(*) Pearson's Qui-square
(**) Kruskal Wallis test
Source: External Evaluation Database/Program for Improving Access and Quality, 2012.
ORIGINAL RESEARCH
Tuberculosis in Brazil: the relationship between population size, structure and process
Ardigleusa Alves CoêlhoI; Marize Barros de SouzaII; Nilma Dias Leão CostaIII; Grasiela PiuvezamIV; Ricardo Alexandre ArcêncioV; Severina Alice da Costa UchôaVI
I
Nurse. PhD. Professor, Department of Nursing, State University of Paraíba.
Paraíba, Brazil. E-mail: ardigleusacoelho@gmail.com
II
Nurse. PhD. Professor, Federal University of Rio Grande do Norte. Natal,
Rio Grande do Norte, Brazil. E-mail: marizebs@gmail.com
III
Mathematician. PhD. Adjunct Professor, Federal University of Rio Grande do
Norte. Natal, Rio Grande do Norte, Brazil. E-mail: nilmadlcosta54@gmail.com
III
Odontologist. PhD. Adjunct Professor, Federal University of Rio Grande do
Norte. Natal, Rio Grande do Norte, Brazil. E-mail: gpiuvezam@gmail.com
V
Nurse. PhD. Professor, University of São Paulo. Ribeirão Preto, São Paulo,
Brazil. E-mail: ricardoarcencio@uol.com.br
VI
Physician. PhD. Associate Professor, Federal University of Rio Grande do
Norte. Natal, Rio Grande do Norte, Brazil. E-mail:
alicedacostauchoa@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.17284
ABSTRACT
Objective: to evaluate the relationship between population size and characteristics of structure and care process of primary attention to tuberculosis in Brazil. Methods: cross-sectional study. A total of 12656 professionals from family health strategy teams were analysed, measured by External Evaluation of the Program for Access and Quality Improvement in Primary Care, where there were cases of tuberculosis. Data analysis was performed using chi-square and Kruskal Wallis tests to verify association between variables and municipality sizes. Research was approved by Ethics in Research Committee - Protocol #21904. Results: significant difference between access, coordination of care, technical quality of attention to tuberculosis and municipality size was observed (p <0.001). Conclusion: characteristics of structure and care process in control of tuberculosis are related to municipal population size.
Keywords: Tuberculosis, primary health care, family health strategy, health services evaluation.
INTRODUCTION
Worldwide, tuberculosis (TB) is still one of the serious public health problems, with approximately 9 million new cases and 1.5 million deaths in 2013. Globally, TB mortality rate has declined by 45% since 1990, with decreasing rates of TB incidence in most of the world1. In the world scenario, Brazil is one of the 22 countries that concentrate 80% of TB cases in the world1. This country had an incidence of 35.4 cases per 100,000 inhabitants in 2013. As for mortality, the mortality rate has halved when compared to the 1990 coefficients, of 2.3 deaths per 100,000 inhabitants, thus reaching the goals set for this millennium2.
Tuberculosis control is a priority for the Brazilian government. Since 2006, the Ministry of Health has intensified the decentralization of diagnosis and treatment to the Family Health Strategy (FHS) in order to increase access to early diagnosis and treatment3. The FHS is the main strategy of primary health care (PHC) in Brazil, because it provides a change in the work process based on the principles of universality, accessibility and coordination of care, bonding and continuity, comprehensiveness, accountability, humanization, equity and social participation4.
The implementation of the FHS provided the expansion of the provision of PHC; however, the decentralization of TB control to the FHS have not guaranteed satisfactory access to the early diagnosis in PHC services 5,6. At present, the diversity of local health systems, regional disparities and inequalities in access to health services have caused an impact on the timely diagnosis of TB and imposed challenges for the achievement of evaluative processes7 focused on the performance of health services. Aspects related to the structure and work process of the teams may be influencing the organization of TB care and it is assumed that these aspects are related to the population size of the municipalities.
Among the current initiatives of the Brazilian Ministry of Health to assess aspects of the quality of PHC, including TB care, the Program for Improving Access and Quality of Primary Care (PMAQ-AB in Portuguese) stands out 8. The present study has as reference the external evaluation component of the PMAQ-AB that conceives health quality from the triad structure, process and results9. This structure was emphasized because we recognize its importance for the organization and adequacy of health work and the process from the perspective of the production of care in order to improve quality. Thus, the objective of this study was to evaluate the relationship between the population size of the municipalities and the characteristics of TB structure and patient care process in primary care in Brazil.
LITERATURE REVIEW
At present, the establishment of health quality standards is still a major challenge. The meaning of quality in health care depends on the accumulation of scientific knowledge, individual expectations and social values in each historical moment10. Health quality is defined as the degree to which health services meet patients' needs, expectations and standard of care9. In another conception, quality consists of the degree to which services increase the likelihood of desirable outcomes for individuals and populations, being consistent with current professional knowledge11. In both definitions, health quality encompasses a variety of terms, which measure quality only in its quantitative aspects, without regard to its subjective dimension10.
Typically, health quality assessment is based on the systemic model12 and dimensions or attributes that define quality (the seven pillars of quality)13. The systemic model seeks to verify the relationship between structure, processes and results. This model has been extremely useful for assessing the quality of health services around the world. Structure comprises the resources and inputs, as well as the organization thereof to carry out the activities. Process, however, refers to activities: the way work is organized to produce care. Result is the action of the product on people's health, and the impact of these activities on individuals or in the community can be measured. The attributes that define the quality of the activities developed in health services are efficacy, effectiveness, efficiency, acceptability, equity, adequacy and scientific-technical quality13.
In this sense, in Brazil, the search for evidence of effectiveness, quality and equity and the establishment of a quality-focused assessment culture triggered evaluation processes in the context of PHC. In the 1990s, the process of evaluation and monitoring of primary care was carried out to investigate the epidemiological pattern, performance and quality of primary care in Brazilian cities with more than 100 thousand inhabitants14. Most recently, the Program for Improving Access and Quality of Primary Care was instituted8.
The purpose of PMAQ-AB is to increase access and qualification of management, care and participation practices in PHC through evaluative cycles, consisting of four phases: adherence and contracting; development, external evaluation and re-contracting. Its guidelines include a continuous and progressive process of improving standards and indicators of access and quality involving the management, the work process and the results achieved by the primary care health teams8. Several aspects of the work process of these teams are evaluated by the PMAQ-AB, including the prevention and treatment of diseases, such as tuberculosis, as a way to increase the capacity of response of the three spheres of management of the Unified Health System (SUS) to surveillance and control of morbidities2.
METHODOLOGY
This is a cross-sectional study with a quantitative approach. The study uses data extracted from the database of the external evaluation phase of PMAQ-AB8, held in Brazil in 2012. The SUS, in 2012, had 33,404 FHSs covering 5,297 Brazilian municipalities15. Adherence to the PMAQ-AB was of 17,202 teams (51% of the teams deployed in the country) and 14,111 Basic Units in 3,944 (70.8%) municipalities in the country.
The study population consisted of 17,202 higher education professionals (993 physicians, 15,876 nurses and 993 dentists). The universe analyzed in this study corresponds to a sample of 12,656 professionals (818 physicians, 11,585 nurses and 253 dentists) by the exclusion of teams where there was no record of TB care.
The variables to evaluate the structure and process of care of TB patients in the municipalities were selected from the questionnaire (Module II) - Interview with the primary care team practitioner and verification of documents in the basic health unit of the external evaluation of the PMAQ-AB. The structured questionnaire, in electronic format, available on tablet was applied by interviewers trained on the theme and methodology. The validation of the interviews was carried out through the software PMAQ-AB online validator16, based on the criteria defined in the protocol for analysis of consistency and validation of data collected 17.
For the analysis of the data, we included variables of seven dimensions of the questionnaire, which were grouped into categories to characterize the structure (access and coordination of care) and the process of TB patient care (technical quality). With regard to access, the variables selected were: implantation of the welcoming in the health unit; welcoming the spontaneous demand; waiting time for listening/welcoming; reservation of vacancies; user's waiting time for receiving care by the primary care team; waiting time for the previously scheduled appointment at the health facility; scheduling of consultations and actions by the team for users to be part of the program and priority groups.
The variables identified for analysis of care coordination were: existence of a protocol with definition of therapeutic guidelines for TB; smear request; frequency of contact between primary and specialist care professionals and frequency of contact between specialists and primary care professionals about referred patients; number of referrals for consultation in pulmonology; estimated waiting time of patients referred to the consultation in pulmonology.
The technical quality was evaluated based on the following variables: monitoring of directly observed treatment (DOT); active search of missing patients from the DOT; existence of case report forms, provision of educational and health promotion actions directed to TB; active search for respiratory symptomatic individuals during the home visit by the community health worker (CHW).
The municipalities of the PHC teams were grouped into four population strata, namely: small municipality (population up to 50,000 inhabitants); medium-size municipality (population between 50,001 and 100,000 inhabitants); large municipality (population between 100,001 and 900,000 inhabitants); and the municipality with more than 900,000 thousand was considered a metropolis18. The categories of structure and process were classified as dependent variables and the population stratum of the municipalities constitute the independent variable.
Descriptive analysis of the characteristics of access, coordination of care and technical quality by population stratum of the municipalities, mean and standard deviation (SD) of the waiting time for care and/or consultation were carried out. With regard to structure, this dimension was measured through access and coordination of care. The dimension process of care for clients with TB was measured through technical quality. To do so, the variables characterizing each aspect of structure and process were divided in yes or no, followed by the sum of the answers of each item, divided by the total of the sample. The chi-square analysis aimed to verify the differences of the strata of the municipalities by population size and the characteristics of structure and process. The Kruskal Wallis test was applied to verify the differences in mean waiting time for listening/welcoming, provision of care by the team and referral of users for consultation in pulmonology by municipal stratum.
The multicentric research project was approved by the Research Ethics Committee of the Federal University of Rio Grande do Sul under number 21904 on March 13, 2012, in accordance with Resolution No. 196/96 of the National Health Council.
RESULTS AND DISCUSSION
Among the professionals that participated in the study, 6,010 (47%) worked in small municipalities, 1,340 (11%) in medium-sized municipalities, 2,997 (24%) in large municipalities and 2,309 (18%) in metropolises.
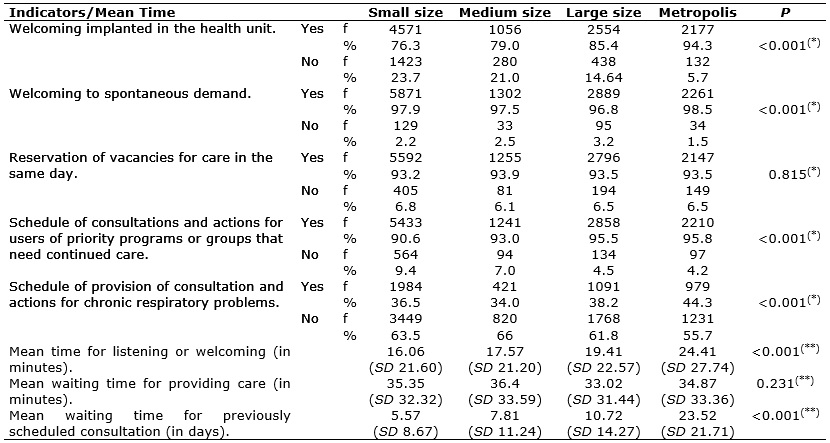
Regarding the characteristics of user access to the health unit, there is a significant difference between the municipalities (p <0.001), especially the metropolises, which present the majority – 2,177 (94.3%) - of PHC teams with implementation of the welcoming strategy; followed by 2,261 (98.5%) with welcoming of spontaneous demand; 2,210 (95.8%), with scheduling of consultations and actions for users of priority programs or groups; 979 (44.3%) with offer of consultations for chronic respiratory problems, as shown in Table 1.
TABLE 1:
Characterization of access to primary health care by population size.
Brazil, 2012
(*)
Pearson's Qui-square
(**)
Kruskal Wallis test
Source: External Evaluation Database/Program for Improving Access and
Quality, 2012.
The analysis of aspects related to access to the health unit reveals changes in the work process of these teams. In the organization of the user access to the service network, the teams have adopted strategies that allow the functional adaptation of the health units to meet the health needs of users, such as welcoming; the possibility of attending to non-scheduled consultations; and scheduling of consultations for priority groups. Welcoming is indicated as the main strategy for the organization of the entrance door in the health units, for articulation between spontaneous and programmed demand19, however, it presents a limitation due to the difficulties of access to the service and the way services are organized20.
Regarding the mean waiting time of users in the health unit, there was a significant difference (p <0.001). Metropolises had the longest mean waiting time, equivalent to 24.41 minutes. Regarding the waiting time for provision of care, the highest mean time was observed in medium-sized municipalities (36.4 minutes), however, there was no significant difference between the strata by population size (p <0.31), according to Table 1.
Regarding the waiting time for previously scheduled consultation, a statistically significant difference was observed between the municipalities (p <0.001). The smallest and largest mean time, in minutes, were verified in small (5.75) and large municipalities (23.52) respectively, which can be visualized in Table 1.
The findings of our study on the user's waiting time of receiving care corroborate the results of a study conducted in Belo Horizonte, where health units, in most cases, serve the user within 2 hours21. In relation to users with TB, there is controversy about the waiting time for consultation, in the user's view. In a study conducted in Itaboraí/RJ, 63% answered that it 'never' takes more than 60 minutes22, but another study shows that although most patients have no difficulty in getting consultations within 24 hours, they do not manage to receive care within 60 minutes4.
In terms of coordination of care, 9,544 (76.3%) professionals interviewed reported the existence of a protocol with therapeutic guidelines for TB in the health unit. There was a statistically significant association between the existence of the protocol and the size of the municipality (p <0.001), according to Table 2.
TABLE 2: Characterization of care coordination for tuberculosis in primary care by
population size. Brazil, 2012 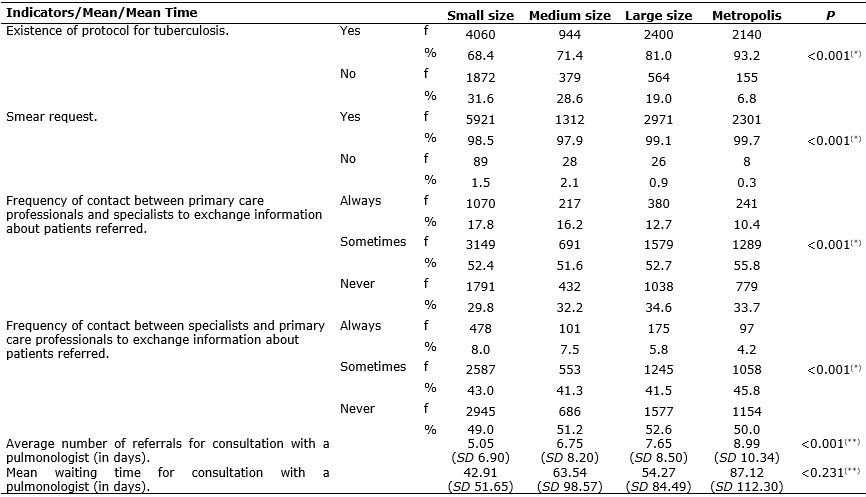
(*)
Pearson's Qui-square
(**)
Kruskal Wallis test
Source: External Evaluation Database/Program for Improving Access and
Quality, 2012.
Clinical protocols are a crucial tool in the work process of health teams by minimizing inadequacies in clinical practice23 and its implementation can facilitate the integration of primary care teams with the care network24. A study carried out in Madrid/Spain showed that one of the limitations of the role of nurses in the TB program was the lack of protocol25.
The request for smear test by the teams was reported by 12,505 (98.8%) of the interviewees, regardless of the population size. A significant difference was observed between the population size of the municipalities in relation to the semar request (p <0.001). The highest frequency of smear request was observed in municipalities classified as metropolises - 2301 (99.7%). Sputum smear is still the main method used for case detection and also for treatment control3.
As for the frequency of contact between PHC professionals and specialists to exchange information about referred patients, 6,708 (53.3%) professionals reported that they sometimes performed these contacts, with the highest frequency observed in PHC teams in metropolitan areas – 1,289 (55.8%). However, 6,362 (50.3%) reported that specialists never contact PHC professionals to treat patients referred to that level of health care. The highest proportion was verified in teams of large municipalities - 1577 (52.6%).
Regarding the referrals of users for consultation in pulmonology by the PHC teams, there is a growing trend in the number of referrals as the population size increases, with a significant difference for the metropolises (p <0.001). These results show that the exchange of information between PHC teams and specialized services is still incipient. Specifically in relation to TB care, a study refers to the discontinuity of information flow in referral and counter-referral processes of patients 26.
Another aspect that deserves attention is the reduced flow of referrals to specialized consultation in pulmonology. The smallest and largest mean waiting time, in days, for consultation with a pulmonologist, was observed among teams of small municipalities (42.91) and in metropolises (87.12), respectively. There was statistical significance between the mean waiting times for consultation and the population size of the municipality (p <0.001), as shown in Table 2.
One of the explanations for this finding may be the fact that, in some Brazilian municipalities, the reference units of the Tuberculosis Control Program are still the main entry points for access to TB diagnosis 7 and for monthly follow-up medical consultations22.
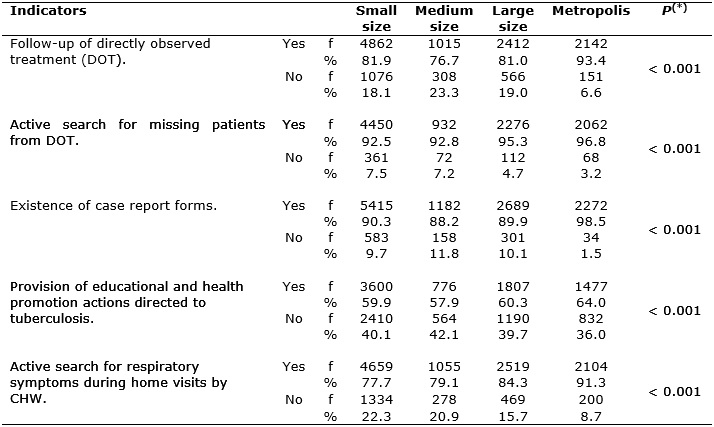
Statistical significance was found in all variables that characterize the technical quality of primary care for TB according to the population size (p <0.001), as shown in Table 3.
TABLE 3:
Characterization of the technical quality of the actions to control
tuberculosis in primary care by population size of the municipalities.
Brazil, 2012.
(*)
Pearson's Qui-square
Source: External Evaluation Database/Program for Improving Access and
Quality, 2012.
Municipalities classified as metropolises present better performance in technical quality, with a higher proportion of follow-up of directly observed treatment (DOT) – 2,142 (93.4%); active search of missing patients to the DOT – 2,062 (96.8%); the existence of TB case report forms by primary care teams – 2,272 (98.5%) and the offer of educational actions directed at TB 1,477 - (64.0%); active search for respiratory symptomatic (RS) patients in the territory of the team by the CHW, - 2,104 (91.3%).
The technical quality of care for TB patients, as a process indicator, shows that decentralization of the actions of diagnosis and treatment of this disease to PHC is a reality in the studied context and that there is a difference in this quality when considering the population size of the municipality. It was verified that the PHC teams have been carrying out actions recommended by the National Tuberculosis Control Program 3.
The DOT is a key element in strengthening patient adherence to treatment and reducing the risk of drug resistance3. There was a high percentage of monitoring of DOT in all PHC teams, regardless of population size. A study carried out in Teresina/Piauí showed that 67.1% professionals of the FHS always referred to follow the DOT26. The follow-up of the DOT by the PHC teams is relevant for minimizing the transmission of the disease and providing changes in TB control in Brazil27.
The active pursuit of missing patients to the DOT has been incorporated into the work process of the evaluated teams. A similar result was found in another study, in which 68.9% of the teams reported developing this activity28. The search of the missing patients is one of the attributions of the Brazilian PHC teams to avoid the abandonment of TB treatment3.
The epidemiological surveillance of TB aims to know the magnitude of the disease to subsidize control actions. Thus, it is the compulsory responsibility of the health units to report the occurrence of new cases, which can be performed by any professional in the team, mainly by filling out the notification form of the National Disease Notification System (SINAN)3. However, for the case report, it is necessary that the form is available at the health unit, as reported by the majority of professionals interviewed, especially in cities classified as metropolises, but the existence of notification forms alone does not guarantee that all cases are notified. Underreporting of cases is one of the main obstacles to the knowledge of the epidemiological status of TB. A study carried out in the Arsi/Ethiopia Zone showed that underreporting of the disease cases was observed in 25 neighborhoods, despite the increase in the notification of cases after the introduction and expansion of the DOT29.
Regarding the active search for respiratory symptomatic (RS) individuals during the home visit performed by CHWs, it is observed that this activity is more effective in the metropolises (91.3%, p <0.001) according to Table 3. Despite the high prevalence of this activity among the teams evaluated, a study carried out in São Paulo found that active search for RS individuals by CHWs still occurs sporadically in PHC30.
Health education is an essential tool to promote care for people with TB, especially in combating stigma31 and, in the studied context, there was a better performance by the metropolises in the provision of educational and health promotion activities directed to tuberculosis. It is important to highlight the importance of the involvement of the person with TB in educative practives32.
CONCLUSION
The present study has broadened the knowledge of the structure and the process of care of the PHC teams in TB control. Access, coordination of care and technical quality of TB care are associated with the size of the municipality. Municipalities classified as metropolises presented better performance in the organization of care.
The analysis of the characteristics of the user access to the health unit points to an organization of the work process by the teams focusing on their technical dimension. Comprehensiveness of care is sought by the adoption of strategies that favor the bonding and the accountability among users and health teams. Access has been facilitated by the welcoming; however, in the coordination of care fragilities persist.
Regarding the process, despite having an organization standardized by the Ministry of Health, the technical quality has weaknesses in educational activities and active search. TB care has made advances, but there are still challenges that need to be overcome. Technical quality should be reinforced to increase the coverage of DOT follow-up, active search for symptomatic respiratory individuals and educational actions.
Further studies are necessary to better understand the differences found in the structure and process of care for users with TB, considering the population size of the municipalities. However, it should be noted that, despite the association between population size and structure and process characteristics, other factors interfere in the organization of the service and in the occurrence of TB.
REFERENCES
1.World Health Organization. Global tuberculosis report 2014 [Internet]. Geneva; 2014. [cited in 2016 Nov 20]. Available from:
http://apps.who.int/iris/bitstream/10665/137094/1/9789241564809_eng.pdf
2. Ministry of Health (Br). Department of Health Surveillance. Control of tuberculosis in Brazil: advances, innovations and challenges. Epidemiological Bulletin [online] 2014; 45 (2): 1-13. [cited in Nov 23 2016]. Available from: http://portalsaude.saude.gov.br/images/pdf/2014/maio/29/BE-2014-45--2--tb.pdf
3. Ministry of Health (Br). Department of Health Surveillance. Manual of Recommendations for the Control of Tuberculosis in Brazil. National Tuberculosis Control Program. Brasília (DF Ministry of Health; 2011.
4.Ministry of Health (Br). Department of Health Care. National Policy of Primary Care. Brasília (DF), Ministry of Health; 2012 [cited in June 04. 2016]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/politica_nacional_atencao_basica.pdf
5.Scatena LM, Villa TCS, Ruffino-Netto A, Kritski AL, Figueiredo TMRM, Vendramini SHF et al. Difficulties in accessing health services for the diagnosis of tuberculosis in Brazilian municipalities . Rev. saúde pública (Online). 2009 [cited in May 06 2016]. 43(3): 389-97.
Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-89102009000300001&lng=en . Epub Apr 10, 2009.
6.Marcolino ABL, Nogueira JA, Ruffino-Netto A, Moraes RM, Sá LD, Villa TCS et al. Evaluation of access to tuberculosis control actions in the context of the family health teams of Bayeux – PB. Rev. bras. epidemiol. [Scielo-Scientific Electronic Library Online] 2009 [cited in May 06 2016]; 12(2): 144-57. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1415-790X2009000200005&lng=en
7.Villa TCS, Ponce MAZ, Wysocki AD, Andrade RLP, Arakawa T, Scatolin BE et al. Timely diagnosis of tuberculosis in health services in several regions of Brazil. Rev. latinoam. enferm. (Online). 2013 [cited in: May 06 2016]. 21(spe): 190-8. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-11692013000700024&lng=en
8.Ministry of Health (Br). Ordinance No. 1,654 of July 19, 2011. It establishes, within the scope of the Unified Health System, the Program for Improving Access and Quality of Primary Care (PMAQ-AB) and the financial incentive of PMAQ-AB, known as the quality component of variable primary care ceiling - variable PAB. Brasília (DF): 2011 [cited in June 04. 2016]. Available from: http://bvsms.saude.gov.br/bvs/saudelegis/gm/2011/prt1654_19_07_2011.html
9.Donabedian A. Quality of care: definition and evaluation methods. México: La Prensa Médica Mexicana; 1984.
10.Frias PG, Costa JMBS, Figueiró AC, Mendes MSM, Vidal AS. Attributes of health quality. In: Samico I, Felisberto E, Figueiró AC, Frias PG, organizations. Health assessment - conceptual and operational bases. Rio de Janeiro: MedBook; 2010 p. 43-55.
11.Lohr KN, Schroeder SA. A strategy for quality assurance in medic care.
N. Engl. j. med. [online] 1990 [cited in June 2016 04]; 322:707-12. Available from: http://www.nejm.org/doi/full/10.1056/NEJM199003083221031
12.Donabedian A. The seven pillars of quality. Arch. pathol. lab. med. [National Center for Biotechnology Information Online] 1990 [cited in June 2016 04]; 114(11):1115-8. http://www.ncbi.nlm.nih.gov/pubmed/2241519
13. Donabedian. A . The quality of care. How can it be assessed? JAMA. [National Center for Biotechnology Information Online] 1988 [cited in 2016 June 04]. 23-30; 260(12): 1743-8. Aveilable from: http://www.ncbi.nlm.nih.gov/pubmed/3045356
14.Bodstein R. Decision-making process and health assessment: broadening the debate on the Family Health Program. Ciênc. Collective health (Online) 2009 [cited in July 25 2014]. 14(suppl 1): 1336-38. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-81232009000800003&lng=pt
15.Ministry of Health (Br). Department of Health Care. Ceiling, accreditation and implantation of the strategies of Community Health Workers, Family Health and Oral Health. Brasília (DF): Department of Primary Care, 2012 [cited in May 06 2016]. Available from: http://dab.saude.gov.br/portaldab/historico_cobertura_sf.php
16.Valentim RAM. PMAQ-AB on-line validity computer program (co-ownership). Natal (RJ): Federal Institute of Education, Science and Technology of Rio Grande do Norte; 2013.
17.Ministry of Health (Br). Department of Health Care. National Program for Improving Access and Quality of Primary Care (PMAQ-AB): protocol for the analysis of consistency and validation of data. Brasília (DF): Ministry of Health; 2012.
18. Brazilian Institute of Geography and Statistics. Research of basic municipal information: profile of Brazilian municipalities 2009 [online]. Rio de Janeiro: 2010. [cited in Dec 11 2016]. Available from: http://www.ibge.gov.br/home/estatistica/economia/perfilmunic/2009/munic2009pdf
19.Almeida PF, Gérvas J, Freire JM, Giovanella, L. Integration strategies between primary health care and specialized care: parallels between Brazil and Spain. Saúde em Debate
[Scielo-Scientific Electronic Library Online] 2013 [cited in May 11 2016]. 37(98): 400-15. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-11042013000300004&lng=en
20. Macedo CA, Teixeira ER, Vago D. Possibilities and limits of welcoming in users' perception. Rev. enferm. UERJ. (Online) 2011 [cited in June 11 2016]. 19 (3):457-62. Available from: http://www.facenf.uerj.br/v19n3/v19n3a20.pdf
21.Pires MRG, Göttems, LBD. Basic health care network in Belo Horizonte: relation with urgency and coordination of care based on the family health strategy. [cited in May 12 2016] Available from: www.politicaemsaude.com.br/anais/orais_painel/056.pdf
22.Lafaiete, RS, Silva CB, Oliveira MG, Motta MC, Villa TC. Research on access to tuberculosis treatment in Itaboraí/RJ. Esc. Anna Nery Rev. Enferm. [Scielo-Scientific Electronic Library Online] 2011 [cited in 11 May 2016]. 15(3): 47-53. Available from: http://www.scielo.br/scielo.php?pid=S1414-81452011000100007&script=sci_arttext
23.Ministry of Health (Br). Grupo Hospitalar Conceição/Teaching and Research Management. Clinical Guidelines/Assistance Protocols. Operational manual. Porto Alegre(RS): Grupo Hospitalar Conceição;2008.
24.Rodrigues LBB, Silva PCS, Peruhype, RC, Palha PF, Popolin MP, Crispim, JA, Pinto IC, Monroe AA, Arcêncio RA. Primary health care in the coordination of care networks: an integrative review. Ciênc. saúde coletiva (Online). 2014 [cited in May 07 2016]. 19 (2): 343-52. Available from: http://www.scielosp.org/scielo.php?script=sci_arttext&pid =
25. Álvarez-Castillo MD Jonsson J, Herrera D. Evaluation of tuberculosis control in an area of the Community of Madrid, Spain (1999–2004). Gac Sanit. [Scielo-Scientific Electronic Library Online] 2011 [cited in May 07 2016]. 25(2):127–32. Available from: http://scielo.isciii.es/scielo.php?script=sci_arttext&pid=S0213-91112011000200008&lng
26.Assis EG, Beraldo AA, Monroe AA, Scatena LM, Cardozo-Gonzales RI, Palha P F et al. Coordination of care in the control of tuberculosis. Rev. Esc. enferm. USP [Scielo-Scientific Electronic Library Online]. 2012 [cited in May 12 2016]; 46(1): 111-8. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0080-62342012000100015&lng=en
27.Cecilio HPM, Marcon SS. Directly observed treatment of tuberculosis in the health professionals' opinion. Rev. enferm. UERJ. (Online) 2016 [cited in Mar 03 2017]. 24(1): e8425. Available from: http://www.facenf.uerj.br/v24n1/v24n1a16.pdf
28.Santos TMMG, NogueiraLT, Arcêncio, RA. Performance of Family Health Strategy professionals in the control of tuberculosis. Acta Paul. Enferm. [Scielo-Scientific Electronic Library Online]. 2012 [cited in May 07 2016]. 25: 954-61. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-21002012000600020&lng=en
29.Hamusse, SD, Demissie M, Lindtjørn Trends in TB case notification over fifteen years: the case notification of 25 Districts of Arsi Zone of Oromia Regional State, Central Ethiopia. BMC public health (Online). 2014 [cited in May 2016 18]. 14: 304. Available from: http://www.biomedcentral.com/1471-2458/14/304
30.Nogueira JÁ. Ruffino Netto A, Monroe AA, Cardozo-Gonzales RI, Villa TCS. Active search for respiratory symptomatic patients in the control of tuberculosis in the perception of community health workers . Rev. eletrônica enferm. (Online) 2007 [cited in May 12 2016]. 9(1): 106-18. Available from: http://www.fen.ufg.br/revista/v9/n1/v9n1a08.htm
31.Sá LD, Gomes AC, Nogueira JA, Villa TCS, Souza KMJ, Palha PF. Intersectoriality and bonding in the control of tuberculosis in Family Health Strategy. Rev. latinoam. enferm. (Online). 2011 [cited in May 12 2016]. 19(2): 387-95. Available from http://www.revistas.usp.br/rlae/article/view/4331/5583
32.Clementino FS, Miranda FAN. Tuberculosis: welcoming and information from the perspective of home visits. Rev. enferm. UERJ. (Online) 2015 [cited in Mar 03 2017]. 23(3): 350-4. Available from: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/4289