this survey required overcoming various difficulties during data collection, mainly offered by the lack of willingness on the part of professionals because of their high workload.
As the main potential, this study may subsidize the elaboration of didactic-pedagogical tools most appropriate to nursing, which is in full development, seeking to consolidate its professional autonomy, especially in terms of visibility and concreteness.
REFERENCES
1.Guevara B, Zambrano GA, Evies A. Worldview in self-care and care of the other. Enferm glob. 2011; 10(21):1-7.
2.Honorato EJSA. A interface entre saúde pública e cibercultura. Ciênc saúde coletiva. 2014; 19:481-5.
3.Santo CCE, Gomes AMT, Oliveira DC, Santos ÉI. Por um caminho de compreensão da construção da enfermagem: uma revisão integrativa da autonomia profissional. R pesq cuid fundam online. 2011; 2:767-70.
4.Moreno-Fergusson ME. Evidência científica y autonomía. Aquichan. 2014; 14:136-7.
5.Stein-Backes D, Stein-Backes M, Erdmann AL, Büscher A, Salazar-Maya A. Significado da prática social do enfermeiro com e a partir do Sistema Único de Saúde brasileiro. Aquichan. 2015; 14:560-70.
6.Moreno IM, Siles J. Pensamiento crítico em enfermeira: de la racionalidade técnica à la práctica reflexiva. Aquichan. 2014; 14:594-604.
7.Simiele MF, Barizon-Luchesi L, Porto F, Oliveira-Sousa T, Silva-Santiago E, Aguiar S. Rito católico e imagem da enfermeira (1957). Aquichan. 2014; 14:109-18.
8.Martinez EA, Souza SR, Tocantins FR. As contribuições das representações sociais para a investigação em saúde e em enfermagem. Invest educ enferm. 2012; 30(1):101-7.
9.Schoeller SD, Leopardi MT, Ramos FS. Cuidado: eixo da vida, desafio da enfermagem. Rev Enferm UFSM. 2011; 1(1):88-96.
10.Avila LI, Silveira RS, Lunardi VL, Fernandes GFM, Mancia JR, Silveira JT. Implicações da visibilidade da enfermagem no exercício profissional. Rev Gaúcha Enferm. 2013; 34(3):102-9.
11.Santos ÉI, Gomes AMT, Oliveira DC. Representações da vulnerabilidade e do empoderamento por enfermeiros no contexto da AIDS. Texto contexto - enferm. 2014; 23:408-16.
12.Costa TL, Oliveira DC, Formozo GA. Qualidade de vida e AIDS sob a ótica de pessoas vivendo com o agravo: contribuição preliminar da abordagem estrutural das representações sociais. Cad Public Health. 2015; 31:365-76.
13.Oliveira DC. Construção e transformação das representações sociais da aids e implicações para os cuidados de saúde. Rev Latino-Am Enfermagem. 2013; 21:276-86.
14.Gomes AMT, Thiengo PCS, Anunciação CT, Oliveira DC, Kestenberg CCF. Representações sociais das atividades da enfermagem junto aos pacientes soropositivos: caracterizando ações e atores sociais. Rev Eletr Enf. [Internet]. 2010 [citado em 29 jul 2015]; 13(1):16-23. Disponível em: http://dx.doi.org/10.5216/ree.v13i1.8712.
15.Formozo GA, Oliveira DC. Representações sociais do cuidado prestado aos pacientes soropositivos ao HIV. Rev Bras Enferm. 2010; 63:230-7.
16.Borges MS, Queiroz LS, Silva HCP. Representações sobre o cuidar e o tratar: o olhar de pacientes e profissionais. Rev esc enferm USP. 2011; 45:1427-33.
17.Oliveira DC, Gomes AMT, Pontes APM, Costa CPM. Construção de um paradigma de cuidado de enfermagem pautado nas necessidades humanas e de saúde. Esc Anna Nery. 2011; 15:838-44.
18.Santos ÉI, Gomes AMT, Oliveira DC, Marques SC, Bernardes MMR, Felipe ICV. Representações sociais elaboradas por enfermeiros que cuidam de pessoas com HIV acerca de sua vulnerabilidade. Rev enferm UERJ. 2014; 22:303-8.