(*) p-chi-square test with significance level lower than 0.05 (p<0.05)
ORIGINAL RESEARCH
Nursing diagnoses in the coping and stress tolerance domain in patients with AIDS
Laísi Catharina da Silva Barbalho BrazI; Vinicius Lino de Souza NetoII; Iellen Dantas Campos Verdes Rodrigues III; Bárbara Coeli Oliveira da SilvaIV; Romanniny Hévillyn Silva CostaV; Richardson Augusto Rosendo da Silva VI
I
Nurse. Master´s student in Nursing at the Federal University of Rio Grande
do Norte. Natal, RN, Brazil. E-mail: laisicatharina@hotmail.com
II
Nurse. Master in Nursing at the Federal University of Rio Grande do Norte.
Substitute Professor of the Department of Nursing at the Federal University
of Rio Grande do Norte. Natal, RN, Brazil. E-mail: vinolino@hotmail.com
III
Nurse. Ph.D. in Nursing at the Federal University of Rio Grande do Norte.
Professor of the Department of Nursing at the Federal University of
Sergipe. Lagarto, SE, Brazil. E-mail: iellendantas@hotmail.com
IV
Nurse. Master in Nursing at the Federal University of Rio Grande do Norte.
Ph.D. student in Nursing at the Federal University of Rio Grande do Norte.
Substitute Professor of the Department of Nursing at the Federal University
of Rio Grande do Norte. Natal, RN, Brazil. E-mail: barbaracoeli@outlook.com
V
Nurse. Master in Nursing at the Federal University of Rio Grande do Norte.
Nurse of the School Maternity Januário Cicco and the Federal Institute of
Education, Science, and Technology of Rio Grande do Norte. Natal, RN, Brazil. E-mail: romanniny@yahoo.com.br
VI
Nurse. Ph.D. in Health Science by the Federal University of Rio Grande do
Norte. Professor of the Department of Nursing and the Post-Graduation
Program in Nursing at the Federal University of Rio Grande do Norte. Natal,
RN, Brazil. E-mail: rirosendo@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.17040
ABSTRACT
Objective: to examine the associations between nursing diagnoses, related risk factors and defining characteristics of the coping and stress tolerance domain of the North American Nursing Diagnosis Association in patients with Acquired Immunodeficiency Syndrome (AIDS). Method: in this cross-sectional study of 113 AIDS inpatients at Giselda Trigueiro Hospital, in Natal, Rio Grande do Norte, Brazil, data were collected between March and September 2014 by interview and physical examination, and analyzed according to the stages of Marjory Gordon's clinical assessment. The study was approved by the research ethics committee (ethical evaluation submission certificate No. 23008113.8.0000.5537). Results: associations were found among anxiety, fear, and stress; change stress syndrome, anxiety, and decreased health status; fear, reports of apprehension, and sensory damage; and risk of feeling impotent, stigmatized disease and poor knowledge. Conclusion: the study contributed to identifying nursing diagnoses related to the specific characteristics of these patients.
Keywords: Nursing; nursing process; acquired immunodeficiency syndrome.
INTRODUCTION
It is estimated that 1.6 million people live with the Human Immunodeficiency Virus (HIV) in Latin America, with most cases concentrated in Argentina, Brazil, Colombia, Mexico, and Venezuela¹. Considering the accumulated data from 1980 to June 2014, a total of 757,042 cases of Acquired Immunodeficiency Syndrome (AIDS) were reported in Brazil. According to the Department of Sexually Transmitted Diseases (STDs), AIDS and Viral Hepatitis of the Ministry of Health approximately 734,000 people were living with AIDS in the country2.
Since 1996, Brazil has adopted the policy of free and universal access to antiretroviral therapy (ART) for people living with AIDS. As a consequence, the country stands out internationally for the actions of coping and reducing the mortality rate related to this disease².
Currently, AIDS is considered a chronic disease due to the existence of ART, resulting in a longer survival. However, it causes changes in the daily life of people living with AIDS, such as the need for health team follow-up, periodic examinations, daily medication intake and in some cases adverse reactions. Also, it can cause a strong impact related to stigma and prejudice, changes in marital relationships, such as the abandonment of the partner, as well as the difficulty in maintaining and reintegrating into the labor market. Such changes can generate stress and depression for coping with the disease3.
In this context, nursing professionals play an essential role in the implementation of actions aimed at promoting, protecting, preventing, diagnosing, treating and rehabilitating AIDS patients4.
Therefore, the introduction of a systematic process ensures greater quality in care delivery and comprehensive care. Nursing has the Nursing Process (NP) as a methodological tool for systematizing care and documenting professional practice to perform this function. It is divided into 5 steps: data collection; nursing diagnosis; nursing planning; implementation and evaluation5.
In this context, the elaboration of the Nursing Diagnosis (ND) becomes a vital stage, considering the intellectual activity that the nursing professional develops in their daily life to judge the human responses that require nursing interventions. Nurses must use their knowledge, cognitive, interpersonal skills and professional attitudes to determine the content and quality of the results of their use, drawing the clinical reasoning 4.
Also, nursing classification systems can be used in the construction of NDs, with the most widely used in the world being the North American Nursing Diagnosis Association International (NANDA), which classifies nursing diagnoses in domains and classes, constituted by title, with a conceptual definition, defining characteristics and related or risk factors, subdivided into 13 domains6.
As a way of knowing the production on the topic, a search was made in the computerized databases of the Virtual Health Library (VHL): Latin American and Caribbean Literature (LILACS) and International Literature in Health and Biomedical Sciences (MEDLINE); and SCOPUS, Cumulative Index to Nursing and Allied Health Literature (CINAHL). It was observed a range of scientific productions using NANDA for the construction of ND in several areas such as puerperal women, medical clinic, child and adolescent health that addressed several domains. However, there was a shortage of scientific production of ND in patients with AIDS in coping and stress tolerance, justifying the accomplishment of this study so the interventions can be proposed closer to the real needs of the patients.
Based on these considerations, the following question emerged: is there an association between nursing diagnoses, risk-related factors and the defining characteristics of NANDA's stress coping and tolerance domain in AIDS patients? to answer the question of research, the study aimed to analyze the associations between nursing diagnoses, related/risk factors and the defining characteristics of NANDA stress coping and stress tolerance in patients with AIDS.
LITERATURE REVIEW
Acquired immunodeficiency syndrome (AIDS) is a disease of the human immune system caused by the human immunodeficiency virus (HIV). The HIV virus is a retrovirus, classified in the subfamily of Lentiviridae1. The way of contagion is in unprotected sexual intercourse, occupational accidents, sharing of syringes, among others. The virus is tropic by the T-CD4 lymphocytes, altering the cell's DNA leaving individuals susceptible to secondary diseases such as meningitis, oral and esophageal candidiasis, tuberculosis and pneumonia3.
The first AIDS case was recorded in Brazil in 19802. At that time, AIDS was believed to be an exclusive disease of homosexuals and drug users. This fact increased the prejudice against these individuals and contributed to their labeling as groups at risk for AIDS1.
Today, there is an increase in the number of young and heterosexual men infected with the virus7, pointing out the relationship between the vulnerability of this group as the active exposure to risk, due to being more exposed and sensitive to specific situations. The representations by society about male and female sexuality make a significant contribution to the divergence of exposure between the two groups, so men are exposed by a greater propensity to a greater number of partners, alcohol, and other drugs8.
Currently, since the HIV virus does not segregate social groups, ethnicity, and age, Brazil's Ministry of Health (MS) is primed for promotion and prevention, focusing on the reduction of risk behaviors as a strategy for disease control2. Thus, strategies such as the active search for communicators, diagnosis and timely treatment and promotion of healthy practices such as the use of condoms have been successfully adopted by the family health strategy (FHS) for the control of the disease7. Among the tactics of coping with infection and prevention adopted by patients, a similarity is observed with the actions carried out by different social segments, such as the health services and the media.
However, it is worth emphasizing an aspect that alarms the sanitary organs that is the representation of such measures for professionals and individuals. Regarding the use of condoms, the value attributed to it as a means of prevention is highlighted, is considered the gold standard for professionals. However, the obtaining means by the patients, even with free distribution in most health services, still has social impediment factors that inhibit their acquisition, which together with the high market cost for a good part of the population and the price differentiated between the female and the male codon hinder the use and predispose the young to risk 8.
METHODOLOGY
This is a descriptive study, with a quantitative approach, performed at Giselda Trigueiro Hospital, a reference in the treatment of infectious diseases in Natal, Rio Grande do Norte, Brazil. Patients with AIDS who were admitted to the hospital were part of the study. Thus, the average number of hospitalized patients in the period from 2009 to 2013 for the calculation of the sample reached a quantitative of 158 patients with AIDS. From this number, the sample for finite populations was calculated, assigned with a sampling error of 5% and reliability of 95%, summarizing 113 AIDS patients, who were selected for convenience.
The following inclusion criteria were adopted for the selection of patients: having been clinically diagnosed with AIDS, presenting age above 18 years old, and being hospitalized at the time of data collection. The exclusion criteria were to ignore the diagnosis of the disease and not to be in psychic and emotional conditions.
The researchers reported to the nursing team, consulted the medical records, and approached the patient for an evaluation of their general health status, level of awareness and guidance to verify if the patient was aware of the disease and had physical and psychic conditions compromised. Patients were investigated for their temporal and spatial orientation.
Data were collected from March to September 2014, through an interview script and physical examination that included sociodemographic data (age, gender, marital status, and family income), behavioral and clinical, based on NANDA taxonomy II, being applied to the patients who were in the infirmary of the hospital, respecting all their privacy and suitability.
The instrument was submitted to content and appearance validation by ten faculty members who develop studies in the SAE area. All proposed suggestions were incorporated into the instrument. Next, a theoretical and practical training was given to researchers with a 12-hour workload, developed through lectures and dialogues, discussions of clinical cases and manuals from the Brazilian Ministry of Health (MS), with emphasis on approaching patients with AIDS. After the theoretical stage of the course, a practical activity of simulation of physical examination in pairs was carried out to train the researchers and standardize the data collection.
The next stage was the instrument applied as a pre-test to ten AIDS patients, which were included in the study sample since there was no need to modify the instrument.
The analysis of the findings was systematized in two moments: in the first one, a process analysis was carried out simultaneously with the data collection, aiming to identify the defining characteristics and related factors according to NANDA, version 2012-2014. Nursing diagnosis structuring was followed by the steps of the Gordon10 clinical trial. After this stage, the results obtained underwent a process of review in a paired way between the authors, to ensure a consensual judgment with a greater accuracy. Then, a database was built using Microsoft Excel 2009 software, recording all the variables of the research instruments, such as the respective nursing diagnoses, defining characteristics, and related and identified risk factors.
For the inferential analysis, the two statistical tests called Pearson's Chi-square test and Fisher's exact test (expected frequencies smaller than five) were used to verify the statistical association between the nursing diagnosis and its respective defining characteristics, related factors and risk factors (p <0.05). The analysis was based on the reading of the descriptive statistics, as well as on the analysis of the p-value found, with their respective comments. A level of 5% was adopted for statistical significance. The data were presented in tables and discussed according to the relevant literature.
This study complied with the norms of ethics in research involving human beings of national and international scope with a favorable opinion of the Research Ethics Committee of the Federal University of Rio Grande do Norte (UFRN), according to the Opinion nº 508.445/2014 and with Certificate of presentation for ethical appreciation number 23008113.8.0000.5537.
RESULTS AND DISCUSSION
A total of 113 AIDS patients participated in the study, most of them were at least 30 years old and 39 years old, males 82 (72.6%), unmarried individuals 75 (66.4%) with incomplete elementary school 63.7%), family income up to a minimum wage 54 (47.8%), considering the minimum wage value of R$ 722.00 and most of them residing in the interior of the state of Rio Grande do Norte 76 (67.3%).
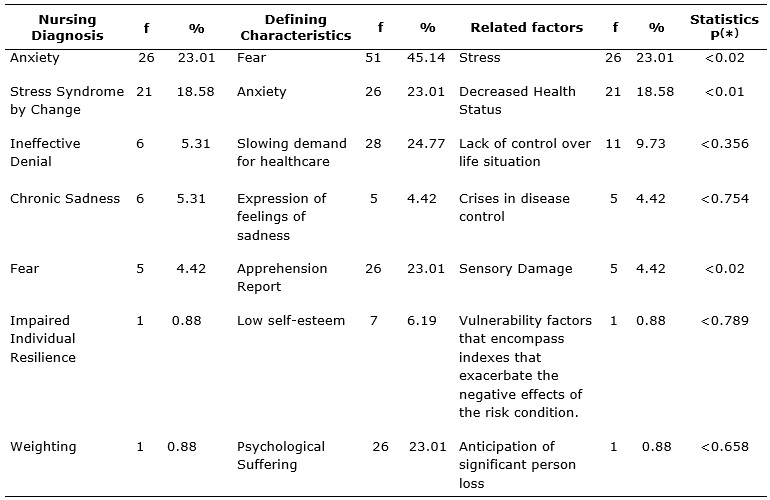
Thus, eight nursing diagnoses were identified. Seven nursing diagnosis was real with the related factors and defining characteristics and one nursing diagnosis was of risk, as explained in Table 1.
Table 1:
Distribution of diagnoses, defining characteristics and related factors of
the Domain Stress and Stress Tolerance for AIDS patients. Natal/RN, Brazil,
2014.
(*)
p-chi-square test with significance level lower than 0.05 (p<0.05)
The results in the table above demonstrated association between the ND anxiety and the defining characteristic (DC) of fear, between the ND anxiety and the related factor (RF) stress; the ND stress-for-change syndrome and DC anxiety, the ND stress-for-change syndrome, and the (RF) diminished health status; the ND fear and the DC report of apprehension, the ND fear and the (RF) sensorial damage.
Table 2 shows the incidence of the diagnosis of the risk of feeling impotent 7 (6.19%), which was associated with factors, stigmatized disease, and poor knowledge.
Table 2:
Distribution of risk factors for diagnosis Risk of the feeling of Impotence
in patients with AIDS. Natal/RN, Brazil, 2014.
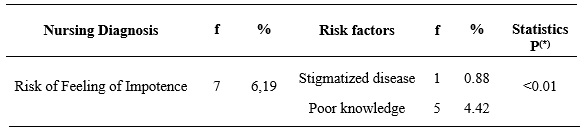
(*)
p-chi-square test with significance level lower than 0.05 (p<0.05)
The results showed an association between the ND risk of feeling impotent and the risk factor (RF) stigmatized disease, between the risk of feeling impotent and the risk factor (RF) poor knowledge.
In view of the results found, discussing the NDs that showed association with their respective defining characteristics and related/risk factors were highlighted, being: anxiety, stress-for-change syndrome, fear and risk of feeling impotent. Statistical significance was set at 5%.
Systematic nursing care for AIDS patients requires a physiological knowledge of the disease and the nurses' perception of the social changes that the illness causes the patients, besides the technical ability.
The ND anxiety presented a higher frequency 26 (23.01%) among the other statements, and it was related to stress and characterized by fear. This is due to the changes that AIDS causes to patients' daily lives, such as frequent hospitalizations due to health status, the use of large amounts of medication, and personal conflicts arising from the diagnosis. Thus, patients experience feelings of apprehension, anxiety, sleep disturbances, substance abuse and fear.
Anxiety is a major predictor of stress and can be conceptualized as a vague and uncomfortable feeling of discomfort or fear accompanied by an autonomic response whose source is usually unknown to the individual but physiologically configured as the excessive release of catecholamines by the pre-nerve endings synaptic and absorbed by cells present in the postsynaptic cleft. Thus, there was a symptomatological picture, such as restlessness, rapid pulse, tachycardia, apprehension, and insecurity 6-11.
Corroborating with the findings, a study carried out in a University Hospital in the State of Minas Gerais pointed out that the diagnosis of anxiety was present in most patients with AIDS presenting a dissociation between the defining characteristics of the study, since the highest prevalence was the apprehension, anxiety, fear, and insomnia, being related to factors of economic situation and change in health status11.
In patients with AIDS, anxiety becomes a common psychological manifestation in all phases of HIV infection, due to changes in health status, uncertainties about the future, changes in therapeutic regimens, changes in results in laboratory tests such as also in personal conflicts 12-14. Therefore, it is the responsibility of the nursing professional to provide a welcoming assistance based on humanized listening, providing moments of exchange of experiences, through integrative and complementary practices.
The ND of stress by changes present in 21 (18.58%) is characterized by a physiological and/or psychosocial disorder resulting from a change from one environment to another, presenting the defining characteristics of anxiety, related to the decreased state of health and others that were not scored in the study as the feeling of impotence that they feel before the disease6.
In this sense, the stress situation triggers a physiological reaction in living beings to external or internal stimuli, threatening the balance of the organism. The responses to stress are mediated by the Autonomic Nervous System (ANS) and the Hypothalamic-Hypophysis-Adrenal (HHA) axis, with complementary actions throughout the organism, aiming to reestablish balance through a complex set of physiological and behavioral responses. These responses range from emergency responses to somatization, psychological distress, and suicide. When stress becomes chronic, other symptoms may be observed as increased adrenal gland function, increasing the risk of infarction, reduced functioning of the thymus and lymph nodes causing damage to the immune system15.
In patients with AIDS, it was supposed that the cause of stress is linked to an abrupt change in lifestyle, together with the fear of death, since the disease, because it has not yet been cured, causes the individual to feel impotent and without expectations of life14.
Coupled with this fear, there is still the issue of living with the side effects of antiretroviral treatment and sometimes feel that it is necessary to hide the disease. This study states that there is a significant relationship of mental disorders with the stigma and discrimination that patients with AIDS suffer, indicating the need for interventions to reduce such situation, such as psychological support not only in outpatient and hospital settings but also in care primary health care16.
This series of psychic and emotional changes work as a source of stress and require a psychological adjustment for both AIDS patients and their families until a better adaptation of the new reality is achieved. This adaptation demands the effort of the individuals and helps from the health professionals, such as the nurses who accompany them to help better manage their expectations, fears, and difficulties14.
Fear is an emotion arising from an objective cause and associated with danger, having a defensive function, as it generates a reaction in the body to the imminent danger. For AIDS patients, fear is a present feeling, generating reactions such as escaping from something bad. Such reactions influence the acceptance of the diagnosis and delay initiation of treatment with antiretrovirals. Despite this, AIDS patients end up having to deal with the harsh reality imposed by the disease, which can lead to mental health problems, such as psychic suffering and suicide ideation in some cases14-17.
Thus, fear ND was present in 5 (4.42%) of the patients studied, characterized by reports of apprehension and related to some sensory damage. In a study carried out with adult patients with AIDS, in the Ambulatory of Infectology of the Federal University of Ceará (UFC), fear diagnosis was also observed among patients, characterized by increased tension and apprehension, and related to the separation of the support in a potentially stressful situation, the findings of the study13.
The daily life of patients with AIDS is permeated by physiological difficulties imposed by the infection, as well as psychosocial factors, particularly depression and lack of social support, being psychologically vulnerable. Maintaining resilience means coping with difficulties and overcoming adversities and potentially traumatic situations. Studies report that well-adjusted patients psychologically tolerate antiretroviral treatment more, have higher adherence rates and report better subjective well-being18-21.
Finally, the risk of feeling helpless was present in 7 (6.19%), presenting as risk factors the poor knowledge of the patient about the disease, and the fact that it is a stigmatized disease. The feelings and conflicts experienced by patients with AIDS, generated after the diagnosis, may be associated with the feeling of impotence since the infection can lead to a feeling of inability to perform their daily activities22-23.
CONCLUSION
The study allowed to identify the association between the ND of anxiety, the DC fear and the RF stress; the ND change stress syndrome, DC anxiety, and the RF decreased health status; the ND fear, the DD report of apprehension, and the RF sensory damage; the risk of feeling impotent, and risk factors, stigmatized disease and poor knowledge. The fact that the study was developed in a certain geographical area and restricted to a single public was among its limitations. However, it is expected that the results of the study contribute to the standardization of the specific nursing language and stimulate other research in the area. Thus, reflections are needed on the nursing care offered to patients with AIDS, because it is believed that the scientific evidence provided by the study allows an improvement both to nursing assistants, as well as to research, extension and teaching areas.
REFERENCES
1.UnAIDS. Fast-Track: ending the AIDS epidemic by 2030. Joint United Nations Programme on AIDS (UNAIDS), Geneva, [Internet] 2014. [cited on January 23, 2016]. Available on: http://www.unAIDS.org.br/biblioteca/JC2686_WAD2014report_en.pdf
2. Ministry of Health (Br), National STD/AIDS Coordination - Epidemiological Surveillance. AIDS Epidemiological Bulletin Year III – nº 1. Brasília (DF); 2014.
3.Braga RMO, Lima TP, Gomes AMT, Oliveira DC, Spindola T, Marques SC. Social representations of HIV/AIDS for people living with the syndrome. Rev enferm UERJ [internet] 2016 [cited on August 18, 2017];24(2):e15123. Available on: http://www.facenf.uerj.br/v24n2/v24n2a05.pdf
4.Faria JO, Silva GA. Nursing diagnoses of the safety and protection domain in patients with AIDS. Rev eletrônica enferm [internet] 2014[cited on August 18, 2017];16(1):93-9. Available on: https://revistas.ufg.br/fen/article/view/19977/0
5.Rivas FJP, García JMS, Arenas CM, Lagos MB, López MG. Implementation and evaluation of the nursing process in Primary Health Care. Int J Nurs Knowl [internet] 2012 [cited on March 15, 2016]; 23(1):18-28. Available on: http://onlinelibrary.wiley.com/doi/10.1111/j.2047-3095.2011.01199.x/pdf
6.Nanda Internacional. NANDA Nursing Diagnostics: Definitions and Classifications 2010-2012. Porto Alegre(RS): Artmed; 2013.
7.Rocha AFB, Araújo MAL, Cavalcante EGF, Moura HJ, Silva APA, Galvão MTG. Positive serology for HIV: an epidemiological study of historical series. Rev enferm UFPE online [internet] 2017 [cited on August 19, 2017]; 11(1):173-8. Available on: https://periodicos.ufpe.br/revistas/revistaenfermagem/article/viewFile/11891/14358
8.Machado YY, Oliveira DC, Nogueira VPF, Gomes AMT. Social representations of health professionals about HIV/AIDS: a structural analysis. Rev enferm UERJ [internet] 2016[cited on August 19, 2017];24(1):e14463. Available on: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/14463
9.Silva RAR, Costa RHS, Nelson ARC, Duarte FHS, Prado NCC, Rodrigues EHF. Predictive factors for the Nursing Diagnoses in people living with Acquired Immune Deficiency Syndrome. Rev Latino-Am Enfermagem [internet] 2016[cited on August 19, 2017];24:e2712. Available on: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-11692016000100342
10.Gordon M. Nursing diagnosis: process and application. 3ª ed. St Louis(MO): Mosby;1994.
11.Faria JO, Silva GA. Nursing diagnoses in patients with AIDS: an approach based on the conceptual model of Horta. Rev RENE [internet] 2013[cited on August 19, 2017]; 14(2): 290-300. Available on: http://www.revistarene.ufc.br/revista/index.php/revista/article/view/821/pdf
12.Bogart LM, Wagner GJ, Galvan FH, Landrine H, Klein DJ, Sticklor LA. Perceived discrimination and mental health symptoms among black men with HIV. Cultur Divers Ethnic Minor Psychol [internet] 2011[cited on June 09, 2016];1:295–302. Available on: http://psycnet.apa.org/buy/2011-15217-009
13.Costa RHS, Nelson ARC, Prado NCC, Rodrigues EHF, Silva RAR. Nursing diagnoses and their components in acquired immune deficiency syndrome patients. Acta Paul Enferm [Internet] 2016[cited on August 21, 2017];29(2):146-53. Available on: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103-21002016000200146
14.Kinyanda E, Hoskins S, Nakku J, Nawaz S, Patel W. The prevalence and characteristics of suicidality in AIDS as seen in an African population in Entebbe district, Uganda. BMC Psychiatry [Internet] 2012 [cited on August 21, 2017];12:63. Available on: https://bmcpsychiatry.biomedcentral.com/articles/10.1186/1471-244X-12-63
15.Tsai AC, Bangsberg DR, Kegeles SM, Katz IT, Haberer JE, Muzoora C et al. Internalized stigma, social distance, and disclosure of HIV seropositivity in rural Uganda. Ann Behav Med [Internet] 2013[cited on August 18, 2017];46:285-94. Available on: https://www.ncbi.nlm.nih.gov/pubmed/23690283
16.Yi S, Chhoun P, Suong S, Thin K, Brody C, Tuot S. AIDS-Related Stigma and Mental Disorders among People Living with HIV: A Cross-Sectional Study in Cambodia. PLoS ONE [Internet] 2015[cited on August 18, 2017];10(3):1-16. Available on: http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0121461
17.Holanda VN, Bezerra AS, Tavares AR, Lima CIR, Mamede LTS, Araújo RLQ, et. al. The biological basis of fear: a systematic review of the literature. Revista Interfaces: Health, Human and Technology [Internet] 2013[cited on August 19, 2017];14(1):1-3. Available on: https://psicologado.com/neuropsicologia/as-bases-biologicas-do-medo-uma-revisao-sistematica-da-literatura
18.Su X, Lau JT, Mak WW, Chen L, Choi KC. Perceived discrimination, social support, and perceived stress among people living with AIDS in China. AIDS Care [Internet] 2013[cited on August 18, 2017];25:239-48. Available on: https://www.ncbi.nlm.nih.gov/pubmed/22835331
19.Peixoto KSM, Silva RAR, Costa RHS. Nursing diagnoses in people with acquired immune deficiency syndrome: an integrative review of the literature. Rev pesqui cuid fundam (Online) [Internet]2015[cited on August 18, 2017];7(1):2123-36. Available on: http://www.seer.unirio.br/index.php/cuidadofundamental/article/view/3410/pdf_1465
20.Grossman CI, Stangl AL. Global action to reduce HIV stigma and discrimination. J int AIDS soc [Internet] 2013 [cited on August 18, 2017]; 16(3 Suppl 2):18881. Available on: doi: https://doi.org/10.7448/ias.16.3.18881
21.Camargo LA, Capitão CG, Filipe EMV. Mental health, family support and treatment adherence associations in the context of HIV/AIDS. Psico USF [Internet] 2014[cited on August 21, 2017]; 19(2):221-32. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1413-82712014000200005
22.Neto VLS, Andrade LL, Agra G, Costa MML, Silva RAR. Profile of nursing diagnosis of hospitalized patients in an infectious disease unit. Rev Gaúcha de Enferm [Internet] 2015 [cited on August 21, 2017];36(3):79-85. Available on: http://www.scielo.br/scielo.php?pid=S1983-14472015000300079&script=sci_abstract
23.Neto VLS, Silva RAR, Silva CC, Negreiros RV, Rocha CCT, Nóbrega MML. Proposal of the nursing care plan in people hospitalized with AIDS. Rev esc enferm USP [Internet] 2017 [cited on August 20, 2017]; 51:e03204. Available on: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0080-62342017000100406