
ORIGINAL RESEARCH
The record of children's growth and development in the health booklet
Abner Pereira de AlmeidaI; Luciana de Carvalho Ceballos II; Alice Regina Costa BarbosaIII; Denismar Alves NogueiraIV; Denis da Silva MoreiraV
I
Nurse. Resident in Neonatal Health. Universidade São Francisco. Bragança
Paulista, São Paulo, Brazil. E-mail: bner.almeida@gmail.com
II
Nurse. Santa Casa de Passos. Passos, Minas Gerais, Brazil. E-mail:
luzinhaceballos@gmail.com
III
Nurse. E-mail: alicelilipipeta@gmail.com
IV
Statistician. Associate Professor of the Institute of Exacta Sciences at
Universidade Federal de Alfenas.Minas Gerais, Brazil. E-mail: denisnog@gmail.com
V
Nurse. Assistant Professor at Nursing School of Universidade Federal de
Alfenas, Minas Gerais, Brazil. E-mail: denisunifal@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2017.16895
ABSTRACT
Objective: to examine the record of children's growth and development in the first year of life, in the health booklet. Methods: in this quantitative, cross-sectional, descriptive study, documentary analysis was carried out with 229 health booklets collected at 10 Municipal Early Childhood Education Centers in a municipality in south Minas Gerais, from January to June 2015, using a purpose-designed form. The study was approved by the research ethics committee (CAAE No. 36321314.6.0000.5142). Results: the rate of data recorded in the booklets was low. Only 3 (1.3%) were fully completed as regards development, and 171 (74.7%) had no child development data entered. Conclusion: the data recorded in the booklets by health personnel on the process of children's growth and development was found to be insufficient. Shortcomings in completion impair communication between health personnel and relatives in comprehensive child care.
Keywords: Nursing; child health; growth and development; comprehensive health care.
INTRODUCTION
The Child Health Booklet (CHB) is an essential tool to monitor the health of children, in which the most significant data and events for the child care follow up are recorded1. This document also enables a dialogue between the multidisciplinary health team, and is recognized as a facilitator between parents and professionals communication2.
The CHB includes the child identification data, obstetric history, birth, the process of growth and development, feeding, the use of iron and vitamin A supplementation, oral, hearing and visual health, vaccines, in addition to the record of clinical complications3.
These records should be made by professionals who are responsible for the child care in health care services. The appropriate management of this instrument must be particularly executed in the maternity hospitals and primary care services; such work represents a challenge for the health team, since much of the information is produced in this places4.
The activities carried out on graduation courses, during the practice of the child health subject, enabled to check that many data in the CHB was not filled. Therefore, this study was performed in view of the importance of the CHB to monitor the process of growth and development in the context of childhood, which provides a health surveillance in this age group that presents a higher risk of mortality2.
The aim of this study was to verify the records of the child's growth and development in health booklets, in the first year of their life.
LITERATURE REVIEW
The primary health care action about the monitoring of growth and development, is the central axis of child care. Surveillance in the prevention of diseases in the context of childhood makes it possible to identify children at greater risk of morbidity and mortality and promote proper control of growth and development of this population group. In Brazil, in recent decades, there is a decrease in infant mortality, touted as one of the millennium goals in the commitment to provide quality of life for this age segment 5-7.
So, in the integral attention to child health, the Ministry of health (MH) proposes 13 lines of care as assistance axes to adapt the operation of the service and the network of children health care5. Almost all actions described in these care lines are included in the CHB and its record enables healthcare professionals and family accompany the child's growth and development process.
The CHB is aimed at every citizen born in the Brazilian territory, and it was established in 2005 to replace the Child's Card, which contained a limited number of information such as identification, weight versus height chart and the child's vaccination card. Since the year 2007 (in its third version), the CHB was incremented with guidelines for health promotion and disease prevention and aggravations3-5,8.
To fulfil its role as an instrument of communication, surveillance, education and child health promotion, there must be a dialogue with the family about these records to fill the CHB completely and correctly. The proper use of this instrument by health professionals enables the family to value it, and makes the CHB a relevant document that guides medical appointments and care actions8.
At the same time, the quality of the CHB information can reveal the condition of the service provided to the children4. The family receives the booklet soon after the child's birth in the maternity ward, and, therefore, must always carry it when using the health care service5.
In this regard, health professionals are responsible of the proper management of this instrument as a resource that promotes dialogue with the family and contributes to the decrease of the morbidity and mortality rates in the first year of life.
METHODOLOGY
This is a study of quantitative, descriptive, transversal methodological approach and documentary analysis9, held in 10 Municipal Child Education Centers (MCEC) in the city of Alfenas-MG. Data were collected in February 2015. The sample of 229 children was calculated considering an acceptable error of ± 5.97 percentage points and a confidence interval of 95% (CI95%) on a population of 1503 child enrolled in 10 MCEC. After the sample calculation, data collection was distributed in 10 MCEC, respecting the percentage of the sample and the number of children enrolled in each educational institution.
In the CHB, we evaluated the data relating to the first-year records, taking into consideration that for monitoring the process of growth and development, the Ministry of health recommends seven medical consultations in the first year of life3. We considered as exclusion criteria, the CHB that were not brought to the MCEC by parents/guardians, after three requirements.
The researchers developed an instrument that served as a basis to verify whether the CHB was filled, contemplating the variables of the study: anthropometric variables (cephalic perimeter x age, weight x age, height x age, BMI x age) and behavioral variables about development (posture, movements, reactions, communication).
The study authors attended the MCEC to request authorization to carry out the research. After, each parent or guardian of children enrolled in the respective MCEC received an invitation, explaining the goals of the study. Those who agreed to participate in the research brought the CHB for data collection. They were arranged in a Microsoft Excel® 2013 spreadsheet and analyzed by statistical program Statistical Package for the Social Sciences (SSPS20).
We complied with the ethical and legal principles in research with humans, according to the resolution No. 466/1210. The data collection occurred with the signature of an informed consent by the parents/guardians, allowing access to CHB. The research project has been approved by the Research Ethics Committee (CEP) at the Federal University of Alfenas (UNIFAL -MG) under the opinion number 869,480.
RESULTS AND DISCUSSION
Growth is a dynamic and continuous process expressed by the increase in body size. It is considered one of the best indicators of the child health, it suffers direct influence of intrinsic (genetic) and extrinsic (environmental) factors as well as food, health, hygiene, housing and sanitation conditions, and the general care of the child1. The data relating to child growth curves - cephalic perimeter x age; weight x age; height x age; body mass index (BMI) x age - are presented in Table 1.
Table 1: Record distribution of anthropometric variables in the Child Health
Booklet. City of the South of Minas Gerais, 2015. (N=229)
Growth monitoring aims to the promotion and protection of the child to prevent deviations of growth could endanger the child current health and future quality of life11. The best method of child growth monitoring is the periodic record of weight, height and BMI of the child in the CHB12.
During data analysis, we observed that in relation to the record of the cephalic perimeter x age, 53 (23.1%) CHB were not filled at all; 44 (19.2%) CHB do not reveal any weight x age data; and for height x age chart, 53 (23.1%) CHB did not have a single record in the childcare consultation months recommended by the MH.
A study carried out in Belo Horizonte with children followed up at the unified health system (SUS), found the CHB filling unsatisfactory, because only 15.5% and 59.4% of children had their cephalic perimeter measured and weight x age registered respectively4.
The cephalic perimeter assessment should be undertaken as a priority in the first year of life, being a measure that offers slight variation for any age group, among gender, ethnic and population groups13.
Weight and height assessment should be periodic since weight gain allows the assessment of individual progress to check higher risk of morbidity and mortality, signaling early a frame of malnutrition or overweight/obesity, clinical pictures that significantly influence the child height development1.
We point out that data of BMI x age were less registered in CHB, in comparison with the others. The inclusion of the IMC as an evaluation parameter enables better monitoring of children in relative weight x length (under 2 years) or weight x height (over 2 years). Such parameter helps professionals identify children who were malnourished in a given period and had their height development jeopardized, as well as children with overweight and short height. In comparison, the weight x age and length x age charts, separately, only show whether the child has, individually, their weight and/or length jeopardized1.
In the CHB there is a reference to fill in the IMC, a table to perform the cross between length/height and weight. The value found at the intersection of the data reflects the value of BMI. However, in practical use, these tables require considerable time to be completed, which can explain why little professionals do it.
We can observe that in the cephalic perimeter x age data, there is an important decrease at 12 months of age - 28 (12.2%), and in the weight x age - 37 (16.0%) and length x age - 39 (17.0%), as Table 1. The older the child, the less completed the chart. This clearly harms the follow up of these children growth process.
A study conducted by the World Health Organization between 1998 and 2002, involving 178 countries, showed that in 80% of them, health workers reported difficulties using the instruments for monitoring children's growth. Problems of conceptual and operational nature were evident, varying from understanding the growth curves to the lack of adequate facilities to measure child growth14.
Aiming at a more appropriate an effective CHB completion, the health professional may use, as a strategy to follow up the child process of growth and development, the time when the children are being vaccinated. Comparing the child's vaccination calendar dates and childcare medical consultations advocated by the Ministry of health, they are similar.
Monitoring the infant population growth can provide feedback to health professionals about interventions or programs implemented in relation to the process of growth in child care. However, for a proper intervention, it is necessary to count with correct anthropometric measurements, appropriate records, regular consultations, trained professionals and maternal education in health actions6.
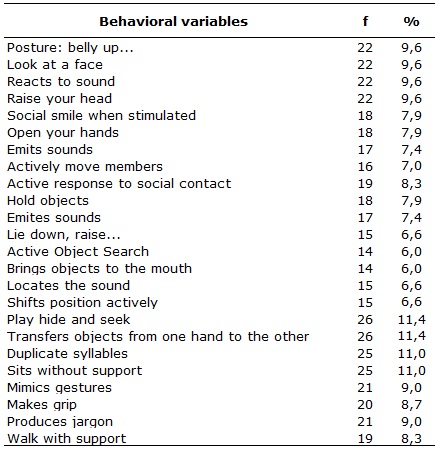
The data in this study, on the evaluation of the process of child development in CHB, demonstrate its completion is precarious. None of the development landmarks were more than 12%, filled as presented in Table 2. Only 3 (1.3%) CHB had a complete fill of the data, and 171 (74.7%) CHB had that variable filled at all.
Table 2:
Record distribution of behavioral milestones of child development in the
Child Health Booklet. City of the south of Minas Gerais, 2015. (N=229)
The process of child development is one of the axes of care for health promotion, and it is based in the childhood period. So, a suitable development depends on care given in early childhood by the family, such as nutrition, stimulation, attention among others, oriented by professionals of health15.
The development is characterized as a global and dynamic process of changes that occur in a person, since their conception, influenced by several physical factors, among them, the care of feeding, hygiene and the prevention of diseases, in addition to the psychological dimension, related to the way a child learns and interacts with the environment in which they live16,17.
As much as the grow, it is imperative to monitor the maturity, psychomotor, social and psyco- affective development of every child, and the professionals should take profit of the pediatric consultation to observe the development and check the parents/guardians relationship with the child. The landmarks serve to dialogue with the family, orienting them to the necessary care for the prevention of diseases and, if in case, forward the child to a specialized service13.
The family plays a role of mediator between the child and society, enabling their socialization, an essential element for the children's cognitive development. The child's interaction with the adult is one of the main elements for an appropriate stimulation in the family space, it contributes to the child perception development, to drive and control their behavior. In addition, it allows them to acquire knowledge and skills, establishing relationships and building their own physical and social environment18.
Therefore, health professionals should be alert to child development milestones, relating to family interaction, to understand the environment in which the child is inserted and, consequently, elaborate intervention strategies, if necessary, so that the child receives integral care.
With regard to primary health care, we note the lack of instruments as well as methodological plans to monitor the child development appropriatley19. Simple and systematized strategies may constitute an important means for the monitoring of child development, providing early identification of deviations in the development milestones, and consequently, the implementation of preventive interventions by health professionals and family20.
The CHB covers activities of promotion and early detection of problems related to child development, contributing to the care through prevention. Thus, increasing the use of this instrument, it is possible to improve the child health integral attention, concerning the monitoring of the development during childhood21.
The daily monitoring of the growth and development process starts with the first puerperium appointment, which evaluates the condition of the mother, along with neonate and pervades the other childcare consultations, scheduled in accordance with the periods recommended by the Ministry of health or according to the needs of the child health care22.
In this perspective, the CHB should be valued as a document that collects and produces information about child health. It is an important instrument for monitoring the child state of health, therefore should be used throughout the use of health services, even on the public or private network15.
CONCLUSION
This study revealed the inadequacy of records on up to one-year old child process of growth and development, performed by health professionals in the CHB. These failures harm communication between professional and families on the integral attention to the child health.
We highlight the responsibility of the professionals in maternity hospitals and primary health care services in the proper management of the CHB, because this instrument must provide correct and complete data for monitoring the process of growth and development in childhood. It is necessary to carry out clear guidelines for mothers to become more involved in bringing the CHB to the medical consultations.
Permanent investments are required in training, so that health professionals can use the CHB, not only as a mandatory instrument, but as a tool that contributes to the improvement of the quality control of the assistance to children.
This study contributed to think on the reality of the data records gathered in CHB, by health professionals, showing the importance of this document for monitoring the growth and development of the child. Nursing professionals must observe the proper completion of this instrument during the childcare consultation, ensuring reliable records, which will serve as parameters for the health monitoring of the infant population, especially for groups with greater social vulnerability.
The limitation of study was that data was collected in documents at a MCEC in only one city in southern Minas Gerais, providing no generalizations. Novel studies on the subject and considering the vision of health professionals and families about CHB and other explanatory variables will be extremely relevant to a greater understanding of the purpose of the instrument.
REFERENCES
1. Ministry of health (BR). Secretariat for health care. Child health: growth and development. Cadernos de Atenção Básica n° 33. Brasília(DF): Editora MS; 2012.
2.Demott K, Bick D, Norman R, Ritchie G, Turnbull N, Adams C, et al. Clinical guidelines and evidence: review for post natal care: routine post natal care of recently delivered women and their babies. London (UK): National Collaborating Center For Primary Care And Royal College of General Practitioners; 2006 [cited in 2016 Nov 12]; Available from: http://www.nice.org.uk/guidance/index.jsp?action=download&o=30146
3. Ministry of health. Child health booklet.9ª ed. Brasília(DF): Editora MS; 2014.
4.Alves CRL, Lasmar LMLBF, Goulart LMHF, Alvim CG, Maciel GVR, Viana MRA, et al. The quality of Child Health Booklet and associated factors. Cad Saúde Pública. 2009; 25(3):583-95.
5. Brazil. Ministry of health (Br); Secretariat for health care. Schedule of commitments to the integral health of children and reducing child mortality. Brasília(DF): Editora MS; 2004.
6.Carvalho MF, Lira PIC, Romani SAM, Santos IS, Veras AACA, Batista FM. Growth monitoring in children under one year: situation in health services in the State of Pernambuco, Brasil. Cad Saúde Pública. 2008; 24(3):675-85.
7.Rocha R, Oliveira C, Silva DKF, Bonfim C. Neonatal mortality and prevention: an analysis of the epidemiological profile. Rev enferm UERJ.2011; 19(1):114-20.
8.Goulart LMHF, Alves CRL, Viana ARM, Moulin ZS, Carmo GAA, Costa JGD, et. al. Child health booklet: assessment on pregnancy, childbirth and newborn data. Rev Paul Pediatria.2008; 26(2):106-12.
9.Polit D, Hungler B. Fundamentals of nursing research: evaluation of evidence for nursing practice.7º ed. Porto Alegre(RS): Artmed; 2011.
10. National Health Council (BR). Opinion nº 466, of December 12th 2012. Guidelines and regulatory norms for research involving humans. Brasília(DF); CNS; 2012.
11.Araújo CLP, Hallal PC, Nader GA, Menezes AMB, Victora CG. Size at birth and height in early adolescence: a prospective birth cohort study. Cad Saúde Pública [Internet]. 2008 [cited 2017 Oct 13] ; 24( 4 ): 871-8. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0102-311X2008000400018&lng=en . http://dx.doi.org/10.1590/S0102-311X2008000400018
12.Barros Fernando C, Victora CG. Maternal-child health in Pelotas, Rio Grande do Sul State, Brazil: major conclusions from comparisons of the 1982, 1993, and 2004 birth cohorts. Cad Saúde Pública [Internet]. 2008 [cited 2017 Oct 01] ; 24( suppl 3 ): s461-s467. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0102-311X2008001500012&lng=en . http://dx.doi.org/10.1590/S0102-311X2008001500012
13. Ministry of health (Br). Secretariat for health care. Manual for use of the child's health booklet. Brasília (DF): Editora MS; 2005.
14.De Onis M, Wijnhoven TM, Onyango AW. Worldwide practices in child growth monitoring. J Pediatr.2004; 144:461-5.
15.Gaíva MAM, Blanco da Silva F. Child health booklet: integrative review. Rev enferm UFPE on line. 2014; 8(3):742-9.
16.Saparolli ECL, Adami NP. Evaluation of the quality of the nursing consultation to the child in the family health program.Acta Paul Enferm. 2007; 20(1): 55-61.
17.Coelho VAC, Tolocka RE, Marco A. Motor habilities assessment and physical growth of preschoolers. Saúde em Rev. 2006; 20(8): 7-14.
18.Andrade SA, Santos DN, Bastos AC, Pedromônico MRM, Filho NA, Barreto ML. Family environment and child cognitive development: an epidemiological approach. Rev Saúde Publica. 2005; 39(4): 606-11.
19.Vasconcelos EN, Silveira MFA, Eulálio MC, Medeiros PFV. The standardization of child under one year old care: study of the meanings assigned by the professionals of the family health program (PSF). Ciênc Saúde Coletiva. 2009;14(4):1225-34.
20.Reichert APS, Vasconcelos MGL, Eickmann SH, Lima MC. Assessment of the implementation of an educational intervention on developmental surveillance with nurses. Rev esc enferm USP. 2012;46(5):1049-56.
21.Andrade GN, Rezende TMRL, Madeira AMF. Child health booklet: experiences of professionals in primary health care.Rev esc enferm. 2014; 48(5):857-64.
22.Ribeiro SP, Oliveira DS, Fernandes SLSA, Felzemburgh RDM, Camargo CL. The everyday life of nurses in childcare consultation. Rev enferm UERJ 2014; 22(1):89-95.