(*) Mann-Whitney Test
RESEARCH ARTICLES
Psychometric properties of the Brazilian version of the Work Role Functioning Questionnaire evaluating workers in radiotherapy
Cristiane Helena GallaschI; Neusa Maria Costa AlexandreII; Sergio Carlos Barros EstevesIII
I
Registered Nurse, Ph.D. - Nursing. Adjunt Professor of the Department of Medical-Surgical Nursing – Faculty of Nursing at the Rio de Janeiro State
University. Rio de Janeiro, RJ, Brazil. E-mail: cristiane.gallasch@gmail.com
II
Registered Nurse, Ph.D. - Nursing. Associated Professor of the Faculty of Nursingat the State University of Campinas. Leader of the Study and Research
Group in Labor and Ergonomy Health. Campinas, São Paulo, Brazil. E-mail: nmca@unicamp.br
III
Radio-oncologist, MD, Ph.D. - Radiology. Coordinator of the Radio-oncology Section in the Women´s Hospital Professor Doctor José Aristodemo Pinotti – CAISM
of the State University of Campinas. São Paulo, Brazil. E-mail: estevesrt@uol.com.br
IV
The authors thanks for the Coordinator of Improvment of Higher Education Personel (CAPES) support for this research.
DOI: http://dx.doi.org/10.12957/reuerj.2015.15791
ABSTRACT
Chronic disorders, including cancer, are a public health problem, causing worker incapacity, absenteeism, resignation and dismissal. This study examined the psychometric properties of the Brazilian version of the Work Role Functioning Questionnaire (WRFQ-Br) in workers with neoplasms undergoing radiotherapy in up-state São Paulo. Psychometric properties were evaluated in 51 subjects with cancer diagnoses undergoing radiotherapy between 2011 and 2012, and 105 healthy workers. The results indicated good internal consistency (Cronbach alpha = 0.77-0.93). Construct validity displayed significant differences (p<0.05) between groups in output, and mental and social demands. Convergent validity analysis revealed a relation between the WRFQ-Br and the Karnofsky scale. Data showed that WRFQ-Br demonstrated reliable psychometric properties for evaluating workers with cancer diagnoses in Brazil.
Keywords: Cancer; reproducibility of results; work capacity evaluation; occupational health nursing.
INTRODUCTION
Chronic conditions like cancer, musculoskeletal disorders, arthritis, cardiac and neurological diseases represent a major public health problem, causing functional and biopsychosocial limitations, absenteeism, removal from work activities and reducing the quality of life performances1-5.
Currently, about 12% of deaths in the world are related to cancer, being about seven million people. Eleven million new cases of cancer per year are reported, with increasing prevision to 27 million by 2030, with 17 million deaths and 75 million people alive, according estimated by the Health World Organization6. Increasing the number of new cases is directly related to the increase in life expectancy of the population and exposure to risk factors7. Approximately 50% of cases occur in developing countries like Brazil, where 576,000 new cases are expected to 2014 and 2015 6,7.
Like other chronic diseases, cancer has become frequent and increasingly common, leading instability to families when the head of the family gets ill, when he is the only source of income provider6. The cancer survival should be considered relevant in the treatment because due to the increase in its incidence, it is necessary to prevent the challenges that come forward to living with a diagnosis of cancer. These survivors complete a primary course of treatment, and there is a need to move on with their lives8.
Limitations to can are found up to 11 years after diagnosis and early treatment9. The evaluation of patients with brain cancer, using the Work Limitations Questionnaire (WLQ) found restrWAIions related to fatigue, depression, anxiety and cognitive loss10. Similar signs and symptoms, except cognitive changes, were found in a study involving patients with thoracic cancer, even four years after diagnosis and treatment11. Residual symptoms after chemotherapy and radiation cause direct impact on return to work12.
Researches involving the limitations on work related to treatment and cancer survival are recent, presented in the international literature from 2000. Professionals of occupational health and oncology need information and skills that will bring changes in work environment and development of actions to improve these pWAIures and to favor the return to work10.
Considering the satisfactory results after the cross-cultural adaptation and evaluation of validity and reliability of the Work Role Functioning Questionnaire adapted ad validated for Brazil (WRFQ-Br) for people with musculoskeletal disorders, the aim of this study was to evaluate the psychometric properties of the same tool for workers diagnosed with cancer undergoing radiantion therapy, which kept or returned to work activities during or after treatment.
LITERATURE REVIEW
Researchers and health professionals are increasingly concerned with using reliable and appropriate scales and questionnaires for specific population 13,14. The validity and reliability are particularly important when selecting instruments to be used in research and clinical practice. However, it is important to note that these data are not static qualities of an instrument. The best is to reassess these properties whenever changing the evaluated population14,15.
The use of validated instruments has been considered essential for the reliability of data obtained from individuals with physical difficulties or psychosocial changes. Reliable data help in the planning of these disorders prevention actions and planning strategies and rehabilitation programs in the area of occupational health.
The WRFQ-Br, with satisfactory results of validity and reliability, emerges as a potential tool for overall assessment of the worker diagnosed with cancer, considering that one of the questionnaires that gave rise to it has been used in a study involving brain cancer10,16.
Due to recent research demonstrating aspects of increased cancer survival and the need for planning the return to work, during and after treatment, this population is suitable for the development and improvement of health assessment tools. Also, questionnaires related to the evaluation of performance or capacity at work and cancer survival are not available for the Brazilian population.
The theoretical reference used in this study is the Psychometrics, based on verification standards and evaluation of psychometric properties of measurement instruments established by the Consensus-based standards for the selection of health status measurement instruments (COSMIN)17.
METHODOLOGY
This is a methodological study following the international recommendations for evaluation of the psychometric properties of WRFQ-Br for individuals diagnosed with cancer undergoing radiation therapy, according to the theoretical reference mentioned.
The study included two groups. The first group consisted of individuals diagnosed with cancer undergoing radiation therapy in a specialized private center. The second group consisted of workers of a technological development center without complaints related to health, all in the state of São Paulo.
The inclusion criteria for subjects with cancer were aged between 18 and 75 years old, with diagnosis confirmed by pathological examination, completion of the radiantion therapy protocol, in teletherapy mode, with exposure to at least a low dose of 2000cGy, completion of radiation therapy protocol for a maximum of two years, maintenance of work activities, formal or informal, with a minimum workload of 20 hours per week16,18-21. The same criteria of age, work activities, weekly working hours, as well as the lack of health-related complaints were considered as criteria for inclusion of healthy workers. Exclusion criteria were patients performing exclusive radiantion therapy of brachytherapy protocol mode, and being illiterate for both groups.
During data collection, patients admitted in 2011 and 2012 answered the WRFQ-Br independently in the center of care in radiation therapy, or at home, with forms sent by post, according to the participant's choice. Workers without health-related complaints completed the questionnaires at work independently, without the influence of professionals of the occupational health service.
The study protocol was submitted to the Ethics Committee in Research of the State University of Campinas School of Medical Sciences and obtained assent under #104/2009 on November, 24th 2009. All study participants received and signed the free and clear consent form.
The instruments used and the expected data analysis are described below, and the discussion was guided by the literature1-17,22-33.
Data collection instruments
A form, based on previous research was used16, adapted specifically for this study to survey the socio-demographic identification and clinical data. The type of work has been described according to the classification of Hébert22.
The WRFQ is originated from the WLQ and Work Limitations instruments - 26 Items (WL-26)21. The purpose of these instruments is to assess if the ability to work is impaired due to health problems related to chronic diseases, causing impacts or limitations in daily work activities21,23. In 2007, the WRFQ was validated, and the results confirmed that the procedures for cultural adaptation of this tool for the Brazilian version in evaluating individuals with work-related musculoskeletal disorders (MSDs) were performed properly16.
The WRFQ-Br includes five subscales, or evaluation demands: scheduling, assessing worker difficulties to plan and managing their daily work activities from beginning to end of the working day; output demand, including productivity, quality of service and job satisfaction; physical demand, measuring ability to perform work activities, including physical, static and dynamic workloads such as heavy objects, movements, resistance, coordination and flexibility; mental demand, contemplating the cognitive demands related to attention and concentration; and social demand, referring to the interactions that the individuals should accomplish with their co-workers and patients in their service16.
The KPS is a system of evaluating the clinical status of the patient, which is part of the consultation and systematic registration carried out by professionals in the health of patients evaluated in oncology. It is used to quantify the welfare and activities of the overall daily life of cancer patients and allows patients to be classified according to their functional impairment. It ranges from 100 to 0 and 100-90 classified as asymptomatic or have minimal symptoms, 89-70 symptomatic, but ambulatory capacity attendance, 69-50 stay in bed, at least, half of the day, 49-30 remain in bed most of the half the day, 29-10 bedridden, requiring constant care and less than 9, agonized patient24,25.
The WHOQOL-Bref, or WHOQOL-abbreviated, assesses general aspects of quality of life, including physical, psychological, social and environmental demands. It was developed based on the WHOQOL-100, used by the Health World Organization, and with satisfactory results in the evaluation of its psychometric properties for the Brazilian population26.
The Work ability index (WAI) is a self-administered questionnaire used in the daily practice of occupational health care, to assess the work capacity of an individual through his perception, with issues that include the physical and mental demands of work, health status and resources of the worker 27,28.
Data analysis
The data were entered into the database and analyzed descriptively by absolute (n) and relative (%) frequencies for categorical variables. For continuous variables, average, standard deviation, first and third quartiles, maximum and minimum values were used. To help in the organization, classification and data analysis, the computer software Microsoft Office Excel 2007, SAS version 9.2 - Cary, NC, USA: SAS Institute Inc., 2008 and R-project 2.15.0 was used.
Reliability was evaluated by internal consistency, examining whether all subparts of an instrument or a scale measure the same characteristic was verified by the Cronbach's alpha4,21,33,34. It was established as evidence of satisfactory internal consistency value of Cronbach's alpha> 0,70 19,33-35. The procedure was performed for each question about the whole and for each question about the domain to which it belongs.
The construct validity was verified by the approach of the groups, comparing workers with cancer with a population of workers without complaints related to health. Differences between groups were expected and may be identified by scores of 18-20. For comparisons between patients and healthy people the nonparametric Mann-Whitney was used, and to evaluate the convergent validity, the Spermann coefficient was used, including scores up to 0.30 as satisfactory, between 0.31 and 0.50 as moderate and above 0.51 as strong magnitude28.
Convergent validity was assessed by correlating the scores obtained in the evaluation of the working population diagnosed with cancer using the WRFQ-Br scores, comparing it to other instruments that assessed the same constructs, KPS, WAI and the Whoqol-Bref.
RESULTS
Subjects' characterization
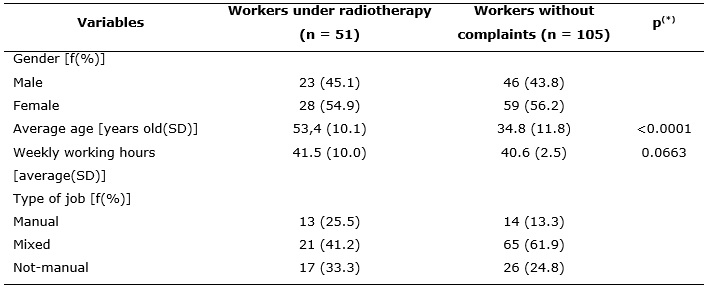
The first group included 51 subjects with a diagnosis of cancer, treated with radiation therapy, users of a private outpatient radiation therapyy center in the state of São Paulo. The second study group comprised 105 subjects without health-related complaints, who were selected from workers from a technology development center. The socio-demographic characteristics of this population are described in Table 1.
TABLE 1:
Socio-demographic characteristics of workers under radiotherapy and healthy individuals. Campinas, SP, 2013. (N = 162).
(*)
Mann-Whitney Test
It is observed a statistically significant difference between the average ages of the groups with the older population among patients, which was expected when studying cancer, found most commonly in the elderly. Both groups have the most workers in mixed work activities, a characteristic observed in the previous studies16. There was no significant difference between groups in the evaluation of the number of hours worked per week.
The most common cancer diagnoses in the group of patients (n=51) were prostate (23.53%) and breast cancer (45.10%). The medical dose of radiantion therapy at the time of data collection was 5664cGy (+117.1).
Concerning to the Karnofsky Scale, there were scores of 80 (19.61%) 90 (17.65%) and 100 (62.75%) among patients.
Evaluation of psychometric properties
The instrument showed adequate values for internal consistency in the assessment of reliability. The overall Cronbach alpha coefficient obtained value of 0.93, indicating the high precision measurement. The assessment of each subscale showed greater accuracy for work plan (0.93) and lower for physical demand (0.77).
The evaluation of the construct validity was performed by differentiation between workers with diagnoses of cancer undergoing radiantion therapy and workers without complaints related to health or diagnosis of cancer. It may also be called the approach contrasted groups, and it is shown in Table 2.
TABLE 2:
WRFQ-Br average scores in workers with cancer undergoing radiotherapy (n=51) and workers without health-related complaints (n=105). Campinas, SP, Brazil,
2013.
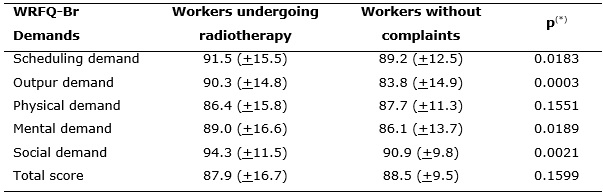
(*)
Mann-Whitney Test
Statistically significant differences were observed between the groups related to production, mental and social demands. There were no significant differences related to the physical demands and work plan, as well as for the total score. The results of WRFQ-Br instruments, KPS, Whoqol-Bref, and WAI, used to evaluate the convergent validity, are shown in Figure 1.
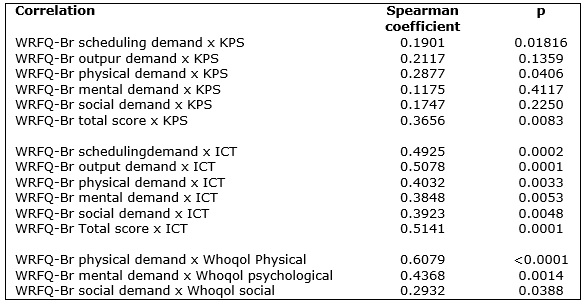
FIGURE1:
Correlations between WRFQ-Br with KPS, ICT and Whoqol-Bref. Campinas, SP, Brazil, 2013.
In the evaluation between the WRFQ-Br and KPS, there were correlations with the physical demands WRFQ-Br and the total score (p <0.05). Comparing WRFQ-Br and WAI, correlations were found between all the demands and the total score of both instruments (p <0.05). The same was observed when comparing the physical demands WRFQ-Br X Whoqol physical, mental WRFQ-Br X Whoqol psychological and social WRFQ-Br X social Whoqol (p <0.05).
DISCUSSION
This study started from the observation of complaints from patients undergoing radiation therapy away from their usual work activities, expressing a desire to keep them, for to experience the satisfaction of productivity, living in their friendship circles, and to keep thinking on different issues from those of treatment and prognosis.
The return to work of cancer survivors´ individuals has been reported as problematic due to changes in physical function, fatigue, lack of support and adaptations in the workplace, as well as work overload36.
Since industrial development, with changes in the conception of the work and its execution, the workers began to experience long working hours, accelerated rhythms, physical fatigue, task divisions and reduction in sharing the production process, resulting in physical health and mental changes28.
Due to the high physical and mental demands at work, besides to long hours, there were observed large numbers of sick leave in the reality of oncology care. There were not patients rate statistics removed among all who have the disease, but this study observed 13.45% of the removal in cases, even after the proposed protocol. There were not data found on the form for assessing the ability of these individuals or attempts to adapt the work, with reduced overhead or journey, as ways to avoid the total removal of labor activities.
In Brazil, as observed in other regions of the world, the rise in survival rates and also healing after treatment in individuals of working age, increase the chances to stay or return to work activities. This rate of return varies according to the characteristics of each country support systems, including health systems, rehabilitation, and social assistance29.
In this study, there was a diagnostic feature that follows the same trend of Brazilian statistics, with the highest prevalence of prostate cancer for men and breast cancer for women6. In this group, the observation of the high level achieved in the Karnofsky scale, with an average of 94.31 (8.06) and most patients presenting score 100 (62.75%), is explained by the inclusion of patients who maintained work activities in this study. Values between 100 and 90 indicate individuals who have no symptoms or they are minimal. Scores 89 and 70 show that the patient is symptomatic, but with outpatient attendance capacity for treatment24,25. This indicates that individuals could have preserved capacity for certain activities, such as work. It should be noted that the values obtained indicate the average observed. However the clinical practice uses only decimal scores in the evaluation of health status (for example 70, 80, 90 or 100).
Evaluation of psychometric properties
The instrument presented adequate values for internal consistency. The total Cronbach's alpha coefficient had a value of 0.93, indicating the high precision measurement. In the assessment of each sub-scale, there was a higher accuracy for work plan (0.93) and lower for physical demand (0.77), but still higher than recommended as satisfactory38,39.
The cultural adaptation of the same instrument for the Canadian population with musculoskeletal disorders showed the lowest precision to the social demand (0.66), with higher Cronbach's alpha of 0.80 for the other sub-scales21. Recently the same instrument has been assessed and validated for the Dutch working population, with Cronbach's alpha coefficient calculated between 0.91 and 0.9636. The WL-26 questionnaire which led to WRFQ obtained during its validation process for people with occupational diseases and injuries in the United States, Cronbach's alpha values between 0.88 and 0.924.
The only correlation found between physical demand, and KPS scale is explained by the fact that the KPS scale refers to clinical symptoms and signs that refer to physical performance. There is no mention of social, mental or work activities25. The correlation between the total score of WRFQ-Br and KPS suggests a possibility of global evaluation of patients diagnosed with cancer also for this new instrument.
Comparing the WRFQ-Br and Whoqol-Bref, it was found a correlation with physical, psychological and social domains of WRFQ-Br, with different magnitudes between the evaluated items. It was a correlation with the measure of the quality of life-related to health, which strengthens the WRFQ-Br as trusted for evaluation of these aspects.
The Whoqol-Bref has been used for evaluation groups with different cancer diagnoses, with reliable results in these populations. Women are undergoing radiation therapy for the treatment of gynecological cancer, followed longitudinally, showed pain as an aspect that negatively influenced the physical, psychological and social fields37.
Women that are undergoing treatment for breast cancer often experiencing changes in behavior and coping strategies of disease and life, which leads to a search for live productive and a healthy way, with return initiatives to work, social activities, family proximity and involvement with religious beliefs 38. Some authors also mention that workers diagnosed with cancer have a more multidisciplinary intervention to facilitate the return to work to the general population39.
Compared to WAI, it was found a correlation with all the demands and the total score of WRFQ-Br, which ensures reliability in the workers´ performance evaluation. When grouped according to the categorization of WAI, individuals show differences in the demand for production and the total score of the Brazilian version of the Work Role Functioning Questionnaire. This is most evident among those categorized into moderate and great ability.
The possibility of detailed evaluation and accurately worker health, which was diagnosed and underwent treatment for cancer and can help to return to work, considering economic, productivity and interpersonal and social relations.
With the completion of new stages of evaluation of the psychometric properties of WRFQ-Br for workers undergoing radiation therapy, it is suggested to use it to better assess the health conditions of workers, the real needs of partial or total absences, the necessary adjustments to adapt the work environment and the implementation of effective rehabilitation programs and promotion of workers' health.
Limitation of the study was the small sample size (n=51), because of the number of removals from work activities, attended elderly (pensions) and deaths.
It is necessary for longitudinal studies that follow these patients from initial diagnosis, so there is the possibility performance assessment before the removal, during treatment and in planning activities and adjustments to return to work.
CONCLUSIONS
The study results confirm that the procedures for evaluation of the psychometric properties of WRFQ-Br instrument were carried out successfully by the recommendations of international literature.
The instrument showed Cronbach's alpha of 0.93 when fully analyzed, indicating a high precision measurement of internal consistency. In assessing the internal consistency of each question about its sub-scale, there were values between 0.77 and 0.93.
In the evaluation of construct validity by the known groups approach, there was a significant difference in items assessing production, mental and social demands (p <0.05). There was no significant difference in the physical and social demands. The hypothesis and mentioned in some publications is that the worker diagnosed with cancer receives largest multidisciplinary support for returning to work. It is still questioned if part of this population may not differ from the general population in some aspects of health assessment.
In assessing the construct validity through convergent approach, it was observed that the total score of WRFQ-Br were related to the contents of the Karnofsky scale, which may suggest a new tool for evaluation of workers with cancer but effective now considering global aspects of individuals, and not only physical symptoms.
There was a relationship with all the points raised by WAI and the physical, psychological and social domains of WHOQOL-Abbreviated with different magnitudes, enhancing the reliability of the WRFQ-Br for evaluation of functional aspects of the job and quality of life of individuals.
Thus, the WRFQ-Br showed good results in the evaluation of its psychometric properties and were considered reliable for its use in the population of workers diagnosed with cancer.
REFERENCES
1.Dall TM, Gallo P, Koenig L, Gu Q, Ruiz D. Modeling the indirect economic implications od musculoskeletal disorders and treatment. Cost Eff Resour Alloc. 2013; 11(5). Published online 2013 March 15. doi: 10.1186/1478-7547-11-5.
2.DiBonaventura MC, Gupta S, McDonald M, Sadosky A, Pettitt D, Silverman S. Impact of self-rated osteoarthritis severity in an employed population: Cross-sectional analysis of data from the national health and wellness survey. Health Qual Life Outcomes. 2012; 10(30). Published online 2012 March 15. doi: 10.1186/1477-7525-10-30.
3.Steiner JF, Nowels CT, Main DS. Returning to work after cancer: quantitative studies and prototypical narratives. Psychooncology. 2010; 19(2): 115-24.
4.Amick BC, Lerner D, Rogers WH, Rooney T, Katz J. A review of health-related work outcome measures and their uses, and recommended measures. Spine. 2000; 25: 3152-60.
5.Feuerstein M. Introduction: The world challenge of work disability. J Occup Rehabil. 2005; 15: 451-2.
6.Ministtry of Health (Br). Secretariat of Health Care. National Cancer Institute. Coordination of Cancer Prevention and Surveillance. Estimates 2008: Cancer Incidence in Brazil. Rio de Janeiro: INCA: 2007.
7. Ministry of Health (Br). Secretariat of Health Care. National Cancer Institute. The situation of Cancer in Brazil. Rio de Janeiro: INCA: 2006.
8.Feuerstein M. Defining cancer survivorship. J Cancer Surviv. 2007; 1: 5–7.
9.Yabroff R, Lawrence WF, Clauser S, Davis WW, Brwon ML. Burden of illness in cancer survivors: Findings from a population-based national sample. J Nat Cancer Inst. 2004; 96: 1322-30.
10.Feuerstein M, Hansen JA, Calvio LC, Johnson L, Ronquillo JG. Work productivity in brain tumor survivors. J Occup Environ Med. 2007; 49: 803-11.
11.Hansen JA, Feuerstein M, Calvio LC, Olsen CH. Breast cancer survivors at work. J Occup Environ Med. 2008; 50: 777-84.
12.Tevaarwerk AJ, Lee JW, Sesto ME, Buhr KA, Cleeland CS, Manola J, et. Al. Employment outcomes among survivors of common cancers: the symptom outcomes and practice patterns (SOAPP) study. J Cancer Surviv. 2013; 7: 191-202.
13.Marx RG, Bombardier C, Hogg-Johnson S, Wright JG. Clinimetric and psychometric strategies for development of a health measurement scale. J Clin Epidemiol. 1999; 52(2): 105-11.
14.Selby-Harrington ML, Mehta SM, Jutsum V, Riportella-Muller R, Quade D. Reporting of instrument validity and reliability in selected clinical nursing journals. J Prof Nurs. 1994; 10(1): 47-56.
15.Olivo AS, Macedo LG, Gadotti IC, Fuentes J, Stanton T, Magee DJ. Scales to assess quality of randomized controlled trials: a systematic review. Phys Ther. 2008; 88(2): 156-75.
16.Gallasch CH, Alexandre NMC, Amick III BC. Cross-cultural adaptation, reliability and validity of the Work Role Functioning Questionnaire to Brazilian Portuguese. J Occup Rehabil. 2007; 17: 701-11.
17.Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et al. The COSMIN checklist for assessing the methodological quality of studies on measurement properties of health status measurement instruments: an international Delphi study. Qual Life Res. 2010; 19: 539-49.
18.Mokkink LB, Terwee CB, Patrick DL, Alonso J, Stratford PW, Knol DL, et. al. COSMIN checklist manual. 2012. Amsterdan (BT): EMGO Institute for Health and Care Research: 2012.
19.Polit DF, Hungler BP. Fundamentos de pesquisa em enfermagem. 3ª ed. Porto Alegre (RS): Artes Médicas: 1995.
20.Dempsey PA, Dempsey AD. Using nursing research: process, critical evaluation and utilization. Philadelphia (PA): Lippincott Williams & Wilkins: 2000.
21.Durand MJ, Vachon B, Hong QN, Imbeau D, Amick III BC, Loisel P. The cross-cultural adaptation of the Work Role Functioning Questionnaire in Canadian French. Int J Rehab. 2004; 27(4): 261-68.
22.Hébert F. Les indicateurs de lésions en santé et sécurité au travaiul: analyses par secteur d'activité économique em 1991. Montreaul (QC): Institut de recherche Robert-Sauvé en santé et sécurité au travail: 1996.
23.Amick III BC, Habeck RV, Ossmann J, Fossel AH, Keller R, Katz JN. PredWAIors of successful work role functioning alter carpal Tunnel release surgery. J Occup Environ Med. 2004; 46: 490-500.
24.Simões JC, Gama RR, Winheski MR. Cancer staging and treatment. São Paulo: Lemar, 2008.
25.Karnofsky DA, Abelmann WH, Craver LF, Burchenal JH. The use of nitrogen mustard in the palliative treatment of cancer with particular reference to bronchogenic carcinoma. Cancer. 1948;1:634-56.
26.Fleck MPA, Louzada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. Portuguese version of the application of the abbreviated instrument for assessing quality of life 'WHOQOL-bref'. Public Health Magazine. 2000; 34(2): 178-83.
27.Zwart BCH, Frings-Dresen MHW, Duivenbooden JC. Teste-retest reliability of the Work Ability Index. Occup Med. 2002; 52: 177-81.
28.Mendes AMB. Psychodynamic aspects of man-labor relationship: the contributions of B. Dejours. Psychology science and profession. 1995; 15: 34-38.
29.Rick O, Kalusche EM, Dauelsberg T, König V, Korsukéwitz C, Seifart U. Reintegrating cancer patients into the workplace. Dtsch Arztebl Int. 2012; 109(42): 102-8.
30.Tamminga SJ, de Boer AGEM, Bos MMEM, Fons G, Kitzen JJEM, Plaisier PW, et. al. A Hospital-based work support intervention to enhance the return to work of cancer patients: a process evaluation. J Occup Rehabil. 2012; 22: 565-78.
31.Roelen CAM, Koopmans PC, Schellart AJM, van der Beek AJ. Resuming work after cancer: a prospective study of occupational register data. J Occup Rehabil. 2011; 21:431-40.
32.Nunnaly JC. Psychometric theory. New York: McGraw-Hill: 1978.
33.Martins GA. Reliability and validity. Journal of Business Management. 2006; 8(20): 1-12.
34.Pagano M, Gauvreau K. Biostatistics Principles. São Paulo: Editora Thomson; 2004.
35.Groeneveld I, de Boer AGEM, Frings-Dresen MHW. A multidisciplinary intervention to facilitate return to work in cancer patients: intervention protocol and design of a feasibility study. BMJ Open. 2012; 2: 1-7.
36.Abma FI, van der Klink, Bültmann U. The Work Role Functioning Questionnaire 2.0 (Dutch version): examination of its reliability, validity and responsiveness in the general working population. J Occup Rehabil. 2013; 23(1):135-47.
37.Vaz AF, Conde DM, Costa-Paiva L, Morais SS, Esteves SB, Pinto-Neto AM. Quality of life and adverse events after radiantion therapy in gynecologic cancer survivors: a cohort study. Arch Gynecol Obstet. 2011; 284: 1523-31.
38.Regis MF, Simões MFS. Breast cancer diagnosis, feelings, behaviors and expectations of women. Rev Eletron Enferm. 2005; 7(1): 81-6.
39. de Boer AGEM, Taskila TK, Tamminga SJ, Frings-Dresen MHW, Feuerstein M, Verbeek JH. Interventions to enhance return-to-work for cancer patients. Cochrane Database of Systematic Reviews 2011, Issue 2. Art. No.: CD007569. DOI: 10.1002/14651858.CD007569.pub2.