ORIGINAL RESEARCH
Stress – realities experienced by nurses working in an Intensive Care Unit
Armando dos Santos TretteneI; Rosana Bonete da CostaII; Priscila Capelato PradoIII; Maria de Lourdes
Merighi TabaquimIV; Ana Paula Ribeiro RazeraV
I
Nurse. PhD. Professor. Craniofacial Anomalies Rehabilitation Hospital of
University of São Paulo. Bauru, São Paulo, Brazil. E-mail: armandotrettene@usp.br
II
Nurse. Graduated. University Paulista. Bauru, São Paulo, Brazil. E-mail: rosana_bonete@hotmail.com
III
Nurse. PhD. Craniofacial Anomalies Rehabilitation Hospital of University of
São Paulo. Bauru, São Paulo, Brazil. E-mail: priprado@usp.br
IV
Neuropsychologist. Professor. Bauru Dentistry College of University of São
Paulo. Bauru, São Paulo, Brazil. E-mail: malu.tabaquim@usp.br
V
Nurse. PhD. Lecturer at University Paulista and Faculdades Integradas de
Jaú. Bauru, São Paulo, Brazil. E-mail: anapaularazera@gmail.com
DOI: https://doi.org/10.12957/reuerj.2018.17523
ABSTRACT
Objective: to investigate the level of stress in nurses of an intensive care unit (ICU). Method: quantitative, descriptive study of a sample of 26 nurses in the ICU of a public hospital. The project was approved by the research ethics committee (Protocol E-016/10). Data were collected through two instruments: the Nursing Stress Inventory and a sociodemographic questionnaire. Statistical analysis included Student's t-test, Pearson's correlation and Variance Analysis, to a 5% significance level. Results: a significant association was observed between longer time working in the area and higher stress levels. Conclusion: the training time of less than ten years with a career that is still on the rise, linked to a context that allows stressful challenges, may have favored facilitatory and compensatory coping mechanisms with lower degrees of impact on the organism.
Descriptors: intensive care units; nursing; physiological stress; psychological stress.
INTRODUCTION
Work-related stress, also referred to as occupational stress, is a problem
to be considered nowadays, as the rates of temporary incapacitation,
absenteeism, early retirement, among others are alarming. However, the
stress and risk of health problems arise when the demands of the job do not
fit the worker's needs, expectations, or abilities.1
In the health area, professional stress is frequent, and, among
professionals, nurses are the most likely to develop a high level of
stress, which directly affects their job satisfaction and the quality of
care provided, including patient safety.2-5
Within the hospital context, intensive care units (ICUs) are environments
for the care of critically ill patients, who require permanent and
specialized medical and nursing care. They are characterized by demanding
routines and the need for fast and effective decision-making, as well as
high technology equipment, an environment with a lot of noise, most of the
time without natural light, and high possibility of death and pain, which
makes this environment naturally stressful.2,3
The work of ICU nurses has special characteristics due to the activities in
the direct assistance to patients and their families, as well as the
managerial and administrative activities, which include all the necessary
resources for the functioning of the unit. They are also responsible for
activities with a high degree of difficulty and responsibility, which
effectively contribute to the development of psychosocial factors that
condition the presence of stress at work, encompassing physical,
psychological and moral stress.6
Another important aspect related to the nurses' performance is the approach
to family members of the patients, who are usually at a high level of
anxiety and stress, especially when the family member's prognosis is
reserved. Authors have pointed out that family members of intensive care
patients are more likely to develop psychological symptoms, including
stress, anxiety and depression. Another factor considered as highly
stressful for nurses working in ICU is to mediate frequent conflicts
between professionals and family members about treatment plans.7
A humanization-based approach, especially in relation to reserved prognosis
of critical patients, is advocated for resulting in emotional support and
comfort to the family.8
In short, working at the ICU means investing intensively in the health care
of critical patients, with the help of differentiated technologies and
trained professionals who work as a team, in a suitable and specific
physical space. It is also associated with the difficulty to deal with
death, frequent in this sector.6
In this context, it is essential to identify the level of stress of nurses
working in the ICU. We believe that, through a situational diagnosis, it is
possible and feasible to propose interventions that minimize this
phenomenon, contributing to the quality of care, patient and professional
safety, worker health and cost reduction.
Thus, the objective of this study was to investigate the level of stress in
nurses working in an Intensive Care Unit (ICU).
THEORETICAL REFERENCE
Stress can be defined as a break in internal homeostasis, that is, the
stress reaction is elicited by a stressor that
consists of any event or situation in the environment that breaks internal
homeostasis, requiring an adaptation effort.9 In this way,
stress is a normal mechanism; If it is well understood and controlled it is
beneficial for a person because it causes the human being to react to
situations of risk. However, the lack of control and chronicity, cause
constant pressure to end in damage, both intellectually and physically. The
stimulus that could be beneficial is replaced by fatigue, which can lead to
the susceptibility of both physical and mental illness.10
Stress can be divided into three phases: alert phase (considered the
positive phase – the human being is energized through the production of
adrenaline, where survival is preserved and a sense of fullness is often
achieved), resistance phase (the person automatically tries to deal with
its stressors in order to maintain its internal homeostasis) and exhaustion
phase (when serious diseases can occur in the most vulnerable organs, such
as infarction, ulcers, depression, among others).9
However, one study has identified a four phases stress model called
near-exhaustion (when stressors persist in frequency or intensity,
resulting in a breakdown in the person's resistance), which is between the
stages of resistance and exhaustion.11
Stress as an intense reaction of the organism can arise when an individual
is confronted with situations that irritate, frighten, excite, confuse or
even those that make him immensely happy, due to the interpretation given
to the challenging event or due to inherently negative stressors. 12 Changes in people's lifestyles are leaving them debilitated
and thus vulnerable to stress, which has assumed the status of disease. In
Brazil, people are increasingly stressed, since the great majority do not
know how to deal with their sources of tension.13
Thus, it can be observed that studies about stress in the nursing team and
its correlation with work can help in the better understanding and possible
elucidation of some of the problems faced by nurses. Since these
professionals have different attributions and specific responsibilities,
depending on the field in which they operate, adding the internal and
external charges and having variable intensities.14
METHODOLOGY
This is a quantitative approach descriptive study carried out in the ICU of
a large public hospital, located in São Paulo state countryside. The sample
consisted of 26 nurses, both genders, in the age group from 31 to 50 years
old, who worked in the ICU, performing care and coordination activities.
Participants accounted for 93% of the workforce in the ICU.
The inclusion criterion was to work in the ICU in a period of more than six
months, because it was considered as adaptive and independent of performing
administrative or care functions. Nurses who were on vacation or on health
leave were excluded.
The ICU had 37 beds: 12 Adult ICU, 12 Pediatric ICU, 9 Coronary ICU and 4
Burned ICU. The nursing team, per unit, was composed of a coordinating
nurse, two nurse assistants in the morning, an attendance nurse in the
afternoon, even and odd evenings, as well as a professional covering the
days of each shift, nursing technician for every two beds per period.
Multidisciplinary care included nursing staff, physicians, nutritionists,
physiotherapists, social workers, speech therapists and psychologists.
Patients with clinical and/or surgical conditions, including neurological,
cardiovascular, pulmonary, metabolic, orthopedic, gastrointestinal and
renal dysfunction were attended.
Two instruments were used to collect the data: Nurses Stress Inventory
(IEE)15 and the Sociodemographic Questionnaire proposed for this
study. The IEE is composed of 44 questions that are inherent to the nurses'
work, scored in four levels, varying from never to always, categorized into
four domains (interpersonal relations, career stressors, intrinsic work
factors, organizational structure and culture). For the classification of
stress level, the following criteria were used: final score between 44 and
88 points - low stress, between 89 and 132 - intermediate stress, between
133 and 220 - high stress.
The socio-demographic questionnaire sought to identify the following
variables: gender, age, marital status, number of children, time in the
area, specialization course in the area, work shift, weekly workload and
number of employments, so that they are associated with the level of stress
later.
The data collection took place in October 2010, in a single moment, in the
counter shift of working hours, at a previously agreed place and time. For
the statistical analysis, T-Student Test, Pearson's Correlation and
Variance Analysis were used, all with a significance level of 5% (p≤0.05).
The research began after approval of the Research Ethics Committee
involving Human Beings16, by means of protocol E-016/10 on
09/08/2010. The participants formalized their adhesion with the signing of
the Informed Consent Form.
RESULTS AND DISCUSSION
To characterize the sample, from the 26 participating nurses, 4 (15.38%)
had administrative and managerial functions and 22 (84.62%) had
administrative and care functions. There was a prevalence of 24 (92%)
female nurses, 17 (65%) comprising between 20-30 years old, 13 (50%) were
married, 16 (62%) had no children, 23 (88%) had 1-10 years of graduation,
16 (62%) had 1-10 years of work time, 17 (65%) were specialists, 13 (50%)
worked in the morning shift, 16 (62%) worked 36 hours weekly and 16 (62%)
had a single employment agreement.
Regarding the IEE score according to domains, standard deviation and
confidence interval: 1-interpersonal relationships (average 29.4 points, SD
6.1), 2-career stressors (average 31.4 points, SD 7.5), 3-factors intrinsic
to work (average 30.5 points, SD 7, 3) and 4-structure and organizational
culture (average 32 points, SD 7.4), organizational structure and culture
domain prevailed as shown in Figure 1.
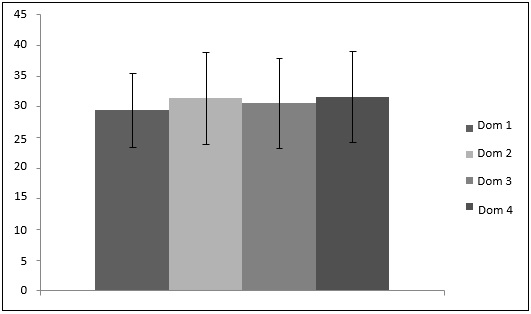
FIGURE 1:
Distribution of the participants according to the score of the Nurses
Stress Inventory, according to the domains: 1-interpersonal relationships,
2-career stressors roles, 3-factors intrinsic to work and 4-organizational
structure and culture, and the confidence interval. Bauru, 2010.
Statistical significance (p=0.017), were associated with the
sociodemographic variables in the stress domains, noting that the longer
the activity time in the area (>5 years), the higher the level of
stress. In the other variables there was no significant correlation.
Regarding the classification of the participants on the level of stress,
the intermediate group had the highest number of participants (16), with a
percentage of 62% of the sample (Figure 2). It was considered
representative that 35% (n=9) of the participants showed a high stress
level and only 3% (1 participant) with a low rating.
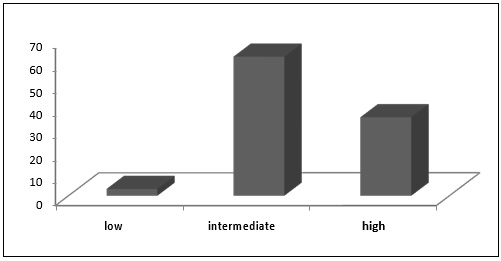
FIGURE 2:
General percentages of participants according to stress levels: low,
intermediate and high, according to the Nurses Stress Inventory. Bauru,
2010.
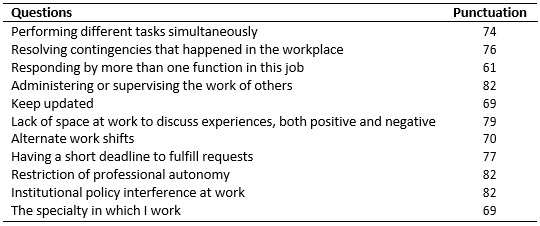
To identify the prevalent situations in relation to the categorization of
stress, Table 1 presents the distribution of participants' responses in
relation to the structure and organizational culture domain,
evidenced as a more intermediate stressor. There was a higher score in the
activities "administering or supervising the work of other people",
"restriction of professional autonomy" and "interference of institutional
policy in the workplace", each with 82 points. The less-punctuated
activities were related to "responding to more than one function in this
job" (61), "keeping up to date" (69) and "the specialty in which I work"
(69).
TABLE 1: Distribution of the participants' responses, according to the
questions belonging to the domain: structure and organizational culture.
Bauru, 2010.
Regarding the sociodemographic characterization, the predominance of the
female gender was observed. Nursing, from its earliest stages, is exercised
mainly by women, although a recent progression of the masculine gender in
the profession has been observed recently. The woman, by exercising
multiple activities besides her job, like domestic activities and the care
with the children, it can be inferred that the level of stress could be
greater in this gender; however, this relationship was not observed in the
present study, a result consistent with the literature, in which there is
no difference in genders regarding stressors.17
In relation to the age group, it was predominant that it comprises between
20 and 30 years old, that is, the nurses working in the ICU were young.
This profile of nurses is indicated as ideal for the ICU due to the
openness and ease of technology, as well as the motivation to aid critical
patients, aiming at professional growth. Nurses over 40 years old, due to
their professional experience, usually hold administrative positions or
teaching-related activities.17 In the present study there was no
association between age and stress level, corroborating another study. 18
Regarding the marital status, it was observed a predominance of married
people, which did not influence on the level of stress. On the other hand,
another study showed that most of the nurses were single, and the level of
stress was higher between divorced and married people.18
Most participants reported that they did not have children. It is
understood that the greater the number of children, the greater the
responsibilities and consequently the greater the stress; however, this
relationship was not observed in the present study.
Regarding training time, those trained between 1 and 10 years prevailed,
and this result did not influence the level of stress. However, one study
evidenced stress in most nursing students, and one third of them are in the
phase of exhaustion, given that this is the most worrying phase, in which
there is a higher propensity to become ill.19 Systematic
training programs for nurses newly admitted to intensive care have been
developed with positive results, and this practice is recommended for
patient safety and reduction of stresses.20
As for the time of ICU performance, more than five years predominated, and
this result influenced the level of stress, i.e., the higher the
professional experience, the higher the stress level, corroborating with
the literature.17 This result was associated to the nurse's
exposure to stressful situations, commonly experienced in ICUs, including:
overload of work, turnover, overcrowding, inadequate physical space, direct
and indirect assistance to severely ill patients with imminent death,
excessive levels of noise, unpreparedness and professional dissatisfaction,
among others.6-8
On the other hand, another study observed that the longer the performance
time, the lower the stress level, relating the result to the acquired
professional experience.18 A study carried out with senior
nurses who began their activities in ICU concluded that they presented
satisfactory adaptation, with capacity to cope well with the inherent
complexity of the unit, associating this result to the stages as students
in this area.21
When questioned about having a course of specialization in ICU, most of the
participants reported having it, but this variable did not influence the
level of stress, corroborating with the literature.18 In order
to act in the ICU, it is necessary to have a significant theoretical and
practical knowledge, due to the complexity of the patients, the
technologies required for care, as well as fast and effective decision
making, which explains the nurses' demand for specialization courses.
In relation to the work shift, morning and night were predominant. Although
the night period is indicated as the most influential work shift on the
level of stress due to sleep deprivation, the results of the present study
did not indicate its influence on stress. However, night work
and shifts in relation to the work shift have been reported as interfering
directly in the functioning of the body, causing headache, irritability,
sleep disturbances and stress.22
Regarding the workload, the majority reported working 36 hours a week and
this variable did not influence the level of stress. It is worth mentioning
that in the ICU where the present study was carried out, the care nurses
had a weekly workload of 36 hours, while the administrative staff had a
workload of 40 hours a week. The prevalence of care nurses may justify this
result. Long working hours are pointed out as an important factor in the
development of stress and burnout, and can be detrimental to family time,
rest and leisure.23
In relation to the number of employment agreements, the majority reported
having a single agreement; however, this result did not influence the level
of stress. It is assumed that nurses who have multiple employment
relationships, with all the inherent responsibilities, are more likely to
develop stress.
When assessing the level of stress of nurses working in the ICU, the
prevalence of the intermediate stress level linked to the structure and
organizational culture domain was observed, implying situations related to
the administration or supervision of the work of others, restriction of
professional autonomy and interference institutional policy at work. These
data corroborate with the findings in the literature.6,24
Coping with criticism, crises among managers, subordinates and colleagues,
difficulties in decision making, discrepancies between tasks, lack of
professional recognition, and difficulties related to patient and family
care are pointed out as more stressful factors.18 The psychic
charges are related to the object of human work, which demands situations
generating stress, suffering, fatigue, tension, and to the forms of
organization of this work, marked by routine, lack of autonomy and by forms
of supervision and control.24 Communication difficulties,
inappropriate working conditions and unworthy remuneration are
destabilizing factors of the interprofessional relationship.
Nurses recognize the difficulties in relation to the leadership and
organization of work, especially when reflecting on how the team relates
and articulates with the demands. The condition of articulating the
individual, relational and organizational dimensions necessary for the
exercise of leadership makes its practice complex, which clarifies the
difficulty faced in the nursing work routine.26
It is worthy highlighting that the working conditions related to the
stressors of the profession, aspects of the organization and administration
of ICU, supervision of team work and professional autonomy are inherent
functions of the nurse. Studies indicate that responsibilities of this type
can be one of the main causes of occupational stress among nurses, because
they lead to lack and/or failure in communication, which make decisions
difficult and compromise care, generating more suffering than pleasure at
work.4,27
A study carried out with the objective of identifying the factors
influencing nurses working in pediatric ICU to leave their jobs concluded
that the main reason was the work stress, influenced by the nature of the
work, the lack of resources and the lack of recognition by the managers.28
It is important to note that although many researches on stress in nurses
have been developed in recent times, there is a shortage of proposals and
interventions that seek to minimize or facilitate the coping of stressors,
since they are inherent to work and to the critical units.
The study allowed to identify, therefore, the necessity of carrying out
multicentric studies, which allow to increase the sampling, as well as
researches that allow comparing the level of stress of nurses, according to
the profile of patients attended. Studies that propose interventions on
occupational stress have been little contemplated in the literature and it
is pertinent as a necessary contribution to the advancement of science in
this challenging theme.
CONCLUSION
The nurses working in the ICU presented an intermediate level of stress,
related to the difficulties regarding supervision, professional autonomy
and influence of institutional policy. The training time of less than ten
years, with a career still on the rise, coupled with a context that allows
challenges considered as stressful, may have favored facilitating coping
mechanisms, with lower degrees of impact on the body.
Although the present study contemplated almost the entire ICU population
participating, the sample size of nurses in intensive care units may be
referred to as a limitation. Another limiting factor is the fact that the
sample includes nurses working in pediatrics, which may have influenced the
result in some way, believing that these professionals are exposed to a
greater number of stressors.
REFERENCES
1.Isfort M. Influence of personnel staffing on patient care and nursing in
German intensive care units. Descriptive study on aspects of patient safety
and stress indicators of nursing. Med Klin Intensivmed
Notfmed. 2013; 108(1):71-7.
2.Martins MGT, Castro O, Pereira PPG. Body, stress and nursing: ethnography
of na Intensive Care and Surgical Center. Estud Psicol (Campinas). 2013;
30(4):525-37.
3.Mehrabi T, Azadi F, Pahlavanzadeh S, Meghdadi N. The effect of yoga on
coping strategies among intensive care unit nurses. Iran J Nurs Midwifery
Res. 2012; 17(6):421-4.
4.Versa GL, Murassaki AC, Inoue KC, Melo WA, Faller JW, Matsuda LM.
Occupational stress: evaluation of intensive care nurses who work at
nighttime. Rev Gaúch Enferm.
2012; 33(2):78-85.
5.Belancieri MF, Beluci ML, Silva DVR, Gasparelo EA. A resiliência em
trabalhadores de enfermagem. Estud Psicol (Campinas). 2010; 27(2):227-33.
6.Ganz FD. Tend and befriend in the intensive care unit. Crit Care Nurse.
2012; 32(3):25-33.
7.McAdam JL, Fontaine DK, White DB, Dracup KA, Puntillo KA. Psychological
symptoms of family members of high-risk intensive care unit patients. Am J
Crit Care. 2012; 21(6):386-93.
8.Gutierrez KM. Experiences and needs of families regarding prognostic
communication in an intensive care unit: supporting families at the end of
life. Crit Care Nurs Q. 2012; 35(3):299-313.
9.Seyle H. The stress of life. New York: Longman, 1956. Apud: Del Bianco
Faria AM, Cardoso CL.Psychosocial aspects of caregivers of children with
câncer: stress and coping. Estud Psicol (Campinas). 2010; 27(1):13-20.
10.Tabaquim MLM, Marquesini MAM. Study of the stress of parentes of
patients with cleft lip and palate in a surgical process. Estud Psicol
(Campinas). 2013; 30(4):517-24.
11.Lipp MEN. Inventário de sintomas de stress para adultos de Lipp (ISSL).
3a ed. São Paulo: Casa do Psicólogo; 2005.
12.Lipp MEN. O modelo quadrifásico do stress. In: Lipp MEN, organizadora.
Mecanismos neuropsicofisiológicos do stress: teoria e aplicações clínicas.
São Paulo: Casa do Psicólogo; 2003. p. 17-21.
13.Lipp MEN, Malagris LEN, Novais LE. Stress ao longo da vida. São Paulo:
Ícone; 2007.
14.Kestenberg CCF, Felipe CV, Rossone FO, Delphim LM, Teotonio MC. O
estresse do trabalhador de enfermagem: estudo em diferentes unidades de um
hospital universitário. Rev Enferm UERJ. 2015; 23(1):45-51.
15.Stacciarini JMR, Tróccoli BT. Instrumento para mensurar o estresse
ocupacional: Inventário de Estresse em Enfermeiros (IEE). Rev Latino-Am
Enferm. 2000; 8(6):40-9.
16.Ministério da Saúde (Br). Conselho Nacional de Saúde. Resolução Nº 466,
de 12 de dezembro de 2012: diretrizes e normas reguladoras de pesquisas
envolvendo seres humanos. Brasília: Ministério da Saúde; 2013.
17.Trettene AS, Ferreira JAF, Mutro MEG, Tabaquim MLM, Razera APR. Estresse
em profissionais de enfermagem atuantes em Unidades de Pronto Atendimento.
Bol Acad Paul Psicol. 2016; 36(91):243-61.
18.Rodrigues VM, Ferreira AS. Stressors in nurses working in intensive care
units. Rev Latino-Am Enferm. 2011; 19(4):1025-32.
19.Kestenberg CCF, Rosa BMS, Silva AV, Fabri JMG, Regazi ICR. Stress in
undergraduate nursing students. Rev Enferm UERJ. 2017; 25:e26716.
20.Alonso-Ovies Á, Álvarez-Rodríguez J, del Mar García-Gálvez M,
Velayos-Amo C, Balugo-Huertas S, Álvarez-Morales A. Usefulness of failure
mode and effects analysis to improve patient safety during the process of
incorporating new nurses in an intensive care unit. Med Clin (Barc). 2010;
135(1):45-53.
21.O'Kane CE. Newly qualified nurses experiences in the intensive care
unit. Nurs Crit Care. 2012; 17(1):44-51.
22.Costa AS, Griep RH, Fischer FM, Rotemerg L. Need for recovery from work
and sleep-related complaints among nursing professionals. Work. 2012;
41(1):3726-31.
23.Silva AA, Rotenberg L, Fischer FM. Nursing work hours: individual needs
versus working conditions. Rev Saude Publica. 2011; 45(6):1117-26.
24.Van Dam K, Meewis M, Van der Heijden BI. Securing intensive care:
towards a better understanding of intensive care nurses' perceived work
pressure and turnover intention. J Adv Nurs.
2013; 69(1):31-40.
25.Silva SM, Baptista PCP, Felli VEA, Martins AC, Sarquis LMM, Mininel VA.
Intervention strategies for the health of university hospital nursing staff
in Brazil. Rev Latino-Am Enferm. 2013; 21(1):300-08.
26.Costa DG, Dall'Agnol CM. Participative leadership in the management
process of nightshift nursing. Rev Latino-Am Enferm. 2011; 19(6):1306-13.
27.Kestenberg CCF, Felipe ICV, Rossone FO, Delphim LM, Teotonio MC. The
stress of nursing workers: study in diferente units of a university
hospital. Rev Enferm UERJ. 2015; 23(1):45-51.
28.Foglia DC, Grassley JS, Zeigler VL. Factors that influence pediatric
intensive care unit nurses to leave their jobs. Crit Care Nurs Q. 2010;
33(4):302-16.