FIGURE 1: Flowchart of the searched articles for review Integrative literature on congenital syphilis.
REVIEW ARTICLES
Congenital syphilis as seen by nursing
Valéria Silva de MelloI; Rosângela da Silva SantosII
I
Nurse Servant of the City Hall of Rio de Janeiro and employed at the Fernando Magalhães Maternity Hospital. Master's Student at the School of Nursing at
the State University of Rio de Janeiro, Brazil. Email: valsilmel@gmail.com
II
PhD in Nursing. Assistant Professor in the Nursing Graduate Program at the State University of Rio de Janeiro, National Research Council researcher 1C.
Support Foundation for Research of Rio de Janeiro. Brazil. Email: rosangelaufrj@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2015.17103
ABSTRACT
This integrative review discussed scientific publications relating to congenital syphilis and to nursing. The guiding question was: What factors guide nursing care for pregnant women as regards preventing and controlling congenital syphilis? Data were collected from April to May 2015 from the following databases: Latin American and Caribbean Health Sciences Literature, Medical Literature Analysis and Retrieval System Online and Scientific Electronic Library Online, with the descriptors 'congenital syphilis' and 'nursing', in Portuguese and English. Eight full publications were selected, from the period 2005 to 2014. Three categories emerged: risk factors for congenital syphilis; inappropriateness of the care provided; and health staffs' difficulties in syphilis prevention and control. Prevention and control of syphilis in pregnancy and congenital syphilis remain a challenge for the Ministry of Health. The study results may help improve the quality of health personnel's work.
Keywords: Congenital syphilis; primary care nursing; pregnant women; antenatal care.
INTRODUCTION
Syphilis is an infectious disease, which has challenged humanity for centuries. It became known in Europe in the 15th century when a very serious epidemic of syphilis broke out. The rapid spread across the continent transformed it into one of the world's leading plagues1.
Despite not occupying an important place in maternal mortality, it has a high prevalence and ease of vertical transmission. During pregnancy, childbirth infection is worrying due to its offense in the congenital form, increasing the perinatal mortality figures, abortion and neurological sequelae in newborns 2.
Syphilis in pregnancy and congenital syphilis reached proportions not justified on the availability of diagnosis and treatment, as well as their numbers do not reflect the expected result of the constant Ministry of Health campaigns to fight the disease. It is also an indicator of prenatal care quality, because when this is done correctly, there is no reason to justify the birth of children with syphilis3.
In this context, we drew the following guiding question: What aspects guide the nursing care for pregnant women, regarding prevention and control of congenital syphilis? To answer this question an integrative review with the following objective: discuss scientific publications related to congenital syphilis and nursing.
LITERATURE REVIEW
The origin of syphilis is controversial. The first theory holds that the disease was endemic in America and that would have been taken to Europe by Christopher Columbus's sailors. The second theory, the old world supports the treponematoses already existed in European territory and acquired an increased differentiation and allowing sexual transmission and triggering epidemics4.
Syphilis is caused by the bacterium, Treponema pallidum, and affects virtually all organs and systems. The main forms of transmission are the sexually (acquired) and vertical (congenital), from mother to fetus5.
The proposal of the Ministry of health was to eliminate congenital syphilis until the year 2000; this goal was not achieved and it continues to face the increasing incidence of congenital syphilis in the population. The notification of cases of congenital syphilis in Brazil increased by 34% between the years 2010 and 2011. The region that has the highest incidence rate of congenital syphilis is in the Northeast. Among the States, the highest incidence is in Rio de Janeiro6.
This issue has mobilized not only Brazil, but also the international community. The Pan American Health Organization (PAHO) and the United Nations Children's Fund (UNICEF), in 2009, launched the "regional initiative for the Elimination of mother-to-child transmission of HIV and syphilis in Latin America and Caribbean". In 2010, this regional initiative articulated to the "Global Plan for the Elimination of new HIV infections among children until 2015 and keep their mothers alive". That same year, PAHO's Member States approved the "plan of action for the Elimination of mother-to-child transmission of HIV and syphilis, congenital", setting goals for the year 2015 to reduce the HIV transmission rate and incidence rate of congenital syphilis.
In Brazil, the system of epidemiological surveillance and Compulsory Notification of diseases was created in 1976, by Presidential Decree No. 78.231. In 1986, the congenital syphilis became national notifiable disease by Ordinance No. 542 of 22 December; syphilis in pregnant women became part of the National Surveillance System in 2005. In 2014, the Ordinance No. 1.271 was published, which also included the notification of acquired syphilis7 .
In 2011, the Stork Network was established, to ensure the mother and child a care network. Among its actions are the prevention and treatment of sexually transmitted infections (STI's), with provision of rapid tests for syphilis and HIV7.
METHODOLOGY
The integrative literature review consists of a systematic survey of publications about specific topic providing synthesize knowledge and incorporate the implementation of the results of the studies carried out8. The purpose is to gain understanding of a given phenomenon based on previous studies. Allowing the critical appraisal and synthesis of available evidence the subject investigated. Providing updates on the subject using relevant data at different times and places. The final product is the current knowledge of the subject under investigation, identifying gaps that will target the development of future research9. It consists of six phases: identification of the theme; Search in the literature; definitions of information; categorization of studies; analysis of the results and the knowledge synthesis10.
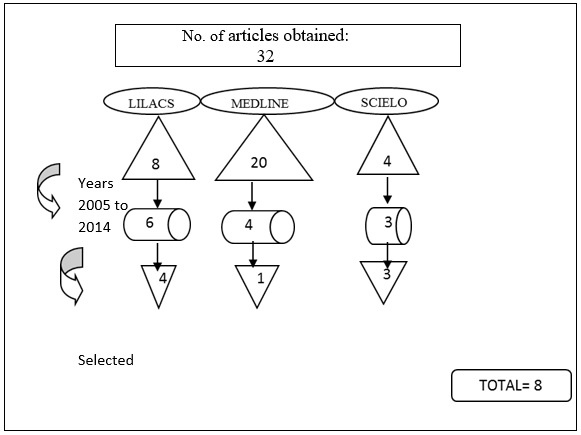
A search was held in the months of April and May 2015, in the following databases: Scientific Electronic Library Online (SCIELO), Latin American and Caribbean Literature in Health Sciences (LILACS) and Medical Literature Analysis and Retrieval System Online (MEDLINE). It was used, the following descriptors and their combinations in the Portuguese and English languages: congenital syphilis and nursing. The inclusion criteria for the selection of the articles were publications in Portuguese and English; articles in their entirety the one representing congenital syphilis and its relationship with nursing and publications indexed in the period from 2005 to 2014.
When starting the search, we found 32 studies: eight articles in LILACS, 20 in MEDLINE and four articles in SCIELO. When applying the timeframe of 2005-2014, they were reduced to six articles in LILACS, four in MEDLINE and three in SCIELO. It was found that five articles were not related to the study objectives and were excluded. The final selection of the sample totaled eight articles: four in LILACS, one in MEDLINE and three in SCIELO. See Figure 1.
FIGURE 1:
Flowchart of the searched articles for review Integrative literature on congenital syphilis.
We constructed an instrument for data collection with the following information: title, authors, year, publication, country, language, and type of study. The eight articles11-18 were assigned with the identification of A1 to A8 for the facilitation and organization of the data found.
RESULTS AND DISCUSSION
The thematic analysis phase through the reading in full of all articles11-18, followed by the identification of the aspects required for categorization. See Figure 2.
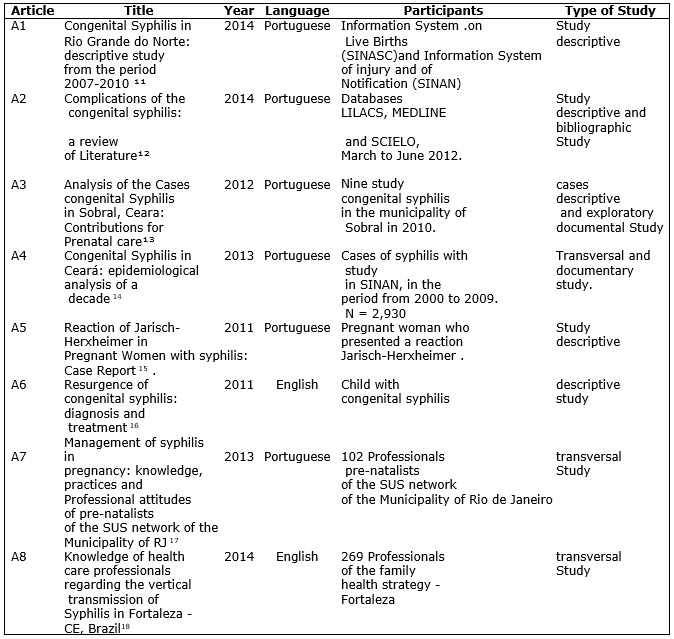
FIGURE 2: Identification of articles selected from the Literature on congenital syphilis. Period 2011-2014.
The results found in the publications were defined in three categories: Risk factors of congenital syphilis; Nursing care provided to pregnant women; and professional Difficulties in the prevention and control of syphilis.
Risk factors of congenital syphilis
Of the eight articles analyzed, five show that pregnant women with syphilis have a low social level, little or no schooling11-14.17. One of the14studies notes in its sampling that more than half are illiterate.
Another study on the epidemiological profile of congenital syphilis, in the municipality of Christmas, showed that mothers belonging to disadvantaged social strata have little access to information required to avoid infection and consequent vertical transmission of syphilis; the diagnosis of the disease, are unaware of the importance of a complete and effective treatment. The socioeconomic factors, such as low education and low income are determinants of numerous diseases in public health. Uneducated mothers and mothers whose families are from low-income families have a higher risk of a pregnancy ending in fetal death than mothers who are above these levels19.
The sexual precocity, unprotected sex, the increase of teenage mothers, illicit drug use, smoking and alcoholism are discussed in two surveys conducted in Ceará13,14 on the epidemiological profile of congenital syphilis, in that State. And it found that such factors are present in most cases 13,14. These factors are also emphasized in another bibliographical review study12.
A final project in Minas Gerais, Brazil, in the family health strategy20, corroborates these results and ratifies the beginning of sexual life of young people increasingly occurs early in a non-adequate non-programmed, unplanned and nearly always insecurely. Many teenagers have no awareness of the seriousness of the STI's and its consequences in the design. The non-use of condoms or their inappropriate use can cause not only infection by sexually transmitted diseases as cause unwanted pregnancy20.
It showed up in this integrative review as a risk factor for re-infection of syphilis and non-treatment partners13, 14, 17,18. Such research examined the knowledge of pre-natalist professionals and the quality of prenatal care, pointing out that the magnitude of the issue has not yet become visible to the healthcare professionals who treat women with syphilis. In addition to the partner's treatment, not in some records they aren't even mentioned.
Another study21 adds the reflection of that special attention is needed from the professionals who practice prenatal care, offering them proper training and monitoring of activities and associated with the prevention of congenital syphilis. It is necessary to find strategies for integrating partners during the pregnancy period.
Nursing care provided to pregnant women: inadequacy
The care provided in the treatment of congenital syphilis was addressed by all of the publications. The effectiveness of treatment is proven in a case study, in which a newborn, showing signs of congenital syphilis in a serology test, and the proper treatment was started, with crystalline penicillin for a period of 10 days. He was accompanied in interdisciplinary consultation with specialists in pediatric infectious diseases. As expected, the titles of the examinations for syphilis were decreasing and the child was discharged, stable and prosperous, with 38 weeks of age16. This report shows that prevention, appropriate treatment and control of syphilis are possible. It is essential to the assessment of prenatal care quality that is being provided in healthcare facilities.
A bibliographical review study12found prenatal care failure and difficulty of access. In addition to inappropriate treatment includes the deficit of information on the effects of syphilis to the fetus and prophylactic measures of congenital syphilis.
Another study, conducted in the municipality of Araguari-MG, Brazil, exemplifies a strategy that has brought good results. Community health agents identify women with menstrual delay in the community and immediately schedule the first appointment for a possible diagnosis of pregnancy. This speeds up the examinations, at an early stage identifying the issues and accelerates the relevant22treatments. This job of locating these pregnant women is part of the guidelines of the Family Health Strategy Program.
Certain publications in the period researched, found that pregnant women with positive serology for syphilis are treated or are inappropriately, the partners are not treated and, consequently, high numbers of women who did receive prenatal diagnosis of syphilis at the time of delivery 11-15,17,18.
Situations that collaborate to low quality in assistance are referred to in research in Ceara14 and in Rio de Janeiro, Brazil 17. Being that pregnant women don't return to get exam results; partners are not treated; delays occur the result; lack access to the treponemic examination; many hospitals do not offer the serological test routinely for pregnant women, back to mother and baby to the community with the possibility of having syphilis.
It is noted also the flaw in the follow-up of children treated with congenital syphilis. An exploratory study examined nine cases of congenital syphilis in the year 2010, Ceará, Brazil, and found that only one held follow-up after treatment, two started and did not finish13.
To achieve the target proposed by the Ministry of health for the eradication of syphilis, there are essential improvements in the quality of epidemiological surveillance, associated with the correct application of recommended for the care of pregnant women and infants affected by the disease. In the period 2007-2010, in Rio Grande do Norte, more than two thirds of cases of congenital syphilis came from mothers who had received prenatal care did not justify such an occurrence11. Using the contribution of a study of social representations of pregnant women in prenatal care, there is the finding that prenatal means a key moment for the identification of diseases that pose a risk to maternal health and the newborn21. The health professional as well as the entire multidisciplinary team should find space for discussion and guidance of the cases, with a focus on a process of care dedicated to biological, psychological, and cultural aspects of the pregnant woman. The professionals involved racing responsibilities sharing about the service provided in the prenatal period.
Professional difficulties in the prevention and control of syphilis
The difficulties of health professionals on the prevention and control of syphilis are evaluated by almost all of the publications11-14,16 -18.
An epidemiological study, analyzing the congenital syphilis in late 2000 to 2009, in Ceará, Brazil, emphasizes that health professionals are not prioritizing congenital syphilis as a public health problem; prevention measures are being ignored; noted the lack of uniformity in conduct for the diagnosis and treatment of syphilis; failures occur in the notification mechanism and records in records, missing important information14. Contributing to this theme, another study performed, too, in Ceará, Brazil, in 12 family health centers, in 2009, which reinforces the professional to receive the expectant mother must be properly qualified, having a look beyond the physical nature, attentive to emotional, economic and family factors, as these can have influence on the membership of the prenatal consultation and, consequently the follow-up23.
Among the eight publications11-18, two exploratory studies evaluate specifically the knowledge and expertise of health professionals in the management of syphilis17,18.
A study was carried out in Rio de Janeiro, Brazil, with 102 pre-natalists from the SUS network, representing 70% of the sample. The professionals had correct knowledge of the ways of transmission of syphilis and affirmed: having participated in training on management of syphilis in pregnancy in the last five years; know and approve of congenital syphilis research reports. On the other hand, it was found that the same professionals revealed: inappropriate conduct in relation to partners, or not addressing or sending request for examination or treatment through of the pregnant woman; barriers related to the knowledge and familiarity with the content of the assistance protocols; difficulties in addressing the STI's17.
The other study was conducted with 515 professional of the family health strategy, in Ceará, Brazil. It found that there were health professionals who do not have adequate knowledge about the measures recommended by the Ministry of Health for the prevention and control of congenital syphilis. The professionals demonstrated lack of knowledge on the diagnosis, treatment and follow-up of pregnant women with positive results for syphilis. A high percentage of professionals failed to correctly identify the recommendation of the treponemal and nontreponemal tests; 21.9% of physicians reported that they would treat pregnant women who are allergic to penicillin inappropriately; 56.7% of professionals showed lack of knowledge about treatment for pregnant women in the secondary stage of syphilis; more than half of them had never undergone training related to syphilis18.
Similar results were obtained in an epidemiological study conducted in Natal, Brazil, in the 2008-2010 period, which discusses the causes of neonatal deaths avoidable by adequate attention to women during pregnancy relating them to the nursing care during the prenatal period. It proved that neonatal mortality might be related to preventable causes, poor access to health services, and the lack of quality in care for the prenatal, childbirth and newborns 24.
A study in Rio Grande do Norte, in the period from 2007 to 2010, described the occurrence of 598 cases of congenital syphilis notification and found flaws in the records of the professionals: information ignored or blank, such as maternal education, partner and prenatal treatment11.
Studies in Ceará13, 14, 18and17in Rio de Janeiro, Brazil also confer that records of cases of syphilis in pregnant women and congenital syphilis are still far below the expected, demonstrating significant weaknesses in the quality of information by a failure in the records.
Gaps in the knowledge of professionals, regarding the management of syphilis in pregnancy, can compromise the effectiveness of prevention and control of congenital syphilis. Special attention to professionals who perform prenatal, offering them the proper training is necessary.
It is extremely important that health professionals correctly carry out quality prenatal consultation of pregnant women with syphilis. Public health policy must establish strategies with healthcare professionals to avoid the transmission of syphilis12.
CONCLUSION
This article has examined and discussed scientific publications related to congenital syphilis and nursing, during the period from 2005 to 2014. It was concluded that the number of nursing publications involving the subject is reduced. Using methods such as the documentation, case studies, literature review, evaluation study of the knowledge and practice. The focus of the articles is focused on pathology, treatment, sequels, differential diagnosis, knowledge, risk factors and social factors.
The limitation of the study is to be selected articles with different methodologies, which prevents the comparison of data and makes the generalization of results.
A limitation of the study is to have selected items with different methodologies, a fact that prevents the comparison of data and makes it impossible to generalize the results. It identifies risk factors that make women vulnerable to syphilis, notes the inadequacy of care lists and difficulties in combating child transmission of syphilis related to the lack of professional training in screening, diagnosis and conducting the treatment of pregnant women with syphilis.
Syphilis in pregnancy and congenital syphilis reached proportions that were contrary to what was proposed by the Ministry of health. The challenge remains for the prevention and control of the disease.
It is suggested that the results brought in this study are faced with the practice of the various units providing prenatal care. The impact of the information provided here can help formulate actions aimed at improving the quality of professional performance.
REFERENCES
1.Geraldes Neto B, Soler ZASG, Braile DM, Daher W. A sífilis no século XVI: o impacto de uma nova doença. Arq Ciência e Saúde. 2009; 16(3): 127-9.
2.Silva FFA. Sífilis e HIV na gestação: uma investigação sobre a assistência pré-natal na rede SUS do município do Rio de Janeiro 2007/2008. [dissertação de mestrado]. Rio de Janeiro: Escola Nacional de Saúde Pública; 2010.
3.Becker MEL. Avaliação da qualidade da assistência pré-natal na atenção primária no município de Rio Branco – Acre. [dissertação de mestrado]. Rio de Janeiro: Escola Nacional de Saúde Pública; 2011.
4.Azulay RD. História da sífilis. Rev Bras Dermatol.1988; 63(1): 3-4.
5.Avelleira JCR, Bottino G. Sífilis: diagnóstico, tratamento e controle. Educação Médica Continuada. Rev Bras Dermatol. 2006; 81(2): 111-26.
6.Ministério da Saúde (Br). Programa Nacional de DST/AIDS/ Hepatites Virais. Boletim Epidemiológico – sífilis 2012. Brasília (DF): Secretaria de Vigilância em Saúde; 2012.
7.Ministério da Saúde (Br). Transmissão vertical do HIV e sífilis: estratégias para redução e eliminação. Brasília (DF): Editora MS; 2014.
8.Souza MT, Silva MD, Carvalho R. Revisão integrativa: o que é e como fazer. Einstein. 2010; 8(1): 102-6.
9.Mendes KDS, Silveira RCCP, Galvão CM. Revisão integrativa: método de pesquisa para a incorporação de evidências na saúde e na enfermagem. Texto contexto – enferm. 2008; 17: 758-64.
10.Botelho LLR, Cunha CCA, Macedo M. O método da revisão integrativa nos estudos organizacionais. Rev eletr Gestão Soc. 2011; 5(11): 121-36.
11.Carvalho IS, Brito RS. A sífilis congênita no Rio Grande do Norte: estudo descritivo do período 2007-2010. Epidemiologia e serviços de saúde. 2014; 23: 287-94.
12.Albuquerque GMA, Chaves EMC, Sampaio LRL, Dias KCF, Patrocínio MCA, Vasconcelos SMM. Complicações da sífilis congênita: uma revisão de literatura. Pediatria Moderna. 2014; 50: 254-8.
13.Mesquita KO, Lima GK, Filgueira AA, Flôr SMC, Freitas CASL, Linhares MSC, et al. Análise dos casos de sífilis congênita em Sobral, Ceará: contribuições para assistência pré-natal. DST - J bras Doenças Sex Transm. 2012; 24(1): 20-7.
14.Costa CC,Freitas LV,Sousa DMN,Oliveira LL,Chagas ACMA,Lopes MVO, et al. Sífilis congênita no Ceará: análise epidemiológica de uma década. Rev esc enferm USP. 2013; 47: 152-9
15.Grossi R, Barros AC, Andrade R, Galvão C, Reis H, Ferreira DC et al. Reação de Jarisch-Herxheimer em gestante com sífilis: relato de caso. DST - J bras Doenças Sex Transm. 2011; 23: 149-51.
16.Follett T, Clarke D. Resurgence of congenital syphilis: diagnosis and treatment. Neonatal Netw. 2011; 30: 320-8.
17.Soares RM, Domingues M, Lauria LM, Saraceni V, Leal MC. Manejo da sífilis na gestação: conhecimentos, práticas e atitudes dos profissionais pré-natalistas da rede SUS do município do Rio de Janeiro. Ciência e saúde coletiva. 2013; 18: 1341-51.
18.Silva DMA, Araújo MAL, Silva RM, Andrade RFV, Moura HJ, Esteves ABB. Knowledge of healthcare professionals regarding the vertical transmission of syphilis in Fortaleza -CE, Brazil. Texto contexto - enferm. 2014; 23: 278-85.
19.Holanda MTCG, Barreto MA, Machado KMM, Pereira RC. Perfil epidemiológico da sífilis congênita no município de Natal, Rio Grande do Norte - 2004 a 2007. Epidemiol Serv Saúde. 2011; 20: 203-12.
20.Domingos AC. Gravidez na adolescência: enfrentamento na estratégia de saúde da família. [trabalho de conclusão de curso]. Belo Horizonte: Universidade Federal de Minas Gerais; 2010.
21.Duarte SJH. Motivos que levam as gestantes a fazerem o pré-natal: um estudo das representações sociais. Cienc Enferm. 2012; 18(2): 75-82.
22.Miranda FJS, Fernandes RAQ. Assistência pré-natal: estudo de três indicadores. Rev enferm UERJ. 2010; 18: 179-84.
23.Peixoto CR, Freitas LV, Teles LMR, Campos FC, Paula PF, Damasceno AKC. O pré-natal na atenção primária: o ponto de partida para reorganização da assistência obstétrica. Rev enferm UERJ. 2011; 19: 286-91.
24.Brandão ICA, Godeiro ALS, Monteiro AI. Assistência de enfermagem no pré-natal e evitabilidade de óbitos neonatais. Rev enferm UERJ. 2012; 20: 596-602.