 FIGURE 1: Descending hierarchical classification (dendrogram) of the analysis of the interviews to nurses who work in the Family Health Strategy. Recife, 2013.
FIGURE 1: Descending hierarchical classification (dendrogram) of the analysis of the interviews to nurses who work in the Family Health Strategy. Recife, 2013.ORIGINAL RESEARCH
Language development: nurses' approach in child care consultations
Luiziane Souza Vasconcelos de LimaI; Iracema da Silva Frazão II; Bianca Arruda Manchester de QueirogaIII
I
Nurse. Master in Children and Adolescent Health of the Federal University
of Pernambuco. Camaragibe, Pernambuco, Brazil. E-mail: luiziane.lima@gmail.com
II
Nurse. Post-Ph.D. in Bioethic. Assistant Professor II, Federal University
of Pernambuco. Recife, Pernambuco, Brazil. E-mail: isfrazao@gmail.com
III
Speech Therapist. Ph.D. in Psychology. Associate Professor, Federal
University of Pernambuco.Recife, Pernambuco, Brazil. E-mail: queiroga.bianca@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2016.16051
ABSTRACT
Objective: to know the nurses' approach on language development during childcare consultation. Method: a qualitative and descriptive study, was conducted with 30 nurses of the family health units in Recife / Pernambuco; the sample was determined by exhaustion criterion. Data were collected in 2013, using a questionnaire for informants characterization, semi-structured interviews and the evaluation of 150 medical records according to a form. The interviews were analyzed by Alceste software, version 2010. Project approved by the Research Ethics Committee (CAAE No 11106112.6.0000.5208). Results: nurses recognize the importance of language development observation. However, this is not a priority in the consultation. It was also observed a lack of preparation to evaluate the development of language. Only 4% of the records had record on language development. Conclusion: Permanent education program for professionals working in childcare is needed, in order to make possible the integral assistance as recommended by the Ministry of Health.
Keywords: Language development; infant care; delivery of health care; pediatric nursing.
INTRODUCTION
Aiming to reduce child morbidity and mortality, the Ministry of Health (MOH) created the Comprehensive Assistance Program for Child Health (PAISC) in 1984. Five basic actions were advocated in it, such as the monitoring of growth and development. This follow-up is done through periodic childcare consultations which, in the Family Health Strategy (ESF) is carried out usually by nurses1.
During the consultation, the professional should observe the main developmental references, detect and forward early children at risk of changes to specialized care, among other behaviors2.
MOH offers and recommends the use of the Development Monitoring Form and Development Surveillance Instrument to standardize and guide the observation and identification of children with probable developmental problems, including language development. The Development Surveillance Instrument is inserted in the Child Health Handbook since 20052,3.
Despite this, studies with nurses4 and with physicians 5 point out that the observation of language development during childcare consultations is not performed as recommended by the MOH.
Considering this problem, this article aimed to know the approach of nurses on the development of language in childcare consultations.
LITERATURE REVIEW
During the child´s life, there are events suggesting an adequate development, such as head support, crawling and walking. However, motor conquests alone do not indicate adequate child development. In this case, the most appropriate evolutionary indicator is the appearance of language, since this achievement emerges from social, communicative, intellectual and affective skills that are significantly complex and evolved6.
The process of language development begins months before the child expresses his or her first word since receptive language (understanding of spoken language) precedes expressive language (sounds, signs or symbols to convey meaning)7.
The emergence of the language is one of the most important aspects to follow, and its alterations as frequent problems in child development, reach about 3 to 15% of children5.
Verbal (speech) and nonverbal expressions (gestures and body language consistently used by the child to communicate meaning) are characteristics of human communication that can be perceived throughout life8. These expressions should be observed by health professionals, especially in childcare consultations, since there is a close relationship between healthy language development, learning, and social insertion, as well as repercussions of language difficulties in school performance and cognitive evolution. Therefore, communication directly influences the individual and the environment in which he/she is inserted9.
METHODOLOGY
This is a descriptive study with a qualitative approach10,11, developed in 40 health units of the family (USF) of the Sanitary District (DS) IV of the city of Recife/PE12,13, with 30 nurses who work in the USFs and who voluntarily participated in the research.
The study was conducted between March and May 2013, and the choice of DS IV was through the partnership with UFPE in the research area.
PAISC guidelines were used as a guiding element for the analyses and discussions, since it is the MOH program that guides all actions of children's health under five years old2,14.
The sample used the exhaustion criterion, where all available individuals 15 were included in the collection period, a fact that occurred with 30 of the 40 unit nurses.
A questionnaire was used to characterize the participants (identification number and others) and the semi-structured individual interview technique, with guiding questions that met the objective.
The data collection was done after approval of the Research Ethics Committee of the Health Sciences Center of the UFPE (CAAE nº 11106112.6.0000.5208) and after the nurses signed the Free and Informed Consent Term. The participants were identified with the letter E, followed by the interview order number, for example, E1, E2 to preserve anonymity.
The interviews took place in the USFs, according to pre-scheduling, being recorded and transcribed on the same day or the following day of collection 15.
After the interview, a script produced by the researcher was used, based on the developmental references in the Development Monitoring Form and the Child´s Handbook, both available by the MOH2. The script was intended to ascertain if there was a record of the observation of language development.
Five medical records of children assisted at the child care were analyzed by the interviewees, on the same day or the same week of the interview (for being the most recent records of the professional), making a total of 150 medical records.
The interviews were analyzed using the Lexical Contextual Analysis software of a Set of Text Segments (Alceste), version 2010, a program that uses statistical association between the lexical contents in the speeches to organize and summarize information considered more relevant16-18 .
Thus, Alceste studied the results, generating graphical representations, such as the dendrogram, whose list of words is the basic source for class construction16. In front of all the information, the researcher carried out an exhaustive reading of the dendrogram, to name and interpret each class.
RESULTS AND DISCUSSION
The mean age of the nurses was 39.4 years old, ranging from 29 to 59 years old and 28 (93%) of the female gender.
As for the training, the average time of graduation was 15.3 years ranging from 5 to 38 years; 24 (80%) attended a public university; all were specialists, 29 (97%) in the of family or public/collective health area and 4 (13%) had a master´s degree or in progress. Regarding the time working in the ESF, they were for 8.4 years on average, varying from 2.5 to 15 years.
Regarding the strategies of permanent education, 24 (80%) participated in the last 12 months of lecture/course/training in topics related to ESF, but none was related to childcare. Of the 150 records analyzed, 77 (51.3 %) were related to child development references, and only 6 (4%) were related to language development.
It is relevant that ESF professionals are permanently prepared for quality assistance since limitation in vocational training can negatively influence professional practice.
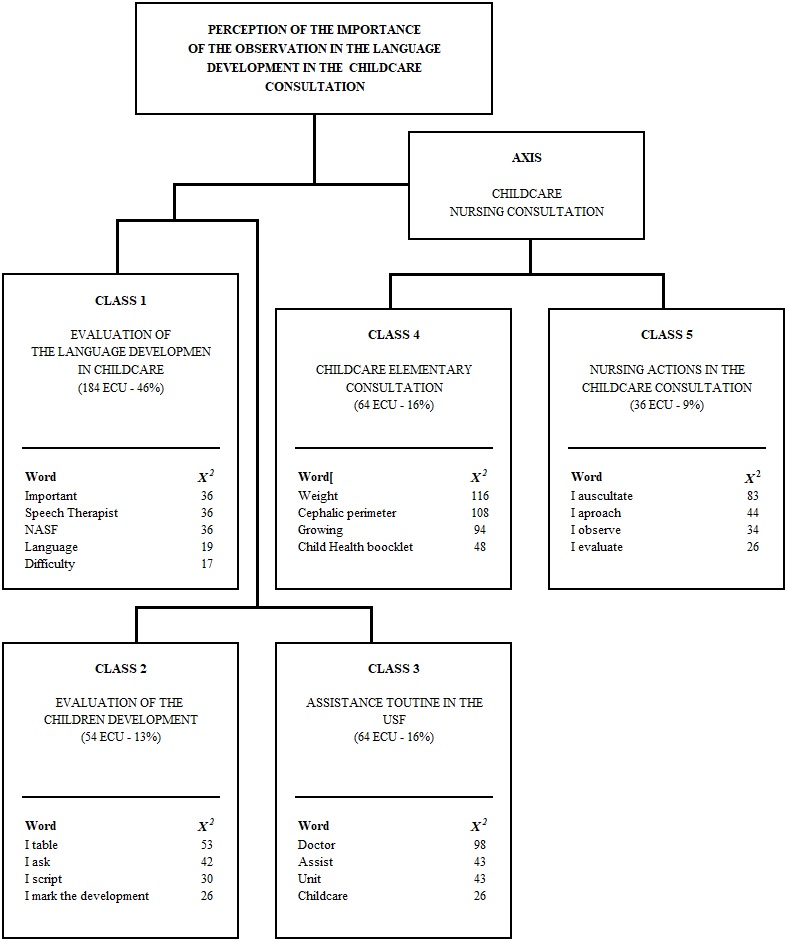
As for the interview data, the lexical analysis performed by Alceste identified 60 initial context units (ICU), the corpus was divided into 550 elementary context units (ECU), but 402 ECUs were classified for analysis, representing a use of 74% of the material. The richness of vocabulary was 97.1%.
The ECUs were divided into five classes, which focused on the following topics: Class 1 (184 ECUs - 46%): evaluation of language development in the child care consultation; Class 2 (54 ECUs - 13%): assessment of child development; Class 3 (64 ECUs - 16%): routine of attendance at USF; Class 4 (64 ECUs - 16%): elements of the child care consultation; Class 5 (36 ECUs - 9%): nursing actions in the child care consultation.
As there was a correspondence between the words of classes 4 and 5, it was decided to analyze them in the axis, before the division. Thus, four classes were left for analysis, as shown in Figure 1.
FIGURE 1: Descending hierarchical classification (dendrogram) of the analysis of the interviews to nurses who work in the Family Health Strategy. Recife, 2013.
Class 1
In Class 1, assessment of language development in the child care consultation, the importance of observation of language development during the consultation, the difficulty in perceiving language problems and the recognition of the lack of capacity to evaluate the development of the language prevailed.
I think it is important, but I do not approach it so much unless I realize something very something. (E6)
It is important, but my focus is on motor development. (E23)
During the application of the questionnaire to characterize the individuals, the interviewees voiced the lack of preparation (training) to perform in childcare, as highlighted by E24 and E28.
It is difficult for people who are a nurse; this is a speech therapy, I do not know if I have the ability to evaluate language development correctly. (E24)
I have difficulty evaluating; I do not think I am qualified. (E28)
As PAISC2 recommends, child care should be comprehensive, so language development is an important aspect to be assessed in consultations. However, this aspect has not been observed as it should be, as pointed out in the statements of E6 and E24.
In some sense, in spite of advocating the evaluation of language development, the MOH in its latest Growth and Development Manual prioritizes the observation of the motor reference in the first year of life, such as the Developmental Aspects of Child, in whom the language development reference is only mentioned in the two-year consultation 19. This fact may impair the quality of developmental surveillance, since the professional may infer that language developmental milestones will only appear after one year of life.
It is known that infants before expressing through speech, they already understand and express in non-verbal language. Usually motor and this aspect can be observed in the first months of life20. Before the first year of life, the child already has evidence of language and, if the appearance of speech does not occur in the expected period, the professional must evaluate the capacity for understanding, communication, and attention5.
It is important to emphasize that aspects of language development are intrinsically linked to some aspects of motor development. When the child has the support of the head to be able to turn towards the object or interlocutor, to express crying or smiling, it is using the physiological mechanisms of articulation, breathing, and phonation, which are also used in the acquisition of speech6.
One of the factors that may interfere with the quality of child health care is the lack of continuing education that focuses on childcare, a fact emphasized in this study, through the testimony of interviewees E24 and E28.
According to the National Curricular Guidelines (DCN)21, the graduate of the Nursing Undergraduate Course must have a generalist, humanistic, reflexive and critical profile and its actions based on technical and scientific rigor. At the undergraduate level, it is necessary to know and intervene on the health-disease problems prevalent at the national level and also in the region of action to be able to develop actions to prevent diseases, health promotion, and rehabilitation. The nurse must learn both in training and in practice through continuing education.
According to the study aimed to analyze the results provided by continuing education in child care in the ESF, it was verified the effectiveness of permanent education, being an important element to reduce the vulnerability of the child population, improving the quality of child health care 22.
Thus, inclusion of undergraduate content of information related to language development and the practice of continuing education is fundamental, so the professionals not only recognize the importance of integral observation of child development but also do so23.
Respondents E1 and E8 acknowledge the harm caused to children who have language development problems and are not detected early for referral and appropriate treatment.
The child will have trouble for the rest of his life if he does not have this initial development carefully. (E1)
In childhood, it is identified if it has any problem or not and the sooner the treatment and development of the child are better. (E8)
It is important for health professionals to be aware of their normal development, their changes, and the impact of early development for future stages of child development, so they can provide clarification to the family and identify the child at risk or with greater vulnerability, prioritizing care and, , referral for diagnosis and intervention as early as possible when necessary2,24.
A literature review carried out in the USA indicates that family support, early detection of risk factors and early care in the preschool years provide the best opportunity for early identification and appropriate intervention for problems that affect the development of children 25.
From this perspective, the child-care consultation proves, once again, as a screening tool in the early detection of risks and aggravations to language development26.
Class 2
In Class 2, Evaluation of child development, a description of the evaluation of child development during the consultation prevailed. The forms of evaluation expressed were the complaints brought by the mother or caregiver about the development, the observation of the child during the consultation and the physical examination. When there were no complaints or the professional could not observe something during the consultation, the mother/family was questioned about the child´s development at home.
Everything is from the mother´s report; she brings the complaints and most of the information. (E3)
This aspect was also observed in a study investigating the pediatrician's practice in the development of language that were routinely, the care of professionals focuses on the complaint of the family and the observation of language development is not a focus of research. Only in cases in which the complainant, anamnesis is carried out and the behavior to verify the complaint is observed5.
The use of instruments to systematically observe/evaluate the main developmental references during the consultation was mentioned in this research, but the interviewees reported difficulty in using the instruments suggested by the MOH to assess child development (child´s booklet and monitoring form) alleging lack of time and the work routine.
I think it is important to use the child´s booklet for this, but I do not because there is so much thing we have not time. (E2)
I do not use the card to guide me because so much time is doing this that it becomes routine work. (E22)
I use the MOH script that has in the child´s book. At the physical examination, I will observe and put if it is present or not. (E6)
A study conducted in the USA to describe the use of developmental screening tests among pediatricians found that physicians who applied developmental screening tests in child care had sufficient time to do so27.
Also in the USA in another study, aimed to analyze the feasibility and effectiveness of the implementation of developmental screening, it was pointed out that the professionals were given time in the consultation to investigate the developmental references using some test and observe the behavior of the child in the informal dialogue with the parents 28. Therefore, although in different public health contexts in this study and not with nurses´ evaluation, it can be seen that the argument used in the E2 discourse may not be justified according to the studies above.
Even in the USA, a study of 646 pediatricians showed that 61% of them did the clinical evaluation without using a screening instrument to identify children with developmental delays27.
In Brazil, it was identified that health professionals did not use tests and/or scales to assess child development references and the main references expected in the first year of life were observed based on knowledge and experience about the process of child development of these professionals4.
In Bahia, it was identified that in 77.9% of the booklets evaluated there was no completion of the development curve29. Failure to use the Child Health Handbook as a tool for systematically recording relevant information is contrary to the MOH recommendations30.
In the study with the objective to analyze the factors associated with the quality of the completion of the Child Health Handbook in Belo Horizonte, it was verified that only 18.9% of them had at least three notes on neuro psychomotor development23. Such a situation may compromise the quality of monitoring and surveillance of child development, since the professional may fail to observe any reference, since he does not use an instrument that allows a systematic and integral evaluation, since childcare consultation is a complex activity, where the professional must evaluate and observe, besides development, aspects related to growth, immunization, feeding, hygiene and health education31,32.
The Development Monitoring Form proposed by the MOH Manual for Child Development Surveillance constitutes an easy-to-apply screening instrument with a low operational cost and capable of performing early detection of delays and should be part of the actions of the nurse in the child care consultation26.
Therefore, the use of screening instruments for child development is important because it helps to increase the accuracy of the development monitoring process. When the professional uses only the physical examination - rather than a standardized assessment - he runs the risk of estimating development in the wrong way. For this reason, the benefits of screening and developmental surveillance are not limited to the child with developmental problems, but to all children, as well as to professionals, as it is an anticipatory guide to the condition of child health 33.
It was found in this present research that in only two of the 150 records analyzed; there was the attached Child Development Monitoring Form.
The practice of not observing, not registering in the medical records and not using an observation instrument can impair the evaluation/observation of the developmental reference, during the child care consultation, can cause harm to the child and health surveillance, and it is not an integral follow-up in accordance with the guidelines of the PAISC.
Class 3
In Class 3, USF attendance routine, it was evidenced that during childcare there are medical and nursing consultations, but each team made its schedule regarding the frequency and quantity of these consultations, and there was no standardized routine among the units.
The unit´s doctor attends the child in the first month of life, twelve subsequent child-care consultations with me and then he returns to her. (E29)
The doctor of the unit has the participation in childcare in two consultations, in the first and the eighth month. (E21)
The lack of a protocol related to childcare routine (that is, a document that can guide the actions of health professionals) hinders the integral assistance to the child´s health24, which is in line with PAISC guidelines, recommending that the care must be integral and continuous 19.
A study carried out with the purpose of presenting a Nursing protocol for childcare consultation, based on the Roper-Logan-Tierney Nursing Model, showed that the use of the protocol is useful to guide Nursing care in childcare, allowing a standardized care and directed to the integral attention of the health of the child in its first months of life 34.
Also, a study that aimed to describe the daily routine of nurses in the child care consultation and to identify the factors that influence the day-to-day performance of this consultation highlighted that the organization of the health service is one of the factors that influence the daily routine of the consultation35.
Therefore, it is necessary to have an organization both in the form of care and in the organization of the health service so that the consultation in childcare happens in a satisfactory manner, resulting in the promotion, prevention, and recovery of health.
Axis: Nursing consultation in childcare
Finally, this axis, which represents the junction of classes 4 and 5, according to Figure 1, demonstrated the nursing actions performed in the child care consultation, the elements of the consultation and how it is performed. The most frequent evaluations during the consultation were the anthropometric measurements, and the evaluation of the reflexes was poorly observed.
It was identified that there is an emphasis on the evaluation of growth by the interviewees. It was found that breastfeeding was a point highlighted by all the respondents, but none addressed the repercussions for language, but the repercussions for the child´s growth.
Physical examination with anthropometric measurements. I use the child´s handbook to record the growth and especially to record the vaccine. (E29)
It is easy to keep up with the growth because the measurement is something palpable. Anthropometric measures are verified by instruments such as measuring tape and scale. However, to follow child development, it is necessary also to the development screening sheet, to identify risk factors to which the child may be exposed, to know the customs and myths of his community and especially his personal relationships (especially those of his family)36.
Only from the 90's, the MOH in its manuals and guidelines, inserted in the assistance an instrument of development surveillance. It is a fact sheet containing developmental references19. Possibly, this fact and the affirmations of the study36 above may justify the performance of health professionals who prioritize the monitoring of growth in childcare, as verified in E29.
CONCLUSION
This study revealed that nurses recognize the importance of observing language development during childcare consultations. However, they do not assume such behavior. They claim lack of knowledge to detect possible deviations from normality and sometimes find it unnecessary to use any instrument to systematically evaluate the main developmental references, considering their experience as sufficient for such observation. For the child, the absence of observation and registration will hinder to diagnose early language problems that may affect their development.
As limitations of the study, there was little exploitation of the medical record to evaluate all the consultations and not just the last consultation, as was done. It could have analyzed the children's handbooks to check whether or not the development references and the observation of the child-care consultation were completed to find out how this evolution is monitored. Also, there was no time to develop continuing education activities that provided reflection on the importance of systematic observation of child development, especially language.
aThis study points to the need for future work aimed at carrying out continuing education actions with ESF professionals, involving the importance of global child assessment, including the monitoring of language development and the impacts on children´s lives when there is no detection and early treatment. Thus, it will be possible to provide comprehensive care that focuses on health promotion during childcare, according to what is recommended by PAISC.
REFERENCES
1.Ministério da Saúde (Br). Secretaria de Assistência à Saúde. Coordenação de Saúde da Comunidade. [site de Internet] Saúde da Família: uma estratégia para a reorientação do modelo assistencia. Brasília (DF): Ministério da Saúde; 1997; [cited in mar 12 2016]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/cd09_16.pdf.
2.Ministério da Saúde (Br). Secretaria de Políticas de Saúde. Departamento de Atenção Básica. [site de Internet] Saúde da criança: acompanhamento do crescimento e desenvolvimento infantil. Brasília (DF): Ministério da Saúde; 2002; [cited in mar 12 2016]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/crescimento_desenvolvimento.pdf.
3.Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Departamento de Ações Programáticas Estratégicas. [site de Internet] Área Técnica da Saúde da Criança e Aleitamento Materno. Manual para utilização da caderneta de saúde da criança. Brasília (DF): Ministério da Saúde; 2005; [cited in mar 12 2016]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/manual%200902.pdf.
4.Saparolli ECL, Adami NP. Avaliação da qualidade da consulta de enfermagem à criança no Programa de Saúde da Família. Acta Paul de Enferm. [Scielo-Scientific Electronic Library Online] 2007; [cited in mar 12 2016]. 20 (1) : 55-61. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0103- 21002007000100010&lng=en. http://dx.doi.org/10.1590/S0103-21002007000100010.
5.Maximino LP, Ferreira MV, Oliveira DT, Lamônica DAC, Feniman MR, Spinardi ACP et al. Conhecimentos, atitudes e práticas dos médicos pediatras quanto ao desenvolvimento da comunicação oral. Rev CEFAC. [Scielo-Scientific Electronic Library Online] 2009; [cited in mar 12 2016]. 11 (2) : 267-73. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S1516-18462009000600017
6.Zorzi JL. Aspectos básicos para compreensão, diagnóstico e prevenção dos distúrbios de linguagem na infância. Rev CEFAC. [Scielo-Scientific Electronic Library Online] 2000; [cited in mar 12 2016].2: 11-5. Available from: http://www.cefac.br/revista/revista21/Artigo%202.pdf.
7.Bee H, Boyd D. A criança em desenvolvimento. Tradução de Cristina Monteiro. 12ª ed. Porto Alegre (RS): Artmed; 2011.
8.Palangana IC. Desenvolvimento e aprendizagem em Piaget e Vygotsky a relevância do social. 3ª ed. São Paulo : Summus ; 2001.
9.Goulart BNGd, Chiari BM. Comunicação humana e saúde da criança: reflexão sobre promoção da saúde na infância e prevenção de distúrbios fonoaudiológicos. Rev CEFAC. [Scielo-Scientific Electronic Library Online] 2012; [cited in mar 12 2016]. 14 (4) : 691-6. Available from: http://www.scielo.br/scielo.php?pid=S1516-18462012000400012&script=sci_abstract&tlng=pt.
10.Minayo MCS. O desafio do conhecimento: pesquisa qualitativa em saúde. 11ª ed. São Paulo: Hucitec; 2004.
11.Flick U. Qualidade na pesquisa qualitativa. Tradução de Roberto Cataldo Costa. Porto Alegre (RS): Artmed; 2009.
12.Instituto Brasileiro de Geografia e Estatística (Br). Censo 2010: contagem populacional. [site de internet] 2010; [cited in mar 12 2016]. Available from: .
13.Secretaria Municipal de Saúde do Recife (Br).Plano Municipal de saúde de Recife 2010/2013. [site de internet] Recife (PE): 2010. [cited in mar 12 2016]. Available from: http://www.recife.pe.gov.br/noticias/arquivos/5916.pdf.
14.Castro IRRd. Vigilância alimentar e nutricional: limitações e interfaces com a rede de saúde. Rio de Janeiro: FIOCRUZ [Scielo-Scientific Electronic Library Online] 1995; [cited in mar 12 2016]. Available from: http://static.scielo.org/scielobooks/v9/pdf/castro-9788575412947.pdf.
15.Turato ER. Tratado da metodologia da pesquisa clínico-qualitativa. 5ª ed. Petrópolis (RJ): Vozes; 2011.
16.Camargo BV. Alceste: um programa informático de análise quantitativa de dados textuais. In: Moreira ASP, Camargo BV, Jesuíno JC, Nóbrega SM, organizadores. Perspectivas teórico-metodológicas em representações sociais. João Pessoa (PB): Editora Universitária; 2005. p. 511-39.
17.Gomes AMT, Oliveira DC. A auto e heteroimagem profissional do enfermeiro em saúde pública: um estudo de representações sociais. Rev Latino-Am Enfermagem. 2005; [cited in mar 12 2016] 13 (6): 1011-8. Available from: http://www.redalyc.org/articulo.oa?id=281421850014.
18.Oliveira DC, Sá CP, Gomes AMT, Ramos RS, Pereira NA, Santos WCR. A política pública de saúde brasileira: representação e memória social de profissionais. Cad Saúde Pública. [Scielo-Scientific Electronic Library Online] 2008; [cited in mar 12 2016]. 24 (1) : 197-206. Available from: http://www.scielo.br/pdf/csp/v24n1/19.pdf.
19.Ministério da Saúde (Br). Política Nacional de Atenção Básica. Brasília (DF): Editora MS; 2012; [cited in mar 12 2016]. Available from: http://189.28.128.100/dab/docs/publicacoes/geral/pnab.pdf
20.Zorzi JL. Falando e escrevendo: desenvolvimento e distúrbios da linguagem oral e escrita. Curitiba(PR): Editora Melo; 2010.
Ministério da Educação (Br). Resolução CNE/CES nº 3, de 7 de Novembro de 2001. Institui Diretrizes Curriculares Nacionais do Curso de Graduação em Enfermagem. [site de Internet]. Brasília: DF; 2001; [cited in mar 12 2016]. Available from: http://portal.mec.gov.br/cne/arquivos/pdf/CES03.pdf.
22.Feliciano KVO, Kovacs MH, Costa IER, Oliveira MG, Araújo AMS. Avaliação continuada da educação permanente na atenção à criança na estratégia saúde da família. Rev Bras Saúde Matern Infant. [Scielo-Scientific Electronic Library Online] 2008; [cited in mar 12 2016]. 8 (1) : 45-53. Disponívem em: http://www.scielo.br/scielo.php?pid=S1519-38292008000100006&script=sci_abstract&tlng=pt.
23.Alves CRL, Lasmar LMLBF, Goulart LMHF, Alvim CG, Maciel GVR, Viana MRA et al. Qualidade do preenchimento da Caderneta de Saúde da Criança e fatores associados. Cad Saúde Pública. [Scielo-Scientific Electronic Library Online] 2009; [cited in mar 12 2016]. 25 (3) : 583-95. Available from: http://www.scielo.br/scielo.php?pid=S0102-311X2009000300013&script=sci_arttext.
24.Vieira VCdL, Fernandes CA, Demitto MdO, Bercini LO, Scochi MJ, Marcon SS. Puericultura na atenção primária à saúde: atuação do enfermeiro. Cogitare Enferm. [Scielo-Scientific Electronic Library Online] 2012; [cited in mar 12 2016]. 17 (1) : 119-25. Available from: http://ojs.c3sl.ufpr.br/ojs/index.php/cogitare/article/view/26384.
25.Oberklaid F, Baird G, Blair M, Melhuish E, Hall D. Children's health and development: approaches to early identification and intervention. Arch Dis Child. 2013 [cited in 2016 Mar 12]. 98(12):1008-11. Available from: http://www.ncbi.nlm.nih.gov/pubmed/23968776
26.Santos MEA, Quintão NT, Almeida RXd. Avaliação dos marcos do desenvolvimento infantil segundo a estratégia da atenção integrada às doenças prevalentes na infância. Esc Anna Nery. [Scielo-Scientific Electronic Library Online] 2010; [cited in mar 12 2016].14 (3) : 591-8. Available from: http://www.scielo.br/scielo.php?pid=S1414-81452010000300022&script=sci_arttext.
27.Sand N, Silverstein M, Glascoe FP, Gupta VB, Tonniges TP, O'Connor KG. Pediatricians' reported practices regarding developmental screening: Do guidelines work? Do they help? Pediatrics. [ Pubmed] 2005; [cited in 2016 Mar 16] 116 (1) : 174-9. Available from: http://pediatrics.aappublications.org/content/116/1/174.
28.Schonwald A, Huntington N, Chan E, Risko W, Bridgemohan C. Routine developmental screening implemented in urban primary care settings: more evidence of feasibility and effectiveness. Pediatrics. [ Pubmed] 2009; [cited in 2016 Mar 16] 123 (2) : 660-8. Available from: http://www.ncbi.nlm.nih.gov/pubmed/19171635.
29.Vieira GO, Vieira TdO, Costa MCO, Santana Netto PV, Cabral VA. Uso do cartão da criança em Feira de Santana, Bahia. Rev Bras Saude Mater Infant. [Scielo-Scientific Electronic Library Online]. 2005; [cited in mar 12 2016]. 5 (2) : 177-84. Available from: http://www.scielo.br/scielo.php?pid=S1519-38292005000200006&script=sci_arttext
30.Secretaria Municipal de Saúde e Defesa Civil (RJ). Superintendência de Atenção Primária. Linha de cuidado da atenção integral à saúde da criança. [site de Internet]
Rio de Janeiro: 2010 [cited in mar 12 2016]. Available from: http://www.ensp.fiocruz.br/portal-ensp/judicializacao/pdfs/485.pdf.
31.Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Agenda de compromissos para a saúde integral da criança e redução da mortalidade infantil. [site de Internet] Brasília (DF): Editora MS; 2004; [cited in mar 12 2016]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/agenda_compro_crianca.pdf.
32.Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Política Nacional de Atenção Básica. [site de Internet]. Brasília (DF): Ministério da Saúde; 2006; [cited in mar 12 2016]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/politica_nacional_atencao_basica_2006.pdf.
33.Earls MF, Hay SS. Setting the stage for success: implementation of developmental and behavioral screening and surveillance in primary care practice: The North Carolina Assuring Better Child Health and Development (ABCD) Project. Pediatrics. [ Pubmed] 2006; [cited in 2016 Mar 12] 118 (1) : e-183-8. Available from: http://pediatrics.aappublications.org/content/118/1/e183.full.pdf+html
34.Gubert FA, Santos DAS, Pinheiro MTM, Brito LLMS, Pinheiro SRCS, Martins MC. Protocolo de enfermagem para consulta de puericultura. Rev Rene UERJ [Scielo-Scientific Electronic Library Online] 2015; [cited in mar 12 2016].16(1):81-9. Available from: http://www.revistarene.ufc.br/revista/index.php/revista/article/view/1853/pdf_1
35.Ribeiro SP, Oliveira DS, Fernandes SLSA, Felzemburgh RDM, Camargo CL. O quotidiano de enfermeiras na consulta em puericultura. Rev enferm UERJ [Scielo-Scientific Electronic Library Online] 2014; [cited in mar 12 2016]. 22(1):89-95. Available from: http://www.facenf.uerj.br/v22n1/v22n1a14.pdf
36.Alves CRL, Moulin ZS. Saúde da criança e adolescente: crescimento, desenvolvimento e alimentação. 2008. In: Caderno de estudo do Curso de Especialização em Atenção Básica em Saúde da Família (CEABSF/NESCON/FM/UFMG) [site de Internet]. Belo Horizonte (MG): Coopmed; [cited in mar 12 2016]. Available from: https://www.nescon.medicina.ufmg.br/biblioteca/imagem/1572.pdf