RESEARCH ARTICLES
Nursing guidance and its influence on surgical hospital patients' anxiety levels
Thays Macedo Nascimento CostaI; Carlos Eduardo Peres SampaioII
INurse, graduate from the Graduate School of Nursing at the State University of Rio de Janeiro, Brazil, Email: thaymacedo1505@hotmail.com
IINurse, PhD. Associate Professor of Medical-Surgical in the Nursing Department at the State University of Rio de Janeiro, Advisor of the researchimpact of nursing guidelines in the anxiety level of surgical patients, Rio de Janeiro, Brazil. Email: carlosedusampa@ig.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2015.16534
ABSTRACT
This quantitative, descriptive study to identify trait and state anxiety in hospital patients undergoing general surgery, and describe the influence of nursing guidance on surgical patients' anxiety levels, was carried out using structured interviews at a hospital surgical department in the municipality of Rio de Janeiro, between July 2012 and January 2013,. The study comprised 50 patients, aged from 20 to 70 years. Analysis of the results revealed that levels of trait and state anxiety increased in patients who received no nursing guidance. It was concluded that preoperative nursing guidance is of fundamental importance to both the client and the whole team participating in this event, by fostering well-being and reducing anxiety during surgery.
Keyword: Nursing guidance; trait; state; anxiety.
INTRODUCTION
When any bodily function is not functioning correctly, it can be defined as an illness1. This process occurs when these functions are weakened, and the human body starts to respond negatively, with the presence of some symptoms, such as tiredness, headache and increased blood pressure.
Disease can lead to hospitalization and this event involves a great capacity for adaptation of the individual to the various changes that occur in everyday life; the patient goes through the motions of aggravating the feelings of isolation and distress, such as fear, pre-existing tensions and concern about hospitalization, which implies a series of feelings of discomfort. This process provides depersonalization, this occurs when the patient is hospitalized long time, for example, in a surgical procedure, passing therefore to be treated according to the context of their symptoms, rather than as individual 2.
The waiting time for performing a surgical procedure in hospitalized patients may be the cause of high stress and anxiety. These sensations are directly related to the issue so much mind the invasive procedure on the uncertainty of the diagnostic result 3. In this context of waiting and anxiety, the families are also closely involved and sharing with the patient their feelings and uncertainties, making the management of this situation even more complex for the nursing staff, since these moments are witnessed by them.
Faced with this problem, the monitoring of surgical patients in the preoperative period by nursing staff is relevant, this is when the client is waiting for the surgery and needs guidance as to the procedure, risks of possible complications in the postoperative period. Thus, the following research question arises: Do nursing guidelines influence the level of anxiety in surgical patients?
The nurse is of great importance, since they assist surgical patients, prioritizes not only the physical factors, but the psychological aspects as well. When starting the preoperative period with surgical marking, the patient experiences worries and fears related to the surgical procedure, therefore the psycho-emotional support is essential, which is offered by the nurse through the guidelines and preoperative care4.
The reason for the interest of this theme emerged from the Scientific Initiation Project of the State University of Rio de Janeiro entitled: Impact of nursing guidelines in the anxiety level of surgical patients. The academic experience in practical scenarios possible to observe that most patients increases their level of anxiety due to waiting for surgery.
From this perspective, the research is relevant to study the anxiety of surgical patients and the health problems that high anxiety levels cause the body as well as emotional, psychological and social aspects. Increased anxiety may occur due to surgical suspensions, which shows the negative side, causing much harm to the patient, increasing their level of anxiety, shaking their psycho-emotional, which affects the result of care and productivity services, implying operating and financial costs and detrimental to the institution4.
Thus, the following was established as this study's objective: Identify the trait and state anxiety of hospital patients undergoing general surgery and describe the influence of nursing orientations on anxiety levels of the surgical patient.
LITERATURE REVIEW
The pre-operative nursing care is divided into mediate and immediate preoperative. The mediate preoperative comprises the period from the time of surgery dial up to 24 hours before the procedure at that time are performed anamnesis, physical, nutritional, laboratory tests, imaging studies, physical and emotional preparation and nursing guidelines aimed at preventing complications in the postoperative period. Such guidelines include: breathing exercises of coughing and deep breathing; lower limb exercises that prevent deep vein thrombosis; guides the use of compressive stocking until hospital discharge; and other guidelines that depend on the history and physical examination data raised, such as smoking, obesity, cold sores, changes in exams5.
From the immediate preoperative, it is understood that from the eve of surgery until the arrival of the client to the operating room the nurse plans and evaluates the physical state and advises the patient to remove the clothes, put the hospital gown and cap the hospital; provides orientation on fasting, emptying of the bladder, personal , hair and oral hygiene, and the removal of dentures. These guidelines help to let the patient closer than will be held at the time of surgical, thus reducing high levels of anxiety5.
In addition to physical preparation, the nurse's role is to work the patient's emotional providing more direct assistance actions in this patient in the preoperative period. With this, they began using the preoperative visit by nursing as a strategy, which makes it possible to perceive the State of apprehension of apprehension and family facing the surgery, clarifying any doubts and helping to detect problems. This aims to reduce the client's anxiety and their families in relation to the anesthetic-surgical procedure6.
Nurses have a comprehensive view of basic human needs of the patient, favoring the care of both the patient and the family. For this care, the nurse needs a differential look, in a holistic manner, to carry out their activities in a systematic way, as the patient remains hospitalized for some time, which leaves them far from their relatives and friends7.
Anxiety is a phenomenon that sometimes benefits, sometimes harms the human being this feeling can stimulate the individual into action state in excess does the opposite, it prevents reactions that paralyze people, who fail to do simple things on the daily basis because of the discomfort they feel. These events can be generated because of the anxiety disorders that can appear in the form of concerns, tension, fear, feeling that something bad is going to happen and lack of control over their thoughts. Such reactions can be measured through the use of state and trait anxiety scales; these scales contribute to outline the levels of anxiety of the surgical patient8.
The trait anxiety scale describes how the individual usually feels. Since the state scale measures as the individual feels that given moment and in the past.
The State of anxiety is an emotional reaction characterized by transient feelings of tension, apprehension, nervousness, anxiety and restlessness, which contributes to the change of heart rate, blood pressure, breathing pattern, tremors and sweating. Since the anxiety trait is the individual behavior that remains latent, until in a given situation, whether by stress or anxiety, are activated, leading the individual to react in a certain way9.
If the individual interpreting an internal or external stimulus as threatening, he will develop state of anxiety, characterized by feelings of tension and apprehension, stimulating the autonomic nervous system. Thus, the guidelines made by the nurse at that time, are important to clarify possible doubts and minimize patient anxiety10.
It is important for nurses to perform the focused guidance to the patient, taking care to answer the questions according to the level of information and patient understanding, because excess details can confuse them increase their level of anxiety. The information compiled by the nurse must be clear and simple so as not to leave the patient confused and more anxious11,12.
Nurses should be prepared with information not only technical and scientific, but humanistic and holistic manner, since often the guidelines go beyond the technical and scientific barriers, helping that patient to find effective coping mechanisms for experienced time11.
METHODOLOGY
This is a descriptive quasi-experimental study with a quantitative approach. This type of research aims to describe and summarize the right group data without interference or draw any conclusions on the larger group13.
In the quantitative study, the researcher collects and interprets information from reality, valuing the phenomenon in its different variables14.
Was also carried out a comparative study between patients divided into two groups, those who received the preoperative nursing orientation and those who did not receive it.
The research field chosen for the data collection covered the wards of the surgical clinic of a university hospital in the city of Rio de Janeiro, which provides services for various medical specialties and develops research and extension actions. The study took place in the period July of 2012 to January 2013. The population studied was composed of patients undergoing general surgery at the hospital studied; the sample consisted of 50 patients. The inclusion criteria were being in the preoperative period for performing general surgery, over 18 years of age; being alert and oriented. Pediatric surgery patients were excluded from this study.
As an instrument, we used a form with open questions to characterize the patient, type of surgery and age. Data collection was performed using a structured script - Inventory trait and state anxiety (STAI) Spielberg, Gorsuch and Lushene - composed of two different scales designed to measure the two concepts of anxiety, or anxious state (STAI-State) and trait anxiety (STAI-Trait). Each scale consists of 20 statements for which volunteers indicate the intensity of the moment (STAI-State) or the frequency with which they occur (STAI-Trait)9, 15,16.
The scale contains answers to questions posed Likert, which are none, a little, very much and totally. Based on them, scores of 1 to 4 are assigned to responses. For the cutoff point in defining the degree of anxiety, the 25 and 75 percentiles were used. The 25 percentile or below is considered low anxiety. Between 25 and 75 is considered moderate anxiety and 75 percentile or above is considered high anxiety15. The STAI was the result of successive empirical findings that have established two types of anxiety: state anxiety and trait anxiety 16.
Anonymity was assured to the participants, as well as the complete freedom of response, they may discontinue their participation at any time, without prejudice to them. The survey was conducted in accordance with the guidelines of the National Health Council of the Ministry of health17, having been authorized by the Committee of ethics in research the Pedro Ernesto University Hospital of the State of Rio de Janeiro (CEP/HUPE/UERJ), with opinion No. 3014/2011.
The data were analyzed and interpreted with the use of simple descriptive statistics, understanding that statistical procedures empower the researcher to reduce, summarize, organize, evaluate, interpret, and communicate numeric information18.
The presentation of results was through tables and figure, having been applied absolute and percentage frequency calculations. The tables were constructed from the total of patients to obtain the mean and standard deviation of trait and state anxiety of hospitalized surgical patients.
RESULTS AND DISCUSSION
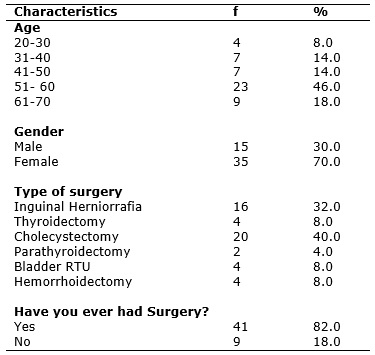
The subjects consisted of 50 patients, 15 (30%) were male and 35 (70%) were female. The ages ranged from 20 to 70 years. Regarding previous surgical experience, 41 (82%) patients had undergone surgery previously and 9 (18%), never. See table 1.
TABLE 1:
Profile of patients undergoing general surgery.Rio de Janeiro, 2013 (N=50).
The most frequent age group identified in the study was 51-60 years - 23 (46%), confirming the results of other studies, which demonstrate that this population is more likely to undergo a surgical procedure10.
One can identify the most common surgical procedure was cholecystectomy - 20 (40%), followed by the inguinal herniorrafia - 16 (32%). Regarding previous surgeries, most of the respondents had already previously undergone surgery.
Previous experience of an anesthetic and surgical procedure and all its implications are seen, therefore, as a first exposure to the stressor, which may influence the coping strategies of other surgeries given the levels of complexity.
These strategies are used to reduce the internal and external demands, helping to minimize feelings of apprehension and loneliness is located away from family and work, and to be admitted to a hospital and undergo a surgical procedure that often the patient is unaware of20.
All these feelings contribute to increased levels of anxiety. The determination of trait and state of patients was performed with two groups, patients receiving nursing guidelines and those not receiving nursing guidelines. Precisely in order to know the intrinsic levels of anxiety (trait of anxiety) and anxiety levels face a stressful situation with surgery (state of anxiety).
While comparing the trait and state anxiety we identified anxiety levels and investigated the possible contributions of the nursing guidelines.
According to the results, it was observed that the patients were oriented trait anxiety equal to the average state of anxiety and 36.2 average 35.6 maintaining the same near these levels (balance). While patients non-oriented showed trait state equal to an average of 36.6 and anxiety, state equal to an average of 44.6. non-oriented patients showed the mean difference between trait and state increased by +8 in their levels of anxiety, since the oriented had a difference of reduced anxiety average +0.6, as shown in Table 1. Through these data, it can be seen that patients who received preoperative guidelines were less anxious when comparing the trait rates and state of anxiety of non-oriented patients
TABLE 2:
Average distribution by state and trait of patients undergoing general hospital surgery. Rio de Janeiro, 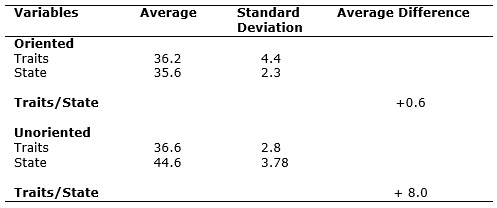
The feelings of anxiety can be developed in the preoperative period, leaving the patient emotionally shaken, contributing to their vulnerability and dependence. Many patients have high stress level, independent of the degree of complexity of the surgery, which can have a relationship with the misinformation of the surgical procedures, anesthesia and preoperative care21.
The anxiety level of patients during surgery proved to be high when not receiving nursing guidelines, highlighting the importance of the nursing role at that time. In turn, anxiety has different levels: low, medium and high according to Spielberg, Gorsuch and Lushene Scale9, 15,16. Thus, we began to investigate the profile of the anxiety levels of oriented and non-oriented patients.
It was observed that the trace levels and the state of anxiety of patients oriented remained low, with their percentage in trait anxiety: low (73.3%); Average (26.7%); high (0%) and state of anxiety levels were low (88.7%); Average (13.3%); high (0%), showing an increase of low levels of anxiety status of oriented patients when compared with the trait anxiety. While the trait anxiety levels and state of non-oriented patients presented very significant variations: anxiety traits achieved results - low (33.4%); Average (66.6%); high (0%) - and anxiety states - low (6.6%); Average (73.3%); high (20%) - an increase of average and high levels of anxiety.
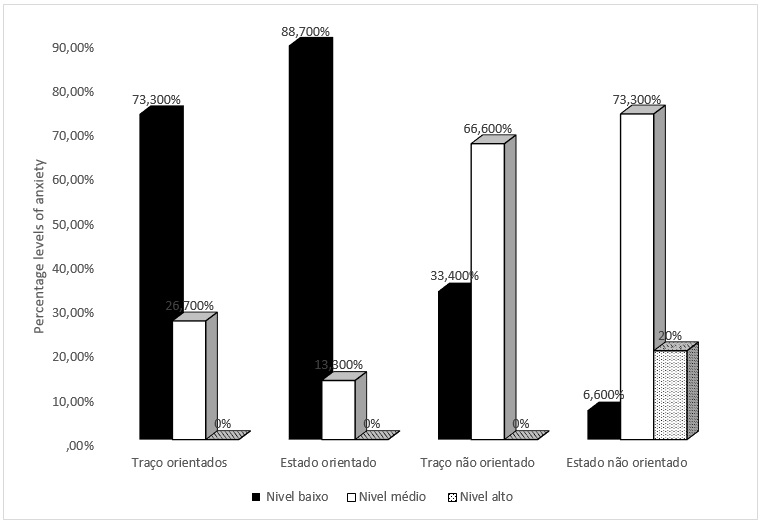
FIGURE 1:
Percentage of patients undergoing general hospital surgery and oriented and non-oriented, according to their level of anxiety. Rio de Janeiro, Brazil 2013.
These results further reinforce the relevance of nursing guidelines for surgical patients, for those who receive guidance remain very similar anxiety levels, while non-oriented patients increase their levels of anxiety, as shown in Figure 1. The results show that patients do not experience a difference in the oriented anxiety profile when compared between trait and state anxiety. The medium and high levels of anxiety of unoriented patients had a significant increase.
Nursing guidelines assist in clarifying the doubts that the surgical procedure causes, reduce the duration of hospitalization, increase satisfaction with the service provided and minimize postoperative complications21.
These guidelines can be performed by nurses, in surgical clinical units and surgical centers, and should be held individually to meet the needs of each patient; is necessary to value the preoperative nursing visit with the surgical patient, establishing a dialogue based on therapeutic listening, giving the patient a calm and peaceful environment to clarify their doubts21.
Among the limitations of the study, include the small sample size and a unique setting that prevent generalization of the results.
CONCLUSION
The study presented contributions in order to facilitate the perioperative nursing care, contributing to the knowledge of nursing and to elaborate on changes in care, since it was possible to identify how much anxiety can influence the patient's well-being.
The high level of anxiety may jeopardize the success of the surgery, since it generates bad feelings, shaking the client. In the study, it was identified that patients unoriented by the nursing staff significantly increase their levels of anxiety, revealing the emotional upset, which may contribute to possible complications in the postoperative period.
It is concluded that, in order to overcome such shortcomings, strategies should be established to provide guidelines for preoperative nursing because they have fundamental importance both for the surgical patient as to the entire team that participates in this moment, with views to the well-being and the reduction of the anxiety and surgical risks.
REFERENCES
1.Figuera J, Viero VE. Vivências do paciente com relação ao procedimento cirúrgico: fantasias e sentimentos mais presentes. Rev SBPH. 2005; 8: 51-63.
2.Costa VASF, Silva SCFS, Lima VCP.O pré-operatório e a ansiedade do paciente: a aliança entre o enfermeiro e o psicólogo. Rev SBPH. 2010; 8: 77-85.
3.Grazziano ES, Bianchi ERF. Nível de ansiedade de clientes submetidos a ngiocoronariografia e de seus acompanhantes. Rev Latino-Am Enfermagem. 2004; 12: 168-74.
4.Sampaio CEP, Ribeiro DA. Perfil cirúrgico e fatores determinantes das suspensões de cirurgias gerais ambulatoriais: contribuições para assistência de enfermagem. Revista de Pesquisa: Cuidado é Fundamental, online 2012; 4: 2938-47. [citado em 9 jul 2014] Disponível em: http://www.seer.unirio.br/index.php/cuidadofundamental
5.Barreto RASS, Araújo ACO, Suzuki K, Freitas VC. A necessidade de informação do cliente em pré-operatório de colecistectomia. Rev Min Enferm. 2010; 14: 369-75.
6.Ministério da Saúde (Br). Manual de Normas e Rotinas e Centro Cirúrgico Central de Material de Esterilização. Lavras (MG): Ministério da Saúde; 2007.
7.Almeida CEE, Nokibara MP, Ribeiro DA, Sampaio CEP. O cuidado de enfermagem associado à prescrição de enfermagem numa unidade de cirurgia cardíaca. Revista de Pesquisa: O Cuidado é Fundamental, online 2012; 3: 2510-20. [citado em 10 jul 2014] Disponível em: http://www.seer.unirio.br/index.php/cuidadofundamental
8.Ministério da Saúde (Br). Biblioteca Virtual em Saúde do Ministério da Saúde. Ansiedade. São Paulo: BVS 2011. [citado em 10 jul 2014] Disponível em: http://bvsms.saude.gov.br/bvs/dicas../224_ansiedade.html
9.Peniche ACG, Jouclas VMG, Chaves EC. A influência da ansiedade na resposta do paciente no período pós-operatório. Rev esc enferm USP. 1999; 33: 391-403.
10.Peniche ACG. Ansiedade e o paciente cirúrgico: análise das variáveis intervenientes [tese de doutorado]. São Paulo: Universidade de São Paulo; 2005.
11.Baggio MA, Teixeira A, Portella MR. Pré-operatório do paciente cirúrgico cardíaco: a orientação de enfermagem fazendo a diferença. Rev Gaúcha Enfem. 2001; 22: 122-39.
12.Grittem L, Méier MJ, Gaievicz AP. Visita préoperatoria de enfermagem: percepções dos enfermeiros de um hospital de ensino. Cogitare Enferm. 2006; 11: 245-51.
13.Lobiondo-Wood G, Haber J. Pesquisa em enfermagem: métodos, avaliação críticas e utilização. 4a ed. Rio de Janeiro: Guanabara Koogan; 2001.
14.Polit DF, Beck CT, Hungler BP. Fundamentos de pesquisa em enfermagem, métodos, avaliação e pesquisa. 5ª ed. Porto Alegre (RS): Artes Médicas; 2004.
15.Frias TFP, Costa CMA, Sampaio CEP. O impacto da visita pré-operatória de enfermagem no nível de ansiedade dos pacientes cirúrgicos. Rev Min Enferm. 2010; 13:76-83.
16.Fioravanti ACM. Propriedades psicométricas do inventário de ansiedade traço-estado IDATE [dissertação de mestrado] Rio de Janeiro: Pontifícia Universidade Católica do Rio de Janeiro; 2006.
17.Ministério da Saúde (Br). Conselho Nacional de Saúde. Normas de pesquisa envolvendo seres humanos-Resolução. no 466/2012. Bioética. Brasília (DF): Editora MS; 2012.
18.Polit DF, Beck CT, Hungler BP. Fundamentos de pesquisa em enfermagem: métodos, avaliação e utilização. 5aed. Porto Alegre (RS): Artmed; 2004.
19.Moraes LO, Peniche ACG. Ansiedade e mecanismos de coping utilizados por pacientes cirúrgicos ambulatoriais. Rev esc enferm USP. 2003; 37: 54-62.
20.Sampaio CEP, Costa TMN, Araújo D, Santoro DC. Mecanismos de enfrentamento desencadeados por pacientes em situação estressora: cirurgia ambulatorial. Rev enferm UERJ. 2013; 24: 515-20.
21.Chistóforo BEB, Carvalho DS. Cuidados de enfermagem aos pacientes cirúrgicos no período pré-