RESEARCH ARTICLES
Humanization of medical and nursing care to the patient during surgery at a university hospital
Andréia Cristina BarbosaI ; Fábio de Souza TerraII; João Batista Vieira de CarvalhoIII
INurse. Master's Degree in Health Sciences at the José do Rosário Vellano University. Professor at the Department of Nursing, José do Rosário Vellano University. Alfenas, Minas Gerais, Braszl. Email: andreiacbc1@hotmail.com.
IINurse. PhD in Sciences through thr Fundamental Nursing Program, School of Nursing of Ribeirao Preto, University of Sao Paulo. Assistant Professor, Federal University of Alfenas. Minas Gerais, Brazil, Email: fabio.terra@unifal-mg.edu.br.
IIIPhD in Surgery from the Federal University of Minas Gerais. Professor in Cardiovascular Surgery, Faculty of Medical Sciences, José do Rosário Vellano University. Member of Cardiovascular Surgery Services, University Hospital Alzira Vellano, Alfenas, Minas Gerais, Brazil. Email: joao.batista@unifenas.br.
DOI: http://dx.doi.org/10.12957/reuerj.2014.2605
ABSTRACT: The surgical patient lives moments of fear and anxiety, which can be remedied with a humanized and individualized care. The objectives of this study were to identify the feelings experienced in the perioperative period, verify the existence of preoperative guidelines and patients' satisfaction regarding the care provided. This is a descriptive study using the statistical method. The population consisted of 100 patients aged over 12 years, both genders. Data collection took place in a university hospital in southern Minas Gerais February-July 2007 through the application of an adapted questionnaire with open and closed questions. The results revealed that preoperative period 68% of respondents had feelings of fear, and 32% of patients received no guidance. As for assistance, 17% had complaints. The data showed that there is need for improvement actions and attitudes aimed at humanizing assistance to the client during hospitalization.
Keywords: Surgery; orientation; humanization; hospitalization.
INTRODUCTION
Humanization is one of the most discussed topics at present, particularly when applied to the context of health care. Humanization of care for the patient who is hospitalized is of paramount importance when an institution has in its work philosophy the quality of care and has an interest in providing better client service for their satisfaction and recognition of the quality of services offered.
The humanization of healthcare began with the implementation of a program of the Unified Health System (SUS), Humanized SUS, when a Brazilian minister identified a growing number of complaints from users1. Therefore, with technological advances, customer care has become fragmented, and increasingly health professionals are specializing and losing touch with it. This way, thier emotions, beliefs and values have moved to the background, and the scientific knowledge related to diseases started to be the target, and with this, care has become inhumane. It is important that the health professional rescue the human essence of care, to ensure that care is humanized and of quality.
In the year 2001, was deployed the National Program for the Humanization of Hospital Care (PNHAH) that started actions to the creation, in hospitals, in humanization committees in order to improve cae for the user and worker2,3. This served as a basis for the implementation of the National Policy of Humanization (PNH) with emphasis on patient care, which goes beyond the technical care, procedures and scientific knowledge4.
Hospitalization generates expectations that reflect directly on the patient in their recovery, since it awakens feelings that are increased when the need for surgery arises5. Surgery is stress factor and generates many uncertainties for whatever reason. The surgical center is an unknown environment to the customer, has routines and equipment that differ from those found in hospitalization units, so the patient has his anxiety increased, and may express their feelings of fear, anxiety and insecurity, changing your high-esteem and even causing frustrations. Also their basic psychological and physiological needs are affected leading to a change in the physical and emotional balance6,7.
The preoperative period is the time that precedes the surgical event, and at that time, the customer exposes the feelings of fear of the unknown, anxiety and fears. It is the period that he becomes more dependent on other people, needing to have his needs met and also the time when he most needs attention and guidance, as sometimes the affection and respect are needed more than the actual orientation5,6,8. The pre-operative orientation when performed effectively can reduce anxiety and responses to psychological stress before and after surgery8.
Given the above, the objectives of this study were to identify the feelings experienced in the perioperative period, verify the existence of preoperative guidelines and patients' satisfaction regarding the care provided.
LITERATURE REVIEW
The impacts of hospitalization and surgical procedures may lead the patient to a series of internal conflicts causing structural and functional changes that can lead to emotional and psychosocial imbalances. These favor the increase in anxiety, arousing the feelings of fear, stress and discomfort that intensify the extent in which the surgical procedure anesthetic arrives, this often occurs when the reception is not satisfactory and needs related to the pre-operative period are not prioritized6,9.
Thus, the surgical procedure requires prior preparation, and this preparation is carried out through the preoperative nursing visit that is meant to explain all the moments that involve the trans-operative, clarifying the completion of exams, the need for procedures and be aware of the complications resulting from the procedures, also provide calmness and tranquility thus reducing the anxiety caused by lack of information and appropriate care offered to the patient6,8,10,11.
The nurse must provide information regarding the rules and routines and how to treat, monitor the patients and if show available to remedy the doubts whenever necessary, building a relationship of trust and communication4. When performing the orientation, one must raise the needs of knowledge and clarification of the patients while respecting the level of instruction of each one for the communication to be effective, and thus the greater the understanding the lower the level of anxiety in that period. Despite its importance, there is a lack of orientations in hospitals, during the preoperative period, tackling issues to be clarified about the surgical event5,12.
It is important that the patient receives individualized care, that is, taking into account the needs and expectations of each one in particular, to ensure that assistance is humanized throughout the perioperative period, thereby providing security, self-esteem, physical and emotional integrity13.
Humanizing means become human, give humane conditions to man, has a relationship with the human being, as a single, complete and complex that should be treated with respect and empathy, receiving a holistic care and integral to the well-being, the recovery of be and the establishment of bonds, being nothing more than a relationship of meeting and reception14,19.
Humanization becomes necessary in hospitals as the technology advances, because with the technical and scientific development associated with the characteristics of the surgical center, considered as a complex unit with work and bureaucratic management, the nurse has just moving away from patient care, hindering their work as qualified professional, which promotes the bio-psychosocial and spiritual well-being6,20,21. The use of technological resources and equipment are essential, but transforms the mechanized work, which can threaten the humanized care3. And when the focus is in machinery, in procedures and pathologies the environment and care are increasing depersonalization, influencing the humanized care, that goes beyond the technical, therefore, involves feelings of dedication to another13,19. In addition, a humanized hospital contemplates throughout its structure the appreciation and respect for the human person18. Thus, in order to humanize the care provided to the surgical client there is a need for change in the philosophy of the institution, training and behavior change of nursing professionals, awareness and preparation for making a difference in the care and promote an individualized and humanized care13.
METHODOLOGY
This is a descriptive, quantitative, cross-sectional study conducted in a university hospital, located in the South of Minas Gerais state in Brazil. The sample consisted of 100 patients who met the following criteria: age over 18 years, both genders, attended by SUS, with indication for elective surgery, hospitalized in the medical and surgical unit of the respective hospital. A convenience sample was investigated from February to July of 2007.
The data collection was performed by means of semi-structured interviews, using an adapted questionnaire with closed and open-ended questions as its instrument, which dealt with matters relating to the characterization of the population under study and information from the pre and post-operative periods. The application of the questionnaire was initiated in the preoperative period and finalized in the postoperative period. Data collection was complemented with consulting the information from the medical record of the patient regarding the perioperative period.
The study was approved by the Ethics Committee in Research of the University of Alfenas under Opinion No 111/2006. The study was carried out with the client's consent, which had signed a written informed consent, after being instructed on the study.
The data collected were recorded without distortion and the analysis given by statistical method, using the Chi-square Test, p< 0.05, and significance level of 5%.
RESULTS AND DISCUSSION
Of the 100 clients who met the inclusion criteria, 61 (61%) were male and 39 (39%) were female. The ages ranged between 13 and 80 years, with the greatest number of respondents was between 36 and 45 years, which corresponded to 36 (36% ); 30 (30%) had more than 45 years and 8% were aged 18 years. Regarding education, 50 (50%) had completed elementary school, 15 (15%) were illiterate and only 2 (2%) completed higher education. In relation to marital status, 45 (45%) were single, 44 (44%), married. The predominant religion was Catholic, with 76 (76%), and 17 (17%) were evangelical. In terms of occupation, 25 (25%) were retired; with the same quota of 12 (12% ), were the occupations of farmer and student, 19 (19%) reported other professions, among them general services, mechanical, nurses and nursing technicians, trader, painter, teacher, justice official, health agent, receptionist, maid and secretary.
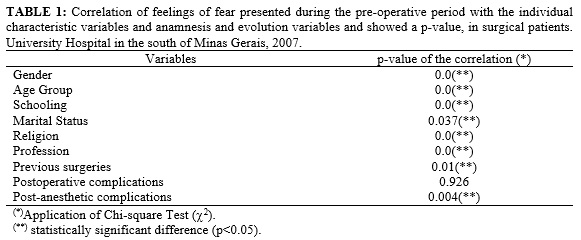
The feeling of fear had statistically significant correlation with the variables: gender, age, schooling, marital status, religion, occupation, previous surgeries and post-anesthetic complications as shown in Table 1.
Previous studies show that the patients in the preoperative feature a combination of feelings, such as concern, fear, nervousness, and anxiety. In addition, that the preoperative anxiety is more prevalent in women and this may be related to coping or adaptation mechanisms that male patients present before surgery11. Studies show that in addition to the doubts about the surgery, patients express feelings of fear, anxiety and nervousness6.
The patient who is at the productive age feels more insecure22. The lower the patient's education level, the less knowledge about the surgical procedure he has, which could lead to an increase in the fear due to the unknown23. The more information the patient receives the less unknown becomes the surgical event and less anxiety and the better the recovery6,8. Regarding their previous surgical experience, studies show greater security on the part of patients, because they already know what will happen8.
Regard the orientations given in the preoperative period, 52 (52%) clients have received orientation as to the type of surgery, 53 (53%) were counseled on the anesthesia, 58 (58%) had received orientation on the stay in the post anesthesia recovery room, and 77 (77%) patients were not informed about the post-operative period, as shown in Table 2.
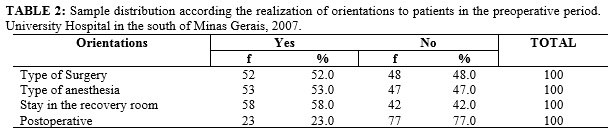
The orientations related to the type of surgery, the type of anesthesia, on the stay in the post anesthesia recovery room, it can be seen that the difference between those who received information and those who did not was small, indicating that there are still many clients that are not being informed as to the procedures that they will be submitted. The greatest concern of surgical patients is related to the lack of information, in this sense, the nurse must provide information related to the entire perioperative period, thus reducing the anxiety11. Moreover, in relation to the guidelines to be followed in the postoperative period, the majority of patients was not geared 77 (77%) as outlined in Table 2.
In previous studies, when some are informed and others are not, this shows a lack of consistency in information7. These are carried out in a very similar manner with all patients, in a manner that is not individualized; this may explain the fact that many patients reporting does not remember what was oriented. In addition, the anxiety can hinder the apprehension of information8. A patient is not informed as to the procedures can go through moments of stress6. It is emphasized that the importance of nurses to inform and orient patients in the preoperative preparation with the objective of reducing the negative feelings experienced at the time10.
It is known that many hospitals do not perform a nursing preoperative visit, thus, not meeting the needs of patients before surgery. This confirms the contradictions that exist between the real and the ideal, because the institutions are not adhering to the National Policy of Humanization6. Another factor that makes it impossible for the implementation of the orientations is the lack of knowledge of the reality and of practical experience on the part of professionals12. Recently trained nurses have many difficulties in overcoming the institution's routines, failing to propose strategies for changes20. To introduce changes to the routines and the humanization of the institutions, it is assumed that establishing an educational process where there is the effective participation of workers so that they can assume their real role18. Studies show that there is a deficiency in the communication between the multi-professional team12, which undermines the results in the post-operative period24.
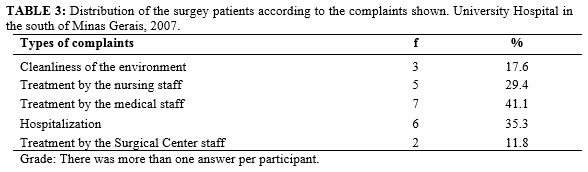
Of the 18 patients who had lodged a complaint regarding the service, 7 (41.1%) complained about the treatment of the medical team, 6 (35.3%) complained of service receipt, and 5 (29.4%) presented with complaints related to the treatment of the nursing team, as shown in Table 3. Of the complaints related to the treatment of the medical staff, it was observed that the lack of staff orientation, speaks very high within the surgical center, lack of explanation regarding the procedures to be performed. Regarding the complaints related to the nursing staff, it was noted that the lack of orientation regarding the procedures to be performed, and the lack of affection and patience of some members of the team. As for the reception, the claims related to the delay in service, long wait in the hospitalization sector before forwarding to the room.
Given the National Policy of Humanization, the reality is that many services are not prepared to accommodate users of SUS and, according to the guidelines of this policy, the nursing should also commit to ensure the promotion, protection, well-being and health6. Humanization has been one of the central themes in the training of health professionals, and the role of universities is to bring these professionals to learn to provide integral and holistic care to the patient15.
To speak with care, as soon as we treat the other with affection, love and respect, in order to strengthen the bond between professionals, patients and family members17, since these are prerequisites for the humanization, but what can be observed in practice, is that this involvement is not3, hence, it has been the dehumanization16. In addition, to have a humanized care also need to articulate the technological advances with human relations, since the technology is important for the quality of care, but cannot replace the human care19.
From there, there is a question mark? Does an individual who does not receive orientations from the doctors and nurses, that is not served with care and respect, and waiting hours in the hospitalization sector to be cared for receives humanized care? To humanize a service it is necessary to correct many aspects related to failures in health care, such as long delays, lack of guidance and integral care, physical structure, among other things, taken as dehumanizing, requiring the attention of managers25.
CONCLUSION
The results presented in this study allow us to conclude that the main feeling experienced by patients in the perioperative period is fear. Moreover, the fears can be solved from the orientations offered in the period before the surgery, decreasing anxiety. Therefore, it was found that the guidelines for pre-operative, although considered mandatory, are not being carried out in an effective way, and that the practices serve partially to the guidelines of the PNH, knowing that, to provide information to the patient have an individualized and humanized care.
Although the majority of the interviewees did not submit complaints regarding the service, the data showed that there is a need for improvement of actions and attitudes toward the humanization of the client, during the hospitalization, since there are still complaints about the treatment.
It is worth mentioning that one of the limitations of the study was that a sample size calculation to define a representative sample. Still, used as a convenience sample, the number was reduced, because many patients refused to participate in the study. This condition prevents the generalization of the findings.
1.Backes DS, Koerich MS, Erdmann AL. Humanizing care through the valuation of the human being: resignification of values and principles by health professionals. Rev Latino-Am Enfermagem. 2007; 15: 34-41.
2.Ministério da Saúde (Br). Programa Nacional de Humanização da Assistência Hospitalar. Brasília: Ministério da Saúde; 2001.
3.Camponogara S, Santos TM, Seiffert MA, Alves CN. O cuidado humanizado em unidade de terapia intensiva: uma revisão Bibliografica. Rev Enferm UFSM. 2011; 1(1):124-32.
4.Costa R, Klock P, Locks MOH. Acolhimento na unidade neonatal: percepção da Equipe de enfermagem. Rev enferm UERJ. 2012; 20: 349-53.
5.Garcia SD, Garanhani ML, Tramontini CC, Vannuchi MTO. O significado do cuidado perioperatório para o idoso. Rev Enferm UFSM. 2014; 4(1):55-66.
6.Giron MN, Berardinelli LMM, Santos FHE. O acolhimento no centro cirúrgico na perspectiva do usuário e a política nacional de humanização. Rev enferm UERJ. 2013; 21:766-71.
7.Silva JP, Garanhani ML. O significado do cuidado perioperatório para a criança cirúrgica. Rev Eletr Enf [Internet]. 2011; [citado em 12 abr 2014] 13:259-68. Disponível em: http://www.fen.ufg.br/revista/v13/n2/v13n2a12.htm.
8.Kruse MHL, Almeida MA, Keretzky KB, Rodrigues E, Silva FP, Schenini FS, Garcia VM. Orientação pré-operatória da enfermeira: lembranças de pacientes. Rev Eletr Enf [Internet]. 2009;11:494-500. Available at: http://www.fen.ufg.br/revista/v11/n3/v11n3a05.htm.
9.Costa VASF, Silva SCF, Lima VCP. O pré-operatório e a ansiedade do paciente: a aliança entre o enfermeiro e o psicólogo. Rev SBPH. 2010;13:282-98.
10.Perrando MS, Beuter M, Brondani CM, Roso CC, Santos TM, Predebon GR. O preparo pré-operatório na ótica do paciente cirúrgico. Rev Enferm UFSM. 2011; 1(1):61-70.
11.Santos MA, Rossi LA, Paiva L, Dantas RAS, Pompeo DA, Machado ECB. Medida da ansiedade e depressão em pacientes no pré-operatório de cirurgias eletivas. Rev Eletr Enf [Internet]. 2012; [citado em 12 abr 2014] 14:922-7. Available from: http://www.fen.ufg.br/revista/v14/n4/v14n4a21.htm.
12.Baggio MA, Nascimento KC, Arzuaga MA, Erdmann AL. Aprendizaje basado en problemas: la comunicación em la integración teórico-práctica en Enfermería. Revista Cubana de Enfermería. 2010; 26: 257-66.
13.Santana JCB, Campos ACV, Dutra BS, Borges CM, Souza AB, Santos VH. O cuidado humanizado sob a percepção dos enfermeiros. Rev Enfermagem Revista. 2012; 15(1): 47-57.
14.Oliveira NES, Oliveira LMAC, Lucchese R, Alvarenga GC, Brasil VV. Humanização na teoria e na prática: a construção do agir de uma equipe de enfermeiros. Rev Eletr Enf [Internet]. 2013; 15:334-43. Disponível em: http://www.fen.ufg.br/fen_revista/v15/n2/pdf/v15n2a04.pdf
15.Casate JC, Corrêa AK. A humanização do cuidado na formação dos profissionais de saúde nos
cursos de graduação. Rev esc enferm USP. 2012; 46:219-26.
16.Corbani NMS, Brêtas ACP, Matheus MCC. Humanização do cuidado de enfermagem: o que é isso? Rev Bras Enferm. 2009; 62: 349-54.
17.Santos MR, Silva L, Misko MD, Poles K, Bousso, RS. Desvelando o cuidado humanizado: percepções de enfermeiros em oncologia pediátrica. Texto contexto - enferm. 2013; 22(3): 646-53.
18.Figueiredo ACA, Coelho CJ. Humanização–qualidade de trabalho dos Servidores laboratoriais do hospital universitário da universidade federal da Grande dourados – UFGD. Rev UNINGÁ. 2014; 39:75-91.
19.Silva LJ, Silva LR, Christoffel MM. Tecnologia e humanização na unidade de terapia intensiva neonatal: reflexões no contexto do processo saúde-doença. Rev esc enferm USP. 2009; 43:684-9.
20.Peres EC, Barbosa IA, Silva MJP. Cuidado humanizado: o agir com respeito na concepção de
aprimorandos de enfermagem. Acta Paul Enferm. 2011; 24:334-40.
21.Brito FM, Costa ICP, Andrade CG, Lima KFO, Costa SFG, Lopes MEL. Espiritualidade na iminência da morte: estratégia adotada para humanizar o cuidar em enfermagem. Rev enferm UERJ. 2013; 21: 483-9.
22.Matsuda LM, Silva N, Tisolin AM. Humanização da assistência de enfermagem: estudo com clientes no período pós-internação de uma UTI-adulto. Acta Scientiaum Health Sciences. 2003; 25: 163-70.
23.Jorgettto GV, Noronha R, Araújo IEM. Estudo da visita pré-operatória de enfermagem sobre a ótica dos enfermeiros do centro cirúrgico em um hospital universitário. Rev Eletr Enferm. 2004; [citado em 12 abr 2014] 6: 213-22. Disponível em: http://www.fen.ufg.br/fen_revista/revista6_2/pdf/Orig8_visita.pdf
24.Santos J, Henckmeier L, Benedet AS. O impacto da orientação pré-operatória na recuperação do paciente cirúrgico. Enfermagem em Foco. 2011;2(3):184-7.
25.Beck CLC, Gonzales RMB, Denardin JM, Trindade LL, Lautert L. A humanização na perspectiva dos trabalhadores de Enfermagem. Rev Texto contexto - enferm. 2007; 16(3): 503-10.