(*)It could be registered more than one type of chronic disease.
RESEARCH ARTICLES
Demographic profile of non-institutionalized elderly and their perception of functional food
Ana Lúcia Félix de PontesI, Luípa Michele SilvaII, Cássia Surama Oliveira da SilvaIII, Luiza Sonia Rios Ascuitti IV, Antonia Oliveira SilvaV, Maria da Conceição Rodrigues GonçalvesIV
I
Nurse. Master degree in the Graduate Program in Nutrition Science from the Federal University of Paraíba. João Pessoa, Paraíba, Brazil. E-mail: ana.lucia.felix@hotmail.com
II
Nurse. Ph.D. student at the Graduate Program in Nursing from the Federal University of Paraíba. João Pessoa, Paraíba, Brazil. E-mail: luipams@gmail.com
III
Nurse. Master degree in the Graduate Program Nutrition Science from the Federal University of Paraíba. João Pessoa, Paraíba, Brazil. E-mail: suramajpa@hotmail.com
VI
Nutritionist. Professor in the Medical Science School of Paraíba. João Pessoa, Paraíba, Brazil. E-mail: luiza.asciutti@terra.com.br
V
Nurse. Ph.D. in Nursing. Professor of the Graduate Program in Nursing of the Federal University of Paraíba. João Pessoa, Paraíba, Brazil. E-mail: alfaleda@hotmail.com
VI
Nutritionist. Ph.D. in Pharmacy. Professor of the Graduate Program in Nutrition Science of the Federal University of Paraíba. João Pessoa, Paraíba, Brazil.
E-mail: raulceica@ig.com.br
VII
Cut out the master´s thesis of Ana Lucia Felix Bridges, entitled Socio-demographic, economic characteristics, eating habits and perception of functional
foods of non-institutionalized elderly, defended in 2012, Federal University of Paraíba-UFPB.
DOI: http://dx.doi.org/10.12957/reuerj.2015.17717
ABSTRACT
The study analyzed demographic profile and perceptions of functional foods among 200 elderly in João Pessoa, Paraíba, Brazil, in 2011. The design was cross-sectional and the approach, quantitative. The analysis used SPSS software, version 19, chi-square test with a p<0.05 significance level. The results were: mostly female, from 60 and 69 to old, earning one minimum wage; and mostly widowers. Eating habits featured 90.5% consumed fruits and vegetables daily; 35,5% reported not eating fried foods and fats; 45% drank more than five cups of liquid; and 51.5% self-rated their state of health as fair. In conclusion, most of the elderly had good knowledge of functional foods and used them often. Their perceptions of functional foods and their eating habits were extremely important to planning future actions, which are essential to health promotion for this population. Keywords: Health; elderly; aging; functional food.><0.05 significance level. The results were: mostly female, from 60 and 69 to old, earning one minimum wage; and mostly widowers. Eating habits featured 90.5% consumed fruits and vegetables daily; 35,5% reported not eating fried foods and fats; 45% drank more than five cups of liquid; and 51.5% self-rated their state of health as fair. In conclusion, most of the elderly had good knowledge of functional foods and used them often. Their perceptions of functional foods and their eating habits were extremely important to planning future actions, which are essential to health promotion for this population.
Keywords: Health; elderly; aging; functional food.
INTRODUCTION
Human longevity has been a riveting question in the first decade of the century 21. Several complex factors interact in the process of aging conceptualizing. It can be conceptualized as a physiological state in which there is a progressive decline in organs function, together with diseases related to age1, reaching a growing number of individuals worldwide.
In less than 40 years, the number of elderly in Brazil went from 3 million in 1960 to 7 million in 1975 and 20 million in 2008; an increase of almost 700% in less than 50 years. Today, Brazil is a country where every year new elderly are incorporated 650,000 to the Brazilian population, and most of them are having chronic diseases and some functional limitations2.
With the aging process, elderly start having peculiar conditions that affect their nutritional status. Thus, processes inherent to the physiological changes of this process, in part, condition the factors involved in the causes of nutritional deficiencies recorded in the elderly population,, and others influenced mainly by the disease and by factors related to socioeconomic situation of the elderly. Therefore, they cannot be considered in its entirety as part of the natural aging process3.
Given this fact and because of the world´s aging population, the scientific community is faced with the greatest need to deepen the understanding of healthy eating habits in promoting and maintaining independence and autonomy of the elderly4.
Based on these and considering the lack of studies on the use of functional foods for the elderly, this researchVII aimed to analyze the demographic profile of non-institutionalized elderly and their perception of functional foods.
LITERATURE REVIEW
The concept of functional foods has its origin in the several eating, healthy and ancient habits from Japan and China. The ancient Chinese, Indian, Egyptian and Greek cultures worked hard with the concept of food, medicine, or therapeutic foods, attributing preventing and/or curing to almost all foods, as well as recognizing the right conditions for preparation and consumption of them including Hippocrates and Galen, who used food daily prescription for curing different ailments5.
Adequate food has fruits and vegetables as components, which contain phytochemicals, polyphenols, flavonoids and essential vitamins for the human body. The intake of these foods is one of the strategies applied to increase life expectancy and delay or reverse the damage associated with the normal aging process, being shown that a diet rich in fruits and vegetables effectively reduces some types of cancer and cardiovascular diseases6. One study showed that resveratrol, tyrosol and hydroxytyrosol, not only activate longevity genes, but they also promote cell survival7. This has helped the realization of studies that seek to encourage the use of foods rich in these substances and others in combat chronic diseases and health problems.
The role of this type of food, based on the regular consumption of fruit, vegetables, whole grains, beans and low-fat dairy, is to optimize nutrition in order to maximize the physiological functions of the elderly and ensure increased health and well-being , bringing as a result the reduction in the risk of developing diseases caused by poor diet, such as nutritional deficiencies and chronic non-communicable diseases (NCDs)8.
Due to the high indices of NCDs, today there is a diet-therapeutic intervention based on reducing the intake of foods high in sugars, fats, sodium and restriction of the use of alcohol. Thus, strategies have been elaborated to increase the consumption of fruits and vegetables, being the program 5 a day one of them, started in the United States and currently implemented in more than 40 countries9,10.
METHODOLOGY
It is a descriptive, cross-sectional design and quantitative approach research, with the participation of 200 elderly people, aged between 60 and 90 years old of both genders. It is noteworthy that 100 elderly are accompanied by the University Hospital Geriatrics Clinic Lauro Wanderley (HU) of the Federal University of Paraíba (UFPB), and another 100 elderly are participants of Living Groups in the Basic Care Program for Elderly (PAPI) , located in the southern city of João Pessoa-PB. The reseach was conducted from May to August 2011, using the Mini Nutritional Assessment (MNA) as a tool11.
The sample was probabilistic, in which all elements of the set have the same chance of being interviewed. To obtain representative data of the south and adjacent area groups, four groups were chosen randomly, three of the southern zone and a neighborhood group adjacent (Castelo Branco II), and the same number of elderly patients in the Geriatric Clinic of HU -UFPB who agreed to participate.
Inclusion criteria were age less than 60 years old; elderly people attending PAPI; elderly with scheduled appointments in the Geriatric Clinic of HU-UFPB, demonstrating interest in the subject and presented cognitive conditions to participate. The respondent, after reading the consent form and have knowledge about the research and clarification of doubts, recorded the signature in that document.
The development of the study followed the ethical precepts disciplined by Resolution 196/96 of the National Health Council12 approved by the Ethics Committee of HU-UFPB under number 725/10 and CAAE 0560.0.126.000-10 520/2010.
The data were collected through individual interviews. Data were analyzed using the Statistical Package for Social Sciences SPSS for Windows version 19.0, analyzed statistically using bivariate analysis and chi-square association (c2).
RESULTS AND DISCUSSION
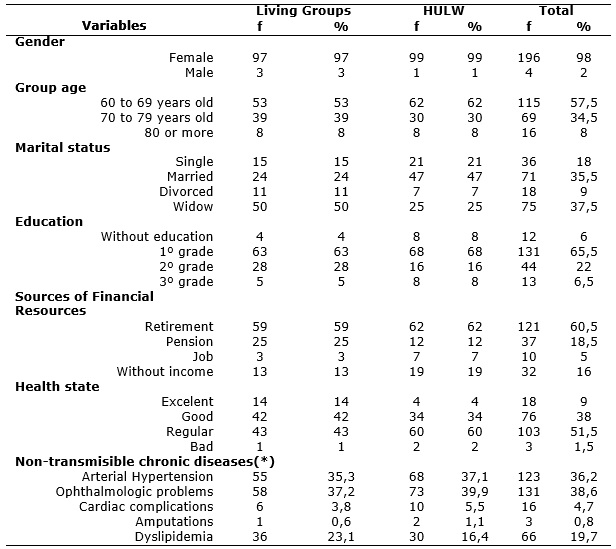
Among the elderly, most of them were female, age group between 60-69 years old, mean age of 68.34 ± age of 6.73 years old and an average family income of a minimum wage; with predominance of widows; most only has primary school education and the most frequent disease was the eye disorder, as shown in Table 1.
The majority reported that their health status was regular, though there was a significant difference between the groups, 43% elderly of the living groups compared to 60% elderly of HULW, according to Table 1.
The elderly participants of living groups showed a statistically significant association between age and ophthalmologic disorders (p=0.021), and participants from HULW had a correlation between the health status and referred to the age group (p=0.035).
TABLE 1: Distribution of sócio-demographic, economic and health variables of the elderly in the Living Groups and HULW. João Pessoa – PB, Brazil, 2011.
(*)It could be registered more than one type of chronic disease.
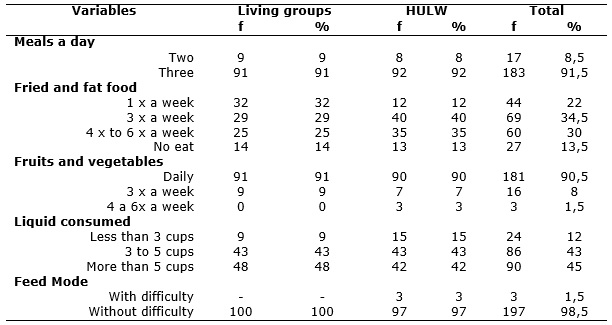
As for the eating habits of the elderly, 91.5% had three meals daily; 90.5% consumed fruits and vegetables daily; 35.5% reported consuming fried foods and fats once a week; 45% drank more than five cups of liquid and the majority (51.5%) reported having a regular health status, being relevant to emphasize that they had autonomy to feed, as shown in Table 2.
It may be noted that the consumption of fried foods and fats was more present among the elderly HULW, than particpants of living groups. It is important to note that only in the hospital 3% of elderly reported having difficulty for feeding.
TABLE 2: Distribution of eating habists of eldery in the Living Groups and HULW. João Pessoa – PB, Brazil, 2011.
Regarding functional foods, 66% of them said to know them and 90% of elderly consume functional foods. When independently visualizing groups, most of the HULW (76%) report having knowledge of these inputs, since the coexistence of groups reported higher consumption (92%), according to Table 3.
TABLE 3: Distribution of knowledge about functional food and its use among ederly of the Living Group and HULW. João Pessoa – PB, Brazil, 2011.

Social and economic profile of subjects
The results bring the predominance of females in the population studied, similar with the trend of feminization of aging, remaining with age advancing 13-15. These elderly, mostly are between the age group of 60 to 69 years old, a phenomenon that can be explained by the gradual growth of this population. The proportion of elderly in 1991 represented 1.3% of the population, with an increase, in 2002, to 1.7%, whose illiteracy rate has decreased, considering that in 1991, 44% of elderly could not read and, in 2002, this ratio was reduced to 33.3% and in 2010, in the city of this present study, the rate was 7.9%13.
Widowhood becomes a common feature among these women, important to note that the loss of the partner and the changes produced in widowhood are considered tragic events or natural in life, which in turn generate profound transformations16.
An important fact observed in this study is the low level of illiteracy recorded4,17, which shows the evolution of the elderly, through investment in education, where they look more for increase their knowledge. Thus, the reduction of illiteracy is due to the improvement of living conditions of the elderly, through community centers, literacy programs for adults and others.
Regarding the financial resources, it is observed that the personal aspirations and the prospect of life of the elderly are met through professional activity. Therefore, the formation of the individual and the work are important issues to be raised when the discussion of retirement. For many elderly, retirement is causing a gradual impoverishment, not only preventing to spend on leisure, but also does not favor a psychological predisposition to practice pleasurable activities; because it is the most constant concern for meeting the basic needs13,15.
In this context, most of the elderly population of this study consisted of retirees and pensioners with a monthly gain of a minimum wage, which could influence negatively on their quality of life and to the acquisition of a healthier diet. It is always an important variable to be highlighted, as in Southern and Southeastern Brazil is that studies show a higher rate of literate in elderly than in the Northeast17,18.
In this study, health status was considered regular in most of the self-assessment, which differs from comparative studies of other groups, as in Portugal 19, although this difference did not reach statistical significance in both studies. However, in this study there was a significant statistic when crossing the age group and the regular health status. In other Brazilian studies, findings show that there are few elderly who perceive negatively their health status20-22.
Among self-reported health conditions, eye disorders showed a high frequency, especially among the elderly participants from community groups, and there is a strong correlation with age. The occurrence of Hypertension (SAH) and Dyslipidemia was also quite high, highlighting the fact of not being old age the only factor for its explanation6,15,23.
SAH is a serious public health problem in Brazil and in the world, considered as one of the most important risk factors for the development of cardiovascular, cerebrovascular and renal disease, accounting for at least 40% of deaths from stroke brain, 25% of deaths due to coronary artery disease, and in combination with diabetes, 50% of cases of renal failure14.
Eating habits in elderly people
These findings emphasize the contribution of living groups, as well as consultations on specific outpatient hospital for the elderly in order to conduct lectures and provide guidance, making this population be more careful with their diet and health, contributing for a better quality of life.
Dyslipidemia is also considered one of the most important risk factors for the development of coronary artery disease in elderly individuals under 80 years old, although this risk decreases with age4. Framingham study data show that the prevalence of hypercholesterolemia (cholesterol Total ≥ 240 mg/dL) in elderly female, is more frequent in the range of 65 to 74 years old, declining gradually after that age24.
In this case, the food also plays an important role in its origin, as well as other changes in the health of this population group. Therefore, nutritional guidance is especially important for the elderly, due to physiological changes related to aging14. For example, meals should be less abundant and distributed, not overloading the stomach of the elderly; They must be prepared to facilitate mastication and allow easy digestion; it is advisable to avoid the use of strong spices and overly fatty and/or hot food served9. It should be stimulating, even those elderly with difficulty feeding, consumption of healthy eating and can meet their nutritional needs3,8.
In the interviews, they were asked how often they ate fatty foods or fried foods. Most of them said they did such intake once a week or not eat fat, confirming several studies4,6,23 that recommendation controlled fat intake, both in patients with hypertension and in healthy people, particularly to avoid increasing complications such as coronary heart disease and obesity9,10.
This analysis agrees with the results of a study in São Paulo, which was researched separately, the daily consumption of fruits and vegetables of São Paulo adults, verifying that 43% of adults consumed fruit daily, 46.8% vegetables and only 18.1% ate legumes25.
In that same approach, one study found that 50% of French adults of both genders consume daily 5 or more servings of fruits and vegetables26. It deserves mentioning that the food has cultural, behavioral and emotional significance, a unique way that can never be neglected. It is noteworthy that a population with higher education and more access to information has a practical consumption of healthy foods and less abuse of drugs such as alcohol every day. Thus, fruits, vegetables, grains and lean meat are included in their dishes; fats, fried foods and sugars appear less in their statements about everyday diet.
Epidemiological studies suggest that people with diets rich in fruits and vegetables have a lower risk of several chronic diseases and early death than people with diets low in these foods. Often this effect is attributed to the antioxidant micronutrients found in plant foods. Antioxidant nutrients, particularly carotenoids in the form of β-carotene has been given with reference to the nutrition of elderly27,28.
In this sense, the factors associated with eating habits have been the subject of several studies, since risk factors for a number of chronic diseases are considered. From this perspective, studies show that regardless of gender, the total caloric diet decreases with age, becoming insufficient in the age group over 60 years old8,9,14.
For all that, geriatric nutrition is especially important because, at this stage, there are different nutritional implications ranging from calorie protein malnutrition, metabolic disorders and drug interactions, to micronutrient deficiencies, which associated with social, economic and psychological factors can contribute to the decline and commitment of several vital body functions28. During the geriatric monitoring, it is important a complete and thorough nutritional assessment, because from there they can identify the elderly at increased nutritional risk for damage to health and establish intervention programs, which should contribute to receive an appropriate nutritional support they need and guidelines about healthy eating29.
Using functional food
As for functional foods and its use among the elderly interviewed, most of them had knowledge of them and take them frequently. The most cited were papaya, banana, orange, apple and oats consumed according to them, for balance of intestine and bones, to prevent cancer and anemia, to help burn cholesterol, among other functions. Increased intake of fruits and vegetables by the population in general has been a priority of public health policy in many countries 30.
These foods have health benefits for their antioxidant activity, promoted by components such as flavonoids, vitamin E, carotenoids, and others that have the ability to neutralize free radicals, which are also responsible for accelerated aging or degenerative disease1.
In this context, functional foods reinforce the salutary effect of substances whose intake through the usual diet is poor. New food trends justify the development of functional foods, due to habits acquired by people who tend to feed on little and poorly balanced in essential nutrients to the body 31.
To stimulate a healthy diet, it is necessary to show the importance of it, and make it to become a routine in their daily routines8. In a study, elderly said to consume daily fruits, vegetables and drank more than five glasses of water a day, very important fact, because diets high in vegetables and fruits have been associated with reduced cardiovascular disease and some cancers9.
The intake of functional foods must be accompanied by a fractional food, as this contributes to the control of satiety and, therefore, the prevention of a metabolic burden, which may be detrimental to digestive problems or the elderly with difficulty in eating. The elderly need greater attention from health professionals as to their fractionation meals, so that there is some suppression of daily food, and in all of them have healthy foods32,33. In this way, they will not only keeping body weight, but helping to prevent health problems.
The benefits of functional foods are focused on several areas, including prevention and treatment of cardiovascular disease, several cancers, diabetes and inflammation, and increased immune response and delayed aging process and extension of healthy life and in this sense a wide variety of bioactive substances of vegetable or animal origin have been investigated for their potential functional and physiological properties.
CONCLUSION
The results indicate that the socio-demographic profile of the elderly is characterized by low education, widowhood and socioeconomic condition of a minimum income; the health condition points to hypertension and eye problems as the main identified NCDs. About the perception of functional foods, it was satisfactory, as well as claiming to know them and use them, the elderly have been accompanied by teams seeking to further improve this understanding and encourage healthy eating, in order to reduce health problems.
It is important to highlight that the elderly stated that the use of functional foods has improved the nutritional status, favoring the acquisition good eating habits such as consumption of more fruits and vegetables and restricting the intake of fat and fried foods, showing satisfaction with the results. In addition to a proper knowledge about functional foods and its use in health promotion, it is assumed that these habits were developed by the elderly, in view of the information received in living groups and specialized care in geriatrics.
Healthy eating and the maintenance of adequate nutritional status are critical factors for healthy aging, so, knowing the perception of the elderly about functional foods and eating habits was extremely important because it enables the planning of future actions, which are essential for the promotion the health of this population.
as study limitations, the scarcity of similar research to enrich the comparisons and the reduced sample and two scenarios that prevent the generalization of the findings can be identified.
REFERENCES
1.Romano AD, Serviddio G, de Matthaeis A, Bellanti F, Vendemiale G. Oxidative stress and aging. Department of Medical and Occupational Sciences, University of Foggia, Italy. J Nephrol. 2010; 23(15):29-36.
2.Veras R. Envelhecimento populacional contemporâneo: demandas, desafios e inovações. Rev Saude Publica. 2009; 43:548-54.
3.Campos MAG, Pedroso ERP, Lamounier JA, Colosimo EA, Abrantes MM. Estado nutricional e antropometria em idosos: revisão da literatura. Rev Med Minas Gerais. 2007;17(3/4):169-70.
4.Fiedler MM, Peres GP. Fuctional status and associated factors among the elderly in a southern Brasilian city: a population-based study. Cad Saúde Pública. 2008; 24(2):409-15.
5.Oliveira MN, Sivieri K, Alegro JHA, Saad SMI. Aspectos tecnológicos de alimentos funcionais contendo probióticos. Rev Bras Cienc Farm. 2002; 38(1): 1-21.
6.Mukherjee S, Lekli I, Gurusamy N, Bertelli AAA, Das DK. Expression of the longevity proteins by both red and white wines and their cardioprotective components, resveratrol, tyrosol, and hydroxytyrosol. Radic Biol Med. 2009; 46:573-8.
7.Sousa KT, Mesquita LAS, Pereira LA, Azeredo CM. Baixo peso e dependência funcional em idosos institucionalizados de Uberlândia (MG), Brasil. Ciênc saúde coletiva. 2014; 19: 3513-20 .
8.Carvalho MM, Lino LLA. Avaliação dos fatores que caracterizam a berinjela (Solanum melongena L.) como um alimento funcional. Nutrire. 2014; 39(1): 130-43.
9.Teixeira PDS, Reis BZ, Vieira DAS, Costa D, Costa JO, Raposo OFF, et al. Intervenção nutricional educativa como ferramenta eficaz para mudança de hábitos alimentares e peso corporal entre praticantes de atividade física. Ciênc saúde coletiva. 2013; 18: 347-56.
10.Gomes FS, Cruz R, Castro IRR. Promoción de frutas y hortalizas en Brasil: la contribución del programa 5 al día. Rev Chil Nutr. 2006; 33(1):295-99.
11.Soini H, Routasalo P, Lagström H. Characteristics of the Mini-Nutritional Assessment in elderly home-care patients. Eur J Clin Nutr. 2004; 58(1):64-70.
12.Ministério da Saúde (Br). Conselho Nacional de Saúde. Comissão Nacional de Ética em Pesquisa. Resolução nº 196 de 10 de outubro de 1996: diretrizes e normas regulamentadoras de pesquisa envolvendo seres humanos. Brasília (DF): CNS; 1996.
13.Instituto Brasileiro de Geografia e Estatística. Primeiros resultados definitivos do Censo 2010. Brasília (DF): IBGE; 2011.
14.Luna RC, Nascimento CC, Asciutti LS, Franceschini SD, Filizola RG, Diniz AD, et al. Relation between glucose levels, high-sensitivity C-reactive protein, body mass index and serum and dietary retinol in elderly in population-based study. Arch of Gerontol and Geriatr. 2012; 54: 462-8.
15.Gonçalves LTH, Leite MT, Hildebrandt LM, Bisogno SC, Biasuz S, Falcade BL. Convívio e cuidado familiar na quarta idade: qualidade de vida de idosos e seus cuidadores. Rev bras geriatr gerontol. 2013; 16: 315-25.
16.Carreira L,Botelho MR,Matos PCB,Torres MM, Salci MA. Prevalência de depressão em idosos institucionalizados. Rev enferm UERJ. 2011; 19: 268-73.
17.Clares JWB, de Freitas MC, Galiza FT, Almeida PC. Necessidades relacionadas ao sono/repouso de idosos: estudo fundamentado em Henderson. Acta Paul Enferm. 2012; 25: 54-9.
18.Pereira GN, Morsch P, Lopes DGC, Trevisan MD, Ribeiro A, Navarro JHN, et al. Fatores socioambientais associados à ocorrência de quedas em idosos. Ciênc saúde coletiva. 2013; 18: 3507-14.
19.Araújo J, Ramos E, Lopes Carla. Estilos de vida e percepção do estado de saúde em idosos Portugueses de zonas rural e urbana. Acta Med Port. 2011; 24: 79-88.
20.Benedetti TB, Petroski EL, Gonçalves LT. Condições de saúde nos idosos de Florianópolis. Arq Catarin Med. 2006; 35(1):44-51.
21.Hartmann ACVC. Fatores associados a autopercepção de saúde em idosos de Porto Alegre [tese de doutorado]. Porto Alegre (RS): Universidade Católica do Rio Grande do Sul; 2008.
22.Carvalho FF, Santos JN, Souza LM, Souza NRM. Análise da percepção do estado de saúde dos idosos da região metropolitana de Belo Horizonte. Rev bras geriatr gerontol. 2012; 15: 285-94.
23.Caetano JA, Costa AC, Santos ZMSA, Soares E. Descrição dos fatores de risco para alterações cardiovasculares em um grupo de idosos.Texto contexto - enferm. 2008; 17:327-35.
24.Moriguchi EH, Michelon E, Vieira JLC. Dislipidemia em idosos. In: Freitas E, Py L, editoras. Tratado de Geriatria e Gerontologia. Rio de Janeiro: Guanabara Koogan; 2002. p:239-48.
25.Figueiredo ICR, Jaime PC, Monteiro CA. Factors associated with fruit and vegetable intake among adults of the city of São Paulo, Southeastern Brazil. Rev Saude Publica. 2008; 42:777-85.
26.Eustáquio C, Druesne-Pecollo N, Latino-Martel P, Dauchet L, Hercberg S, Bertrais S. Socioeconomic diferences in fruit and vegetable consumption among middle-aged French adults: adherence to the 5 a day recommendation. J Am Diet Assoc. 2008; 108:2021-30.
27.Agudo A, Cabrera L, Amiano P, Ardanaz E, Barricarte A, Berenguer T, et al. Fruit and vegetable intakes, dietary antioxidant nutrients, and total mortality in Spanish adults: findings from the Spanish cohort of the European Prospective Investigation into Cancer and Nutrition. Am J Clin Nutr, 2007; 85:1634-42.
28.Kuczmarski MF, Weddle DO. American Dietetic Association University of Delaware, Newark, DE, USA. J Am Diet Assoc. 2005; 105(4):616-33.
29.Azevedo MR, Horta BL, Gigante DP, Victora CG, Barros FC. Fatores associados ao sedentarismo no lazer de adultos na coorte de nascimentos de 1982, Pelotas, RS. Rev Saude Publica. 2008;42(2):70-7.
30.Palanca V, Rodriguez E, Señoráns J, Reglero G. Bases cientificas para el desarollo de com actividad biológica combinada. Alimentos funcionales. Nutr Hosp(Madrid). 2006; 21:199-202.
31.Neutzling MB, Rombaldi AJ, Azevedo MR, Hallal PC. Factors associates with fruit and vegetable intake among adults in a southern Brasilian city. Cad Saúde Pública. 2009; 25:2365-74.
32. Lorga Adalberto, Paola Angelo de, Scatolini Neto Argemiro, Halperin Cidio, Moreira Dalmo, Hachul Denise et al . I Diretrizes do Grupo de Estudos em Cardiogeriatria da Sociedade Brasileira de Cardiologia. Arq Bras Cardiol. 2002; 79(Suppl 1): 1-46.
33. Barbieri AFS, Chagas IA, Santos MA, Teixeira CRS, Zanetti ML. Consumo alimentar de pessoas com diabetes mellitus tipo 2. Rev enferm UERJ. 2012; 20: 155-60.