ORIGINAL RESEARCH
Occupational accidents involving community health agents
Mirian Cristina dos Santos AlmeidaI; Patricia Campos Pavan BaptistaII; Arlete SilvaIII
I
Nurse. Master in Nursing. PhD student in Sciences: University of São Paulo,
School of Nursing. São Paulo Brazil. E-mail: miriandresp@hotmail.com
II
Nurse. PhD. Associate Professor: University of São Paulo, School of
Nursing, Professional Orientation Department. São Paulo Brazil. E-mail: pavanpati@usp.br
III
Nurse. PhD. Retired Teacher. University of São Paulo, School of Nursing.
São Paulo Brazil. E-mail: arlsilva@uol.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2016.17104
ABSTRACT
Objective: to analyze occurrence of occupational accidents in community health agents (CHAs) in the municipality of Caraguatatuba, São Paulo, Brazil. Method: in this quantitative, descriptive, cross-sectional study, approved by the Research Ethics Committee of Guarulhos University (No. 723/11), data were collected from 137 CHAs, in 2012, using a questionnaire and interview. Results: 59(43.07%) CHAs were found to have had 80 occupational accidents, the most frequent being CHA cyclist injured in traffic accident, by dog bite or by fall; 64(80.00%) were typical to the profession, 13(16.25%) were travel accidents and 3(3.75%) were occupational disease. Only 31(38.75%) of the accidents were reported by Occupational Accident Notification, and 16(20.00%) entailed absence from work. Conclusion: these results alert to the importance of promoting preventive and intervention measures in CHA working conditions.
Keywords: Community health workers; accidents, occupational; occupational accidents registry; occupational health.
INTRODUCTION
Accidents and sickness at work among health workers are the concern of several researchers, highlighting a serious problem in the national and international context1-4. However, there is still a shortage of studies about accidents with primary care workers, which the first level of contact between the population and the health service, approaching mainly health promotion and disease prevention2.
Among several primary health care professionals, the community health worker (CHW) was inserted in several countries for specific populations after the International Conference on Primary Health Care, in 1978, in the former Soviet Union, which advocated health for all5. Currently, this professional is present in public health programs in countries such as Ethiopia, Mozambique, Uganda, Bangladesh, Pakistan, Thailand, Haiti, among others6. In Brazil, the CHW was institutionalized in the context of National Public Health in the 1990s, with the creation of the Community Health Work Program (PACS in Portuguese) and later with the Family Health Program (FHP), now called the Family Health Strategy (FHS). Their work is characterized by the realization of home visits to all the families of their micro-area of coverage, developing individual or collective actions of prevention and health promotion, being an important link between the population and the other members of the FHS. According to the Ministry of Health (MoH), in 1998, there were 59,066 CHWs throughout Brazil. With the expansion of the FHS, the number of CHW increased considerably, reaching 272,718 in August 2016, to serve more than 129 million Brazilians7.
The interest for accomplishing this study was based on the experience of one of the authors as a nurse of the FHS and on the concern about occupational accidents (OA) suffered by CHW with whom she worked. Added to this, there is the limited knowledge about the occurrence of OA with the CHWs, which makes it difficult to organize programs for the prevention and health promotion of these workers that have become of fundamental importance in primary health care at the national level. Thus, this research had the objective of analyzing the occurrences of OA among CHWs of the city of Caraguatatuba - SP.
LITERATURE REVIEW
Occupaional health involves a set of actions that aims to provide promotion, protection, recovery and rehabilitation of health of workers subjected to risks and damages arising from working conditions, including, among other aspects, assistance to the worker victim of OA8. In order to do so, in Brazil, the National Occupational Health Policy is organized in such a way that the principles and guidelines of the Unified Health System (SUS) are observed in all spheres of government for the "development of comprehensive health care for workers, with emphasis on surveillance, aimed at promoting and protecting workers' health and reducing morbidity and mortality resulting from development models and productive processes"9:46.
In this context, OAs are classified as typical: arising from the exercise of professional activity; commuting accidents: occurring during the journey between the residence and the place of work and vice versa; and occupational sickness: produced by the exercise of work belonging to the branch of activity included in the Brazilian Social Security Regulation10. All OAs occurring with workers hired under the Consolidation of Labor Laws (CLT) must be notified by the company, through an Occupational Accident Report (OAR), to Social Security, regardless of the type of accident and the need to leave from employment or not11.
METHODOLOGY
This is a descriptive, cross-sectional field study with a quantitative approach. Data collection was performed in January 2012, at the basic health units (BHU) of the city of Caraguatatuba-SP-Brazil, which encompasses 22 FHS, with a total of 166 CHWs, hired under the CLT regime.
The sample consisted of 137 CHWs. Of the 29 CHWs that did not participate in the study, four were on medical leave, 16 were on vacation, two refused to participate in the study and seven were dismissed during the data collection period.
Data were collected by one of the researchers after authorization from the institution and approval by the Research Ethics Committee of the Guarulhos University (Opinion no. 723/11). During a FHS team meeting, the CHWs were invited to participate in the survey, receiving all pertinent information and, those who agreed, signed the Free and Informed Consent Form. A questionnaire containing sociodemographic and occupational data was applied, and soon after the CHWs were interviewed, in a reserved room, about the occurrence and description of OAs, notification and need for hospitalization and/or leave. The OAs were grouped according to the International Statistical Classification of Diseases and Health-Related Problems (ICD 10) and a simple descriptive statistical analysis of the data was performed.
RESULTS AND DISCUSSION
Characterization of CHWs and OAs
Of the 137 CHWs participants in the study, 129 (94.16%) were female, aged between 19 and 62 years (mean 34.79 years; SD 9.96) and 83 (60.58%) reported having stable marital status.
The time of work as CHW ranged from 25 days to 11 years (mean 3.17 years; SD 2.88), with a weekly workload of 40 hours. To perform the work, mainly home visits, 104 (75.91%) CHWs reported using the bicycle as a means of transportation; 16 (11.68%) did it on foot; 14 (10.22%) used bicycle or did it on foot; 2 (1.46%) used motorcycles and 1 (0.73%) used a bicycle or motorcycle.
Among the 137 CHWs interviewees, 59 (43.07%) reported having suffered OA during their professional career: 44 (74.58%) reported one OA, 7 (11.86%) reported two OAs, 6 (10,17 ) three OAs, 1 (1.69%) four OAs and 1 (1.69%) could not quantify them.
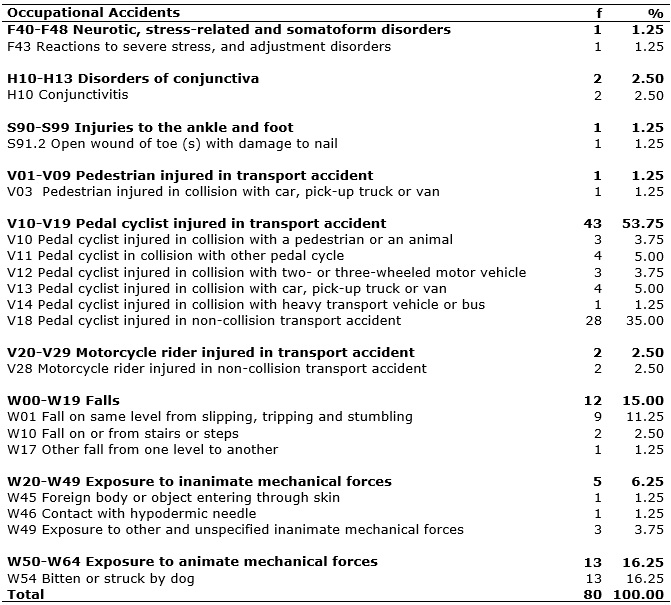
The 80 (100%) OAs reported by the 59 CHWs were grouped according to the International Statistical Classification of Diseases and Health-Related Problems (ICD 10), and the most prevalent was the external causes of morbidity and mortality (V01-Y98), according to data presented in Table 1.
TABLE 1:
Distribution of work-related accidents reported by community health workers
according to the International Statistical Classification of Diseases and
Health-Related Problems (ICD 10). Caraguatatuba, SP, 2012.
Most OAs occurred with pedal cyclists injured in transport accidents, followed by dog bite or strike, falls and exposure to inanimate mechanical forces, according to Table 1.
Regarding the type of OA, 64 (80%) were typical, 13 (16.25%) as commuting accidents and 3 (3.75%) were occupational diseases.
According to the place of occurrence of typical and commuting OAs, 59 (76.62%) occurred on public roads, followed by 12 (15.58%) in the backyard of the patient's home, 3 (3.90%) at the BHUs, 2 (2.60%) on the stairs of the patient's building and 1 (1.30%) at the gas station, when the CHW was calibrating the tire of his bicycle.
Of the 80 OAs, 49 (61.25%) were not officially notified through OAR. When asked about the reason for non-notification, they reported that they sometimes reported the accident to the nurse, physician or nursing assistant of the FHS and that they often did not notify it because there were no serious injuries.
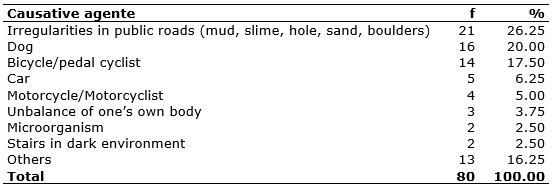
The causative agent of OAs most pointed out by CHWs was irregularities in the public road, dog and bicycle/ pedal cyclist, according to data presented in Table 2. Others, such as slippery floor in the BHU, broken toilet, can, thorn, sweater, truck, pedestrian, umbrella, debris, tile covering deactivated septic tank, other CHW's shoes, capillary glycemia lancet and pressure at work/home disagreement, were also pointed out.
TABLE 2:
Distribution of occupational accidents with community health workers,
according to the causative agent. Caraguatatuba, SP, 2012.
The parts of the body affected by OAs were: 50 (51.03%) - lower limbs, followed by 26 (26.53%) upper limbs, 8 (8.16%) - thorax, 7 (7.14%) - pelvic region, 6 (6.12%) - head and 1 (1.02%) - abdomen, totaling 98. Since there were 80 OAs, some affected more than one part of the body.
Of the 97 injuries identified, superficial and soft-tissue injuries were the most frequent with 46 (47.43%) occurrences, followed by 38 (39.18%) - contusion/hematoma/edema. Also, there were 5 (5.15%) - dislocation/sprain due to falls and transport accidents; 2 (2.06%) - traumatic injuries incised by the handling of debris (broken toilet and can) in the backyard of the patient's home during a dengue prevention visit; 2 (2.06%) traumatic injuries resulting from accident with capillary glycemia test lancet and perforation of lower limb with thorn during home visit; 1 (1.03%) deep soft tissue lesion by dog bite in the gluteal region; 1 (1.03%) hand fracture due to collision between CHW pedal cyclist and a car; 1 (1.03%) concussion by collision of the CHW pedal cyclist with a pedestrian and; 1 (1.03%) nail injury caused by accidental footing with shoe in the second left foot pod.
A total of 12 (20%) OAs resulted in leave from work activities for a minimum of one day and a maximum of 35 days (mean 8.93; SD 10.15 days). The most frequent period was 1 to 4 days, with 7 (43.75%) occurrences.
Analysis
A study carried out in Sidrolândia-MS-Brazil found that 26.82% of CHWs were victims of OAs. This percentage is lower than that observed in the present study, in which almost half of CHWs already suffered some type of OA12.
Most OAs was related to transport accidents involving a bicycle, since it is the most used means of transportation by the CHWs of Caraguatatuba-SP-Brazil, either to develop their home visits in their micro-area of coverage or to commute from home to work and vice versa; 35% of these accidents occurred without collision, when the bicycle skidded, stopped abruptly because some object had entwined in the wheel, and due to lack of maintenance (problem in brakes, bicycle handlebar that broke off), among other causes.
The bites or strokes caused by dogs were the second cause of OAs and occurred on the public road and also in the backyard of patients' homes, often in the presence of the owner of the animal. It is known that dog bites are highly infectious and can transmit rabies and other diseases due to the microorganisms present in the animal's saliva, the environment and the victim's skin, and it is necessary to provide prophylactic measures to prevent human rabies, tetanus and antimicrobial treatment according to individual assessment of cases13.
Falls were the third cause of OAs and encompassed falling from one's own height by slipping or tripping; falling from stairs of a building during a home visit in a dark environment; and falling from one level to another when CHW fell into a deactivated septic tank in the backyard of a user's home.
In another study with CHW, falls were the most prevalent (54.54%), followed by dog bite, insect bites and accident with barbed wire12. Studies conducted in Canada with health workers have identified that the risk of falls was significantly higher in support workers, CHWs, women and people over 60 years of age. The activities that most contributed to falls were walking or running and pushing or picking up objects, and the main factors that led to falls were the type of tread (slippery, uneven surfaces and rugs) and working in open air14.
Exposure to inanimate mechanical forces was the fourth cause of OAs in CHWs, and occurred by a foreign body or object entering in through skin, when a thorn pierced the foot of the CHW that was wearing sandals during a home visit; perforation with a hypodermic needle, when a CHW was signing the time record sheet on a table where the nursing assistant performed a blood glucose test, The needle fell to the floor and CHW, when picking it, pierced the finger of the hand; cut with can and broken toilet during a dengue prevention visit in a residence yard; and the bicycle rim that broke when CHW calibrated the tire, injuring his the upper limb. The accident that caused injury to one of the nail-toe was caused by the CHW who wore a wooden clog and accidentally stepped on the foot of another CHW that was wearing a sandal, instantly extracting the nail from the second left foot pod.
Studies on OAs with CHWs are still scarce, but recent research including all health professionals pointed CHWs as victims of accidents with biological/sharp material15,16. These data point to the importance of prophylaxis against Hepatitis B and tetanus for CHWs.
Only three occurrences of work-related diseases were identified: two from conjunctivitis, acquired at work during a conjunctivitis outbreak in the assisted population, and one from stress, perhaps due to lack of knowledge about the types of OAs. The low number of work-related illnesses has also been identified in research carried out with health professionals and in national OA statistics, whose records indicate the predominance of typical accidents, followed by commuting accidents10,17,18.
Literature has shown high psychological demand in the work of CHWs. This worker, as a link between the community and the health service, coexists with patients' biological and social problems, experiencing feelings of impotence and fragility, as well as receiving demands from community due to low resolution of health problems, which can result in chronic stress and, consequently, high levels of burnout19-23.
Lack of notification of OAs is justified by CHWs, in most cases, due to the low severity of the accidents. However, it may also be related to the fact that the registration of the notification is centralized with the company's administrative sector, which is the FHS manager (in the scenario of the present study). There is still the bureaucracy required in completing the OAR. When suffering an OA, the CHW must observe a protocol - undergo a medical consultation (at the BHU itself or in another health service), where a medical certificate must be issued, stating the date, time, accident circumstance and ICD-10 code. Afterwards, the worker must attend the administrative department of the company, where the OAR will be held, as well as other decisions, if necessary, such as scheduling an appointment with an occupational physician for medical expertise. When accidents are mild, without physical injuries or even simple injuries such as bruises and hematomas, professionals mistakenly believe that medical care is not necessary, which is required for conducting an OAR and, in addition, they complain that they would have to go from where they live and work to the administrative sector of the company, which demands time.
In another study with CHWs, no OA was reported12. Underreporting of OAs is not a recent problem and also occurs with other professionals, being justified by the irrelevance of the damage, the frequency with which it occurs, the lack of knowledge of the protocol for OA care, the bureaucracy to perform the OAR, work overload and negligence24,25.
Information on the importance and obligation of notification, regardless of the seriousness of the OA, and decentralization of notifications to the BHUs and other health services may minimize underreporting.
In the present study, no occupational disease was reported. In general, typical and commuting OAs are more easily reported compared to occupational diseases, which require an assessment and comparison of the causal link to be recognized as such, leading to underreporting of workers' sickness data"26:288.
Irregularities in public roads such as holes, mud, mud, sand and boulders cause most of the OAs among CHWs and are related to falls of from one's own height, slips, tripping, falling of bicycle or motorcycle.
Dogs are also important cause of accidents, either by bites or by entering the front of bikes or motorcycles, resulting in falls.
Public areas with no pavement, which are damp and slippery, and dogs are part of the risks present in the work of these professionals27.
Bicycles or pedal cyclists were the third most frequent causative agents, as this is the main means of transport used by CHWs to carry out their work in Caraguatatuba-SP-Brazil.
A survey of pedal cyclists, workers from Pelotas-RS-Brazil, found that among the 293 interviewees, 5.5% were injured in the last year, most of them being mild accidents (scratching or bruising), with no need to leave from work; 15% of the bikes examined had no brakes, and only 0.3% had all the safety equipment required by the Brazilian Traffic Code, namely, horn and night front, rear and side signage, as well as signage in the pedals and rear-view mirror at the left side, not being mandatory to wear a helmet28.
Another study conducted in Ontario, Canada, used forensic analysis data on 129 deaths of pedal cyclists aged 10-83 years, and found that riding a bicycle without a helmet is associated with an increased risk of death from head injury29. The importance of carrying out routine maintenance of bicycles, as well as following traffic regulations, the construction of bicycle lanes and the use of helmets is of utmost importance.
Agents that cause accidents among CHWs are specific to their work process, encompassing, in most cases, the environment and the instruments used in their work, which requires a high degree of attention during their work activity. Also, personal protective equipment (PPE), which prevents accidents, is extremely relevant.
As for the affected part of the body, the most frequent ones were the lower limbs, followed by the upper limbs, caused mainly by bicycle transport accidents and dog bites. Most of the lesions occurred in the pelvic, abdominal, thoracic and head regions and resulted from traffic accidents and falls.
Comparison between CHWs of this study and postmen, who carry out their work on foot, by bicycle or motorcycle, from house to house, showed that the most affected parts of the body in OAs are similar between those categories. Among postmen who referred to dog bites, more than half suffered injuries in the hands or feet and legs30.
The majority of OAs among CHWs resulted in superficial soft tissue injuries (dog bruising and superficial bite 47.43%) and bruising/hematoma/edema (39.18%). These results denote the importance of the use of personal protective equipment (PPE) such as trousers with thick jeans, for the protection of the lower limbs. Since Caraguatatuba is a seaside town, with peculiar habits of life, the uniform of CHWs of this town is composed of a short-sleeved T-shirt or vest and lightweight bermudas, which does not contribute to the prevention or minimization of injuries in case of accidents.
Leave from work was not necessary for most of the injured CHWs. This data is similar to the survey conducted with nursing professionals, in which 88.15% of the workers did not need to ask for temporary leave from work17.
None of the CHWs needed to be hospitalized due to the OA; some received care in the emergency room of the municipality and, after spending a few hours under observation, were sent home.
The period of absence from work averaged 8.93 days, and the sum was 143 days, equivalent to 4 months and 23 days. This can have consequences not only for workers who are victims of accidents, but also for users of the health service and other colleagues, who are overloaded with the tasks of those who have been absent. For each day of absenteeism, about 10 to 12 families stop receiving care. This reinforces the need to invest in the prevention of OAs, since these do not only harm the worker, but the care team and the community in general.
CONCLUSION
The analysis of the OAs occurring with CHWs point to the need for public policies on occupational safety, and the adoption of strategies for prevention of accidents and to health promotion of these workers is crucial.
Safety measures, such as prophylaxis against tetanus and Hepatitis B and use of PPE - such as jeans, closed shoes and helmet for those who use bicycle as a transport -, should be adopted and controlled regularly by the employing institution.
CHWs should also to be oriented on the most frequent OAs of their professional category, the notification thereof, importance of the appropriate use of the PPE. These measures are of extreme importance for the prevention of accidents and formulation of public policies for promotion and protection of these workers' health.
A limitation of this study is the high proportion of OAs involving bicycles, which may be related to the characteristics of the research field, a coastal city where the bicycle is a very common means of transportation. The reduced contingent of subjects and only one scenario prevent the generalization of results. This study should be replicated in a population of workers representing this universe in order to reinforce and support intervention and preventive measures for these workers, who are the basis of Brazilian public health care.
REFERENCES
1.Gärtner FR, Nieuwenhuijsen K, van Dijk FJ, Sluiter JK. The impact of common mental disorders on the work functioning of nurses and allied health professionals: a systematic review. Int J Nurs Stud. 2010; 47(8): 1047-61.
2.Prochnow A, Magnago TSBS, Tavares JP, Beck CLC, Silva RM, Greco PBT. Profile of occupational accidents published in Brazilian studies. Health (Santa Maria).2011; [cited in 2016 Feb 17] 37(1): 77-90. Available in: https://periodicos.ufsm.br/revistasaude/article/view/2900/2060
3.Alamgir H, Cvitkovich Y, Yu S, Yassi A. Work-related injury among direct care occupations in British Columbia, Canada. Occup Environ Med. 2007; [cited in 2016 Feb 17] 64(11):769-75. Available in: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2078424/pdf/769.pdf
4.Ribeiro RP, Martins JT, Marziale MHP, Robazzi MLCC. Work-related illness in nursing: an integrative review. Rev esc enferm USP. [Scielo-Scientific Electronic Library Online] 2012 [cited in 2016 Feb 17]. 46(2):495-504. Available in: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S008062342012000200031&lng=en&nrm=iso&tlng=en
5.Silva JA, Dalmaso ASW. Community health workers and their attributions: the challenge for the human resources training process in health. Interface-Comunic.Saúde,Educ. 2002; [cited in 2016 Feb 17] 6(10): 75-96. Available in: http://www.redalyc.org/articulo.oa?id=180114097007
6.World Health Organization. Global experience of community health workers for delivery of health related millennium development goals: a systematic review, country cases studies, and recommendations for integration into national health systems. Pakistan: WHO; 2010. [cited in 2016 Mar 8] Available in: http://www.who.int/workforcealliance/knowledge/publications/CHW_FullReport_2010.pdf?ua=1
7. Ministry of Health (Br). Health Website [Internet website]. History of Family Health Coverage. [cited in 2016 Sep 20] Available in: http://dab.saude.gov.br/portaldab/historico_cobertura_sf.php
8. Brazil. Law no. 8080 of September 19, 1990. Provides for the conditions for the promotion, protection and recovery of health, organization and operation of corresponding services and other measures. Official Journal of the Union, Brasília (DF) 1990 Sep 20; Sec.1:18055.
9. Ministry of Health (Br). Minister's office. Decree no. 1,823, of August 23, 2012. It institutes the National Policy of Occupational Health. Official Journal of the Union [of the Federative Republic of Brazil], Brasília (DF) 2012 Aug 24; Sec. 1, 165:46-51.
10.Ministério da Fazenda (Br). Anuário estatístico da previdência social-2015. Brasília; 2016.
11. Brazil. Law no. 8213 of July 24, 1991. Provides for social security benefit plans and provides other measures. Official Journal of the Union, Brasília (DF), 1991 jul. 24; Sec.1: 14809.
12.Rossi DAN, Contrera-Moreno L. Risks to occupational health of the community health workers of Sidrolândia, MS. Ensaios e Ci. 2006; [cited in 17 fev 2016] 10(3): 191-200. Available in: http://www.redalyc.org/pdf/260/26012809019.pdf
13.Brook I. Management of human and animal bite wound infection: an overview. Curr Infect Dis Rep. 2009;11(5):389-95.
14.Drebit S, Shajari S, Alamgir H, Yu S, Keen D. Occupational and environmental risk factors for falls among workers in the healthcare sector. Ergonomics. 2010; 53(4): 525-36.
15.Dias MAC, Machado AA, Santos BMO. Occupational accidents due to exposure to biological material: portrait of a reality. Medicine (Ribeirão Preto) 2012; [cited in 2016 Feb 17] 45(1):12-22. Available in: http://www.revistas.usp.br/rmrp/article/view/47479/51207
16. Julio RS, Filardi MBS, Marziale MHP. Occupational accidents with biological material occurred in municipalities of Minas Gerais. Rev Bras Enferm. [Scielo-Scientific Electronic Library Online] 2014 [cited in 2016 Feb 17]. 67(1): 119-26. Available in: http://www.scielo.br/pdf/reben/v67n1/0034-7167-reben-67-01-0119.pdf
17- Ribeiro EJG, Shimizu HE. Occupational accidents with nursing workers. Rev Bras Enferm. [Scielo-Scientific Electronic Library Online] 2007 [cited in 2016 Feb 17]. 60(5): 535-40. Available in: http://www.scielo.br/pdf/reben/v60n5/v60n5a10.pdf
18-Ribeiro PC, Ribeiro ACC, Lima Júnior FPB. Profile of occupational accidents occurred in a hospital in Teresina, PI. Cogitare enferm. 2010; [cited in 2016 Feb 17] 15(1):110-6. Available in: http://revistas.ufpr.br/cogitare/article/view/17181/11316
19.Coriolano MWL, Lima LS. Focus groups with community health workers: support for the understanding of these social actors. Rev enferm UERJ, 2010; [cited in 2016 Feb 17] 18(1):92-6. Available in: http://www.facenf.uerj.br/v18n1/v18n1a16.pdf
20.Trindade LL, Lautert L. Syndrome of Burnout among the workers of the Strategy of Health of the Family. Rev esc enferm USP. [Scielo-Scientific Electronic Library Online] 2010 [cited in 2016 Feb 17]. 44(2):274-9. Available in: http://www.scielo.br/pdf/reeusp/v44n2/en_05.pdf
21.Santos IER, Vargas MM, Reis FP. Occupational stressors in community health workers. Rev Psicol, Organ Trab. 2014; [cited in 2016 Feb 17] 14(3):324-35. Available in: http://pepsic.bvsalud.org/pdf/rpot/v14n3/v14n3a08.pdf
22.Mota CM, Dosea GS, Nunes PS. Assessment of the presence of burnout syndrome among community health workers in the city of Aracaju, Sergipe, Brazil. Ciênc saúde coletiva. [Scielo-Scientific Electronic Library Online] 2014 [cited in 2016 Feb 17]. 19(12):4719-26. Available in: http://www.scielosp.org/pdf/csc/v19n12/1413-8123-csc-19-12-04719.pdf
23.Barroso SM, Guerra ARP. Burnout and quality of life of community health workers in Caetanópolis (MG). Cad. saúde colet. [Scielo-Scientific Electronic Library Online] 2013[cited in 2016 Feb 17]. 21(3): 338-45. Available in: http://www.scielo.br/pdf/cadsc/v21n3/v21n3a16.pdf
24.Oliveira AC, Gonçalves JA. Occupational accident with sharp edge material among workers of an operating center. Rev esc enferm USP. [Scielo-Scientific Electronic Library Online] 2010 [cited in 2016 Mar 31]. 44(2):482-7. Available in: http://www.scielo.br/pdf/reeusp/v44n2/en_34.pdf
25.Theodoro ED, Miotto MHMB, Barcellos LA, Grillo CHB. Prevalence of occupational accidents in dentists. Rev Bras Pesquisa em Saúde. 2009; [cited in 2016 Mar 31] 11(4):4-9. Available in: http://periodicos.ufes.br/RBPS/article/view/348/259
26.Leite PC, Silva A, Merighi MAB. The working woman in nursing and work-related musculoskeletal disorders. Rev esc enferm USP. [Scielo-Scientific Electronic Library Online] 2007 [cited in 2016 Mar 31]. 41 (2): 287-91. Available in: http://www.scielo.br/pdf/reeusp/v41n2/15.pdf
27. Nascimento GM, David HMSL. Risk assessment in the work of community health workers: a participatory process. Rev enferm UERJ. 2008; [cited in 2016 Feb 17] 16(4): 550-6. Available in: http://www.facenf.uerj.br/v16n4/v16n4a16.pdf
28.Bacchieri G, Gigante DP, Assunção MC. Determinants and patterns of bicycle use and traffic accidents suffered by pedal cyclist workers in the city of Pelotas, Rio Grande do Sul, Brasil. Cad Saúde Pública. [Scielo-Scientific Electronic Library Online] 2005 [cited in 2016 Mar 31]. 21(5):1499-508. Available in: http://www.scielo.br/pdf/csp/v21n5/23.pdf
29.Persaud N, Coleman E, Zwolakowski D, Lauwers B, Cass D. Nonuse of bicycle helmets and risk of fatal head injury: a proportional mortality, case–control study. CMAJ. 2012; [cited in 2016 Mar 31] 184(17):E921-3. Available in: http://www.cmaj.ca/content/184/17/E921.long
30.Oliveira EA, Manosso RM, Braune G, Marcenovicz PC, Kuritza LN, Ventura HLB et al. Neighborhood and postal worker characteristics associated with dog bites in postal workers of the Brazilian National Postal Service in Curitiba. Ciên saúde coletiva. [Scielo-Scientific Electronic Library Online] 2013 [cited in 2016 Mar 31]. 18(5): 1367-74. Available in: http://www.scielo.br/pdf/csc/v18n5/22.pdf