ORIGINAL RESEARCH
Food and nutrition actions in the family health strategy: structure and work process
Dixis Figueroa PedrazaI; Tarciana Nobre de MenezesII; Gabriela Maria Cavalcanti CostaIII
I
PhD in Nutrition. State University of Paraíba, Graduate Program in Public
Health. Campina Grande, Paraíba, Brasil. E-mail: dixisfigueroa@gmail.com
II
PhD in Nutrition. State University of Paraíba, Graduate Program in Public
Health. Campina Grande, Paraíba, Brasil. E-mail: tnmenezes@yahoo.com.br
III
PhD in Nutrition. State University of Paraíba, Graduate Program in Public
Health. Campina Grande, Paraíba, Brasil. E-mail: gabymcc@bol.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2016.15848
ABSTRACT
Objective: to characterize food and nutrition actions in the context of the family health strategy, and analyze the structure and work process. Method: this cross-sectional study was conducted in 2010 at 20 (29.85%) of the family health primary care units of Campina Grande. Data was collected by questionnaires answered individually by nurses and collectively by the healthcare team. The project was approved by the UEPB research ethics committee (No. 0355013300009). Results: in the absence of nutritionists, doctors and nurses conduct the main food and nutrition activities. These professionals, in addition to lacking proper structure, such as educational materials, face problems related to user population demand, adherence and socioeconomic status, and professional training is particularly important. Conclusion: food and nutrition actions in primary health care require the inclusion of nutritionists working with the support of a multidisciplinary team.
Keywords: Primary health care; health evaluation; family health program; nutrition programs.
INTRODUCTION
The Family Health Program (FHP), later called Family Health Strategy (FHS), emerged as a strategy to reorganize primary care in Brazil, by replacing the traditional model of health care, historically curative and hospital-centered, by a model in line with Principles of the Unified Health System (SUS)1,2. The FHS has as characteristics the clientele's ascription, focus in the family, structuring of a multidisciplinary team, preventive health action, detection of population needs and multidisciplinary performance for the promotion of health2.
Although it is recognized that there are different degrees of implementation of FHS in the different localities of the country, evaluations have been showing good results in terms of coverage and positive effects on morbidity and mortality rates1-4. However, technical and physical limitations related to the capacity of providing the expected comprehensive care have also been pointed out3,4.
Since the Sanitary Reform, the multidisciplinary teamwork has been highlighted in health policy, based on the interdependence and complementarity of the actions developed by various health workers. The multidisciplinary performance presupposes collective activity, cooperation in the elaboration and execution of technical interventions, allowing considering the subjects in their integrality. It establishes, therefore, the requirement of professionals with knowledge, skills and attitudes that allow the necessary changes in the organization of the services - teamwork, shared competences and humanization in service5.
Food and nutrition, as basic requirements for promotion and protection of health, were fully consolidated in the operational plan of SUS, in 1990, with Law 8.080, and it is affirmed in the historical process of the National Food and Nutrition Policy6,7. On the occasion of the III National Conference on Food and Nutrition Safety, in 2007, it was verified the need to strengthen the actions of food and nutrition at all levels of health care6. The provision of primary actions on food and nutrition in primary care, in a multidisciplinary way, and the qualified incorporation of the nutritionist are essential for compliance with the principles of comprehensiveness, universality and solubility of health care5.
Actions on food and nutrition in the context of primary health care, particularly in the FHS, play a fundamental role due to the growing demands of health care arising from the current epidemiological situation in Brazil, represented by a load of determinants: an unfinished agenda for combating infections, malnutrition and reproductive health problems; the challenge of chronic diseases and their risk factors, such as smoking, overweight, obesity, physical inactivity, stress and poor diet; and the continuous growth of external causes of morbidity and mortality7 . Such profile requires a deep reflection that indicates the need for changes in the perspective of social determination of health and feeding8,9.
The present study, considering the scarcity of publications focusing on food and nutrition in the context of FHS10, had the objective of characterizing the actions of food and nutrition in the scope of FHS, by analyzing the structure and the work process.
LITERATURE REVIEW
Among the models of evaluation of health services, the one developed by Donabedian stands out. This model suggests, among other variables, that good structural conditions are indispensable for a good process, which leads to better outcomes. In this sense, structure refers to the relatively stable material and organizational material that provide assistance. Process, in turn, refers to the doing in the exercise of such assistance11-13.
In this sense, the nurse is an important member of the basic multidisciplinary team in the FHD, being an active link in the process of consolidating the strategy as an integrative and humanizing health policy. In addition, the nurse has great importance in the multidisciplinary health team, in the context of FHS, for their attributions, such as supervision of the activities of other professionals (community health workers and nursing assistants) and expected skills in relation to leadership and management14,15.
METHODOLOGY
This study is part of the research entitled Primary health care (PHC) in the city of Campina Grande, Paraiba: evaluation of the performance and effectiveness of family health strategy and the incorporation of food and nutrition actions . It is a cross-sectional study that uses two-level measures (structure and process).
The study was carried out in the municipality of Campina Grande, Paraiba, between June and December 2010. The municipality was chosen because it has a geographically delimited area with basic family health units (BFHU), a reasonable historical tradition of organizing PHC services, and partnership between academia and health managers/teams. Campina Grande is the second largest municipality in the state, with a population of 376,060 inhabitants, a pioneer in the implementation of the FHP in 199416. At the time of the research, it had a health system composed of six health districts with 67 BFHUs, covering 71% of the population17.
The collection unit was the BFHU, regardless of the number of teams. 20 (29.85%) of the UBSF of the municipality were studied. These were selected according to three parameters of choice: location in areas of the city with a similar socioeconomic situation, being considered of good relative standard of service, having low turnover of workers. The draw was random, considering the division by sanitary districts in order to represent the different geographical spaces/areas of the city.
The FHS has the nurse as an important member of the basic multidisciplinary team18. In the city of Campina Grande, this group represents 41.81% of the higher-education professionals (dentists - 40, physicians - 88, nurses - 92) of the basic team working in the UBSF. Thus, to represent the health professionals, a nurse, randomly selected, was interviewed in each unit to obtain some characterization data.
The evaluation of health services addressed two dimensions, structure and process. Information on structure was obtained by using a standardized questionnaire with closed questions and answered individually by the nurses. It comprised questions about the composition of the team (human resources), anthropometric equipment, protocols to guide feeding and nutrition actions, stocks for oral supplementation and rehydration, and posters for educational purposes on feeding issues.
Information on the work process was obtained by using two instruments. Firstly, a collective instrument was used with open questions related to the development of food and nutrition actions (promotion of healthy eating, nutritional follow-up of pregnant women, nutritional monitoring of children assisted under the Program to Combat Nutritional Deficiencies and within the Food and Nutrition Surveillance System/Bolsa Família Program), which was answered at a meeting of the health unit team. The second instrument, with closed questions, addressed the food and nutrition educational activities developed by nurses, as well as the accomplishment of the food and nutritional diagnosis of the assisted population by the health team.
Data from each BFHU was organized into Office Excel spreadsheets (Microsoft Inc., United States). Tabular analysis was performed, and the frequencies for each variable were calculated. The data were processed and analyzed by using the R software (CORE TEAM, 2014).
Interviews were conducted after obtaining informed consent of the subjects, according to a specific term, which ensured anonymity. This study was approved by the Research Ethics Committee of the State University of Paraiba (opinion No. 0355013300009) and obeyed the research ethical principles according to Resolution 196/1996 of the National Health Council.
RESULTS
Twenty (100%) nurses were interviewed, of whom 19 (95%) were females with a mean age of 34.5 years (SD = 8.7 years). All the nurses entered the position through a public tender, and when questioned about the satisfaction with the employment relationship, 19 (95%) aswered positively. The majority, 17 (85%), did not receive salary incentive by the municipality, and 11 (55%) did not carry out other professional activities. Considering the training, it is noteworthy that 16 (80%) had specialization and only 4 (20%) had master's degree.
Regarding the composition of the teams, it was observed that all had physicians, nurses, nursing assistants and community health workers. Of the 20 (100%) teams, 12 (60%) had dentists and dental assistants. The nutritionist was not part of any of the teams, and in all of them, physicians or nurses were referred to as the professionals who do the main activities related to food and nutrition issues.
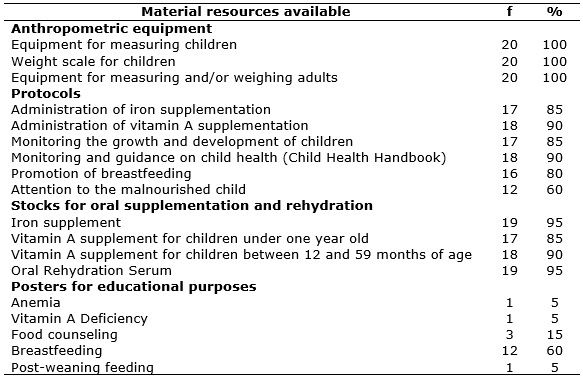
Considering the evaluation items of structure, the anthropometric instruments were the most complete, followed by the stocks for supplementation and oral rehydration, as shown in Table 1.
TABLE 1: Material structure resources related to food and nutrition available in
the basic family health units of the city of Campina Grande, Paraiba, 2010
(N=20).
Attention and care protocols related to food and nutrition area and posters for nutritional education purposes were characterized with less availability. According to the results, except for the malnutrition care protocol, all items that were unavailable in at least 5 (25%) of the units were those related to educational purposes through posters; 1 (5%) single unit had posters exposed on post-weaning diet, anemia and vitamin A deficiency; posters on breastfeeding and food counseling were exposed in 12 (60%) and 3 (15%) of the units, respectively.
As regards the work process developed in the BHU, health promotion activities were performed in 13 (65%) of the units, whereas nutritional support activities for people with obesity, diabetes and hypertension were developed in 12 (60%). The nutritional monitoring of pregnant women, the nutritional monitoring of children, activities under the Program to Combat Nutritional Deficiencies and activities under the Food and Nutrition Surveillance System/Bolsa Família Program were carried out in 14 (70%) of the units.
Considering the main difficulties and suggestions for the performance of activities, the physical structure was pointed out as the main obstacle, and the decrease of demand as the main parameter to be reached for the appropriate professional exercise. Problems of material resources (didactic material/forms/supplements in inadequate quantity and/or quality), overwork, including bureaucratic work, and the socioeconomic situation of the population were also mentioned as important difficulties for the development of most actions. To improve performance, the following things were suggested: professional training, availability of nutritionists and awareness/acceptance of the population.
Regarding the population diagnosis of the food and nutritional situation, eight nurses indicated that their teams do not perform this action. In the diagnosis, the aspects treated in 10 or more of the units, in descending order, were the morbidity and mortality indicators, the sanitation conditions, the geographic characterization, the identification of vulnerable groups and the analysis of the programs and activities developed. Nurses, the minority, reported the inclusion of the following items in the diagnosis performed by the team: action plan, critical evaluation of the situation found, socioeconomic indicators, demographic indicators, nutritional indicators.
Regarding the educational activities on feeding and nutrition developed by the nurses, it is observed that the guidelines on breastfeeding up to two years old and on the feeding of children constituted the two activities less accomplished, as shown in Table 2. Activities on feeding during pregnancy and healthy eating practices were performed by 16 (80%) of the nurses; and about exclusive breastfeeding up to six months of age were performed by all nurses.
TABLE 2: Themes of educational activities related to food and nutrition developed
by nurses of the basic family health units of the city of Campina Grande,
Paraiba, 2010 (N=20). 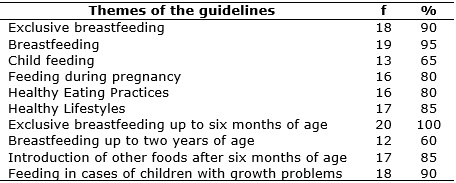
DISCUSSION
Despite the lack of studies on the subject, other researches, such as the present one, also revealed that physicians and nurses have carried out the main approaches of feeding and nutrition in the FHS18-20. In Brazil, the undergraduate training of physicians and nurses lacks information that enables them to work in the area of nutrition21. It is also reduced the number of FHS physicians and nurses with stricto sensu training in the area of public health, which could help to solve the problem21,22. Still, this problem becomes more intense when considering the training and practices of the fragmented, technical and healing-focused model that permeates the work of these professionals23-25.
These are elements that can lead to problems in addressing food or nutrition issues or their omission. In this study, the difficulties encountered when inquiring the health team and the nurses were similar to those described with professionals from different health areas of other localities18-20,26,27. It refers to the demand for nutrition training linked to the deficiency of knowledge, as well as to the importance attached to nutritional education18,19,26-28.
With respect to actions to promote health and healthy eating that can be developed by physicians, nurses and other health professionals, it is noteworthy to express that these can be strengthened with the guidelines of the food guides: Food Guide for the Brazilian Population29 and Food Guide for Brazilian children under two years of age, recently revised and summarized 30. As part of the Program to Combat Nutritional Deficiencies, it is hoped that the professionals of the FHS teams will potentiate this action, encouraging, through food and nutritional education, the consumption of fortified foods (iodized salt and flours with iron and folic acid)7. For nutritional support for people with obesity, diabetes and hypertension, primary health care professionals can use the Primary Care Book No. 12, directed to the organization of care for the overweighed patient31. In addition, the deficient structure of Campina Grande in relation to the availability of posters for educational purposes in relation to priority programs in the area of food and nutrition of the Ministry of Health, such as the National Program for Supplementation of Iron and the National Program for Supplementation of Vitamin A, shows that the effective implementation of these programs within the scope of the FHS is still a major challenge for managers and professionals in the municipality. The educational material to support the practice related to these programs is available on the website of the General Coordination of Food and Nutrition.
Other obstacles to the performance of nutrition approaches, mentioned by FHS professionals from the city of Campina Grande, were also recorded in different studies, such as lack of time/overwork/high demand18,28, the unfavorable socioeconomic situation of the population27,28 and the difficulty in achieving adherence/acceptance to the guidelines18,28. It is again perceived a lack of qualification, since the lack of adherence of the clientele may reflect inadequate approaches to the view of patients as active participants32.
In this sense, and considering the relevance of the socioeconomic situation, it is necessary to emphasize the need for a broad understanding of the problems experienced by the community in the model of the social production of nutritional and health status, which makes the issue of qualification not only an indispensable connection to specific knowledge in nutrition, but also to the knowledge of educational strategies. This is a challenge for all FHS professionals who have the same responsibility in educational practices. On the other hand, it should also be considered that the diagnosis of the food and nutritional situation is an essential tool for planning and supporting the actions of food and nutrition.
Finally, the difficulties of professionals to work on the themes of food and nutrition refer to the need for inserting the nutritionist in the FHS team. When studying the perception among health professionals from different areas, the interviewees from the city of Vitoria de Santo Antao, (PE)28 pointed out the need of including the nutritionist in the FHS, from the core of minimum team, without prejudice to their inclusion in the Family Health Support Center (NASF in Portuguese). A similar result was observed when studying health professionals in five municipalities representing each region of the country27. However, in the municipality of Sao Carlos (SP)18, while some professionals reported that it is important and necessary to include the nutritionist in the minimum team, others have shown the opposite. The latter argue that the work of other professionals could meet the nutritional needs of the population if they were trained to deal with their patients in a broader way, including specific knowledge of nutrition, and that it is unnecessary for the nutritionist to work full-time in health units.
It should be noted that the need for incorporating the nutritionist in the FHS teams is based on the fact that the absence of this professional is against with the principle of comprehensiveness of health actions, since no other health professional has training to work in the area feeding and nutrition within communities with important contributions in promoting the health of the population33. The importance of the participation of the nutritionist and their integration in the health teams are established in their academic training that enables them to carry out the nutritional diagnosis of the population and propose the appropriate dietary guidelines to this profile and to the family reality34. The nutritionist is the trained professional and legally qualified for such action6,35. In this context, food and nutritional surveillance stands out as an action that constitutes, in municipal management, the basis for the formulation and implementation of public policies 6.
It is worth emphasizing that the legal framework for the training of the nutritionist guarantees the effective insertion of this professional in the SUS, based on three concepts: training in the primary objectives of SUS (promotion, maintenance and recovery of health); formation of general competencies and abilities similar to the other health professionals (health care, decision-making, communication, leadership, administration and management, permanent education), highlighting the possibility of insertion in all three levels of care; formation of specific skills and abilities important for SUS actions. The role of the nutritionist in PHC is established in two dimensions, the management and care of food and nutrition actions6.
However, the absence of the nutritionist in the family health team has been attributed to factors such as political will, lack of financial resources, low social recognition, professional devaluation and representations that managers build regarding their professional performance19,37. In this context, research has pointed out that, in contrast to the increase in the number of nutritionists in Brazil, there has been a historical maintenance of a low percentage of professionals working in the area of Nutrition and Public Health, in which PHC is inserted35,36.
The creation and consolidation of NASFs constitute, in the previous conjuncture, an odd opportunity to change this situation. With the insertion of the nutritionist in the NASF teams, the actions of feeding and nutrition in the PHC have been strengthened through the management and interdisciplinarity of the actions7. This may be the ideal space to generate a greater knowledge about the core competencies of the nutritionist and to understand the need to insert them in the NASF and/or the BFHS teams. Together with other health professionals, who work in the hospital and outpatient clinic spaces, the participation of the nutritionist is important in the project of transforming the history of health in Brazil, in a process that encourages work in a multidisciplinary team, able to conceive health in its collective dimension, as stated in the official speech of the HFP, when referring that it is not focused on medical work, but on a multidisciplinary team, in which all knowledge must be respected38. The importance of integrated team actions in the FHS context has also been pointed out in previous research, including regarding the role of nurses in food and nutrition actions, which was highlighted as a major challenge25,38,39.
CONCLUSIONS
Physicians and nurses are the professionals who carry out the main activities of food and nutrition in the scope of primary health care. The development of feeding and nutrition actions in the FHS is hampered by structural problems such as the lack of educational materials and lack of population adherence. It is important to emphasize the importance of professional qualification, considering that many professionals do not work on basic themes such as promotion of health and healthy eating, as well as in the diagnosis of the food and nutritional situation. The development of food and nutrition actions in primary care needs a nutritionist who works with the support of a multidisciplinary team.
This study presents limitations due to its spectrum related to the study site - it investigates the reality of only one municipality, preventing the generalization of the results. Also, the descriptive characteristic and the way of obtaining the information prioritized the answers of the professionals and there is the possibility of information bias.
REFERENCES
1.Henrique F, Calvo MCM. Avaliação do Programa Saúde da Família nos municípios do Estado de Santa Catarina, Brasil. Cad Saúde Pública. 2008; 24(4):809-19.
2.Gomes KO, Cotta RMM, Euclydes MP, Targueta CL, Priore SE, Franceschini SCC. Avaliação do impacto do Programa Saúde da Família no perfil epidemiológico da população rural de Airões, município de Paula Cândido (MG), 1992-2003. Ciênc Saúde Colet. 2009; 14(Supl 1):S1473-82.
3.Almeida PF, Giovanella L. Atenção Primária Integral à Saúde: indicadores para avaliação. Rio de Janeiro: FIOCRUZ; 2011.
4.Almeida PF, Fausto MCR, Giovanella L. Fortalecimento da atenção primária à saúde: estratégia para potencializar a coordenação dos cuidados. Rev Panam Salud Publica. 2011; 29(2):84-95.
5.Ministério da Saúde (Br). Matriz de ações de alimentação e nutrição na atenção básica de saúde. Brasília (DF): Ministério da Saúde; 2008.
6.Lang RMF, Rivas MGTO. O nutricionista e as ações de nutrição em saúde. In: Taddei JA, Lang RMF, Longo-Silva G, Toloni MHA, editores. Nutrição em Saúde Pública. Rio de Janeiro: Editora Rubio; 2011. p. 437-53.
7.Jaime PC, Silva ACF, Lima AMC, Bortolini GA. Ações de alimentação e nutrição na atenção básica: a experiência de organização no Governo Brasileiro. Rev Nutr. 2011; 24(6):809-24.
8.Ferreira VA, Magalhães R. Nutrição e promoção da saúde: perspectivas atuais. Cad Saúde Pública. 2007; 23(7):1674-81.
9.Gomes RCF, Fagundes AA, Pinheiro ARO, Teixeira BA, Sousa JS, et al. A formação em saúde pública nos cursos de graduação de nutrição no Brasil. Rev Nutr. 2012; 25(1):21-33.
10.Vasconcelos IAL, Santos LMP. Research potential of food and nutrition in the Family Health Strategy: A structured review. Rev Nutr. 2014; 27(1):107-26.
11.Donabedian A. The quality of care – how can it be accessed? JAMA. 1988; 260:1145-50.
12.Niquini RP, Bittencourt SA, Lacerda EMA, Saunders C, Leal MC. Avaliação da estrutura de sete unidades de saúde da família para a oferta da assistência nutricional no pré-natal no município do Rio de Janeiro, Brasil. Rev Bras Saúde Matern Infant. 2010; 10(Supl 1):S61-8.
13.Moura BLA, Cunha RC, Fonseca ACF, Aquino R, Medina MG, VilasBôas ALQ et al. Atenção Primária à Saúde: Estrutura das Unidades Como Componente da Atenção à Saúde. Rev Bras Saúde Matern Infant. 2010; 10(Supl 1):69-81.
14.Silva VG, Motta MCS, Zeitoune RCG. A prática do enfermeiro na Estratégia Saúde da Família: o caso do município de Vitória/ES. Rev Eletr Enf. 2010; 12(3):441-8.
15.Barbosa RC, Lorenzini E, Bazzo K, Silva EF. Liderança do enfermeiro na estratégia saúde da família: revisão integrativa. Revista Eletrônica Gestão & Saúde. 2013; 4(2):428-38.
16.Secretaria Municipal de Saúde de Campina Grande (Pb). Programa Saúde da Família: projeto de implantação. Campina Grande (PB): Secretaria Municipal de Saúde de Campina Grande; 1994.
17.Ministério da Saúde (Br). [site de Internet]. Cadastro Nacional de Estabelecimentos de Saúde – CNES. [cited 2016 June 29]. Available from: http://cnes.datasus.gov.br/Mod_Ind_Unidade_Listar.asp?VTipo=02&VListar=1&VEstado=25&VMun=250400&VSubUni
18.Camossa ACA, Telarolli Junior R, Machado MLT. O fazer teórico-prático do nutricionista na estratégia saúde da família: representações sociais dos profissionais das equipes. Rev Nutr. 2012; 25(1):89-106.
19.Boog MCF. Dificuldades encontradas por médicos e enfermeiros na abordagem de problemas alimentares. Rev Nutr. 1999; 12(3):261-72.
20.Pádua JG, Boog MCF. Avaliação da inserção do nutricionista na Rede Básica de Saúde dos municípios da Região Metropolitana de Campinas. Rev Nutr. 2006; 19(4):413-24.
21.Machado MH. Perfil dos médicos e enfermeiros do Programa Saúde da Família no Brasil: relatório final. Brasília (DF): Ministério da Saúde; 2000.
22.Gil CRR. Formação de Recursos Humanos em saúde da família: paradoxos e perspectivas. Cad Saúde Pública. 2005; 21(2):490-8.
23.Mulato SC. Enfermagem tradicional, atual e do futuro: a visão de docentes de enfermagem. Rev enferm UERJ 2010; 18(4):572-7.
24.Cursino EG, Fujimori E. Integralidade como uma dimensão das práticas de atenção à saúde da criança: uma revisão bibliográfica. Rev enferm UERJ 2012; 20(5):676-80.
25.Gonçalves RJ, Soares RA, Troll T, Cyrino EG. Ser médico no PSF: formação acadêmica, perspectivas e trabalho cotidiano. Rev bras educ med. 2009; 33(3):393-403.
26.Saparolli ECL, Adami NP. Avaliação da qualidade da consulta de enfermagem à criança no Programa de Saúde da Família. Acta Paul Enferm. 2007; 20(1):55-61.
27.Sousa MF, Hamann EM, Mendonça AVM. Alimentação e nutrição na Estratégia Saúde da Família em cinco municípios brasileiros. Ciênc Saúde Colet. 2014; 19(1):49-57.
28.Costa KAO, Santana PR. A importância e o papel do nutricionista na Atenção Básica em Vitória de Santo Antão / PE. Tempus - Actas Saude Colet. 2011; 5(4):67-85.
29.Ministério da Saúde (Br). Guia alimentar para a população brasileira: promovendo a alimentação saudável. Brasília: Ministério da Saúde; 2006.
30.Ministério da Saúde (Br). Dez passos para uma alimentação saudável: guia alimentar para menores de dois anos: um guia para o profissional da saúde na atenção básica. Brasília (DF): Ministério da Saúde; 2010.
31.Mistério da Saúde (Br). Obesidade: caderno de atenção básica número 12. Brasília (DF): Ministério da Saúde; 2011.
32.Pontieri FM, Bachion MM. Crenças de pacientes diabéticos acerca da terapia nutricional e sua influência na adesão ao tratamento. Ciênc Saúde Colet. 2010; 15(1):151-60.
33.Geus LMM, Maciel CS, Burda ICA, Daros SJ, Batistel S, Martins TCA, et al. A importância na inserção do nutricionista na Estratégia Saúde da Família. Ciênc Saúde Colet. 2011(Supl 1); 16:797-804.
34.Mattos PF, Neves AS. A importância da atuação do nutricionista na Atenção Básica à Saúde. Práxis. 2009; I(2):11-5.
35.Vasconcelos FAG. A inserção do nutricionista no Sistema Único de Saúde. In: Taddei JA, Lang RMF, Longo-Silva G, Toloni MHA, editores. Nutrição em Saúde Pública. Rio de Janeiro: Editora Rubio; 2011. p. 423-35.
36.Boog MCF. Atuação do nutricionista em saúde pública na promoção da alimentação saudável. Cienc Saude. 2008; 1(1):33-42.
37.Ministério da Saúde (Br). Abrindo a porta para dona saúde entrar: uma estratégia para a reorganização do modelo assistencial. Brasília (DF): Ministério da Saúde; 2000.
38.Ribeiro SP, Oliveira DS, Fernandes SLSA, Felzemburgh RDM, Camargo CL. O quotidiano de enfermeiras na consulta em puericultura. Rev enferm UERJ 2014; 22(1):89-95.
39.Monteiro AI, Santos ADB, Macedo IP, Gurgel PKF, Cavalcante JMP. A expressão da autonomia do enfermeiro no acompanhamento do crescimento e desenvolvimento da criança. Rev enferm UERJ 2011; 19(3):426-31.