RESEARCH ARTICLES
Coronary artery disease and family support in older adults
Lauana Aparecida Teodoro JacintoI; Álvaro da Silva SantosII; Marina Aleixo DinizIII; Larissa Carvalho SilvaIV; Fabíola Silva de Sousa PedrosaV; Juliana Barbosa ArduiniVI
INurse. Specialist in Public and Family Health. Master in Health Care. Nurse at Ministry of Social Defense of Minas Gerais. Uberaba-Minas Gerais, Brazil. E-mail: lauana_jacinto@yahoo.com.br.
IINurse. Doctor in Social Sciences. Associate Professor in the Department of Nursing in Education and Community Health and the Graduate Program in Health Care (Masters and PhD) of the Federal University of Triangulo Mineiro, Uberaba-Minas Gerais, Brazil. Leader of the Research Group Life Cycles, Family and Health in Social Context (CIFACS). E-mail: alvaroenf@hotmail.com.
IIINurse. Master in Health Care. PhD student of the Graduate in Fundamental Nursing Program at Ribeirão Preto College of Nursing, Ribeirão Preto-São Paulo, Brazil. E-mail: mafmtm@yahoo.com.br.
IVNurse. Specialist in Emergency Department. E-mail: lissacarvalhos@hotmail.com.
VNurse at Municipal Health Department of Conceição das Alagoas-Minas Gerais. E-mail: fafasousa2003@hotmail.com.
VINurse. Specialist in Public and Family Health. Nurse at the Hospital of the Federal University of Minas Triangle, Uberaba-Minas Gerais, Brazil. E-mail: julianabarduini@yahoo.com.br.
VIIStudy funded by the Foundation for Research of Minas Gerais.
DOI: http://dx.doi.org/10.12957/reuerj.2014.15664
ABSTRACT: This quantitative study, based on questionnaires applied at interview, was conducted in 2010 to analyze risk factors for coronary artery disease and the relationship of family support in 853 older adults registered with the family health program in Uberaba, Minas Gerais, Brazil. The group was prevalently aged 60 to 79 years (88.6%); women (63.7%) and retirees (81.1%); with income up to 2 minimum wages (78.1%); arterial hypertension (65%); sedentary lifestyle (59%); diabetes mellitus (28%); smoking (21%); alcohol (12.1%); dyslipidemia (4.8%); family relations excellent (49.7%) and good (42%); family monitors state of health (81.7); but does not cooperate with physical exercise (86%), medication (66.7%), financial resources (61.4%) and food (60.5%). It was concluded that health professionals should encourage family support, and together with the State, act to formulate policies and strategies to reduce risk factors for cardiovascular diseases.
Keywords: Cardiovascular diseases; risk factors; older adults; family relations.
INTRODUCTION
The aging issue can be understood as a condition of great social impact, as the diseases and non-communicable diseases (NCD) burden the social system and disqualify the life of its bearer because of the cost of the medication, complications and difficulties in care. However, it is a socio-demographic gain by expanding life expectancy.
The Brazilian population is aging dramatically. According to data from the Brazilian Institute of Geography and Statistics (IBGE)1 the current life expectancy is 74.6 years old. The World Health Organization (WHO) classifies the individual as old those who are 65 years old or older, in developed countries, and 60 or more in developing countries2,3.
The aging must be understood as non-pathological process, with progressive reduction in functional reserve. However, under overload conditions, such as in the presence of cardiovascular disease and emotional stress, one may develop some pathologies that require assistance, featuring senility3,4. This condition of physical or intellectual weakness can be avoided the lower exposure to risk factors for cardiovascular disease4. Because of this, care for the elderly should be based on aging own changes, seeking healthy aging and quality of life5,6.
Cardiovascular diseases (CVD) are a major impact in terms of mortality and morbidity for Brazilian society, being responsible for 28% of deaths from 1996 to 2011. The CVD lead the morbidity and mortality rates in Brazil and in the world, with Coronary Artery Disease (CAD) the cause of a large number of deaths and spending on health care7,8.
Family support can be defined as primary feature of socialization in which patterns of behavior, language, values, beliefs and customs are transmitted and the basic psychological and physiological needs are met. It is a reciprocal process between family members, which generates effects both to the recipient, as those offering it9. Elderly may need independent family support in face of diseases, in various ways. In the case of elderly patients with CAD, they may need both physiological, and emotional family support.
Thus, the objective of this study is: to analyze risk factors for coronary artery disease and the family support relationship in elderly enrolled in the Health Family Strategy of Uberaba/MG.
LITERATURE REVIEW
Population aging is among the main concerns in a country that is seen worldwide as a synonym for youth. But this has been changing in recent decades: Brazil has gone through a development process that is leading to achieve social and demographic indices of a developed country, but with systems and institutions inherited from another context10.
In Brazil, according to the Summary of Social Indicators of 2011, conducted by IBGE, circulatory system diseases amounted to 37.5% of all deaths and are the leading cause of death among the elderly in the country11. Smoking, obesity, diabetes mellitus (DM), hypertension, high cholesterol, family history of CAD and physical inactivity increase the risk of disease12,13. In turn, non-modifiable factors are those which cannot be influenced and cannot be excluded, comprising: ethnicity, gender, age and family history5.
Lifestyle and emotional stress are risk factors for cardiovascular disease and have been highlighted in the literature. Studies have shown a higher incidence of cardiovascular events in people with depressive symptoms or low scores of quality of life indicators. Patients with CAD already installed have impaired quality of life and high level of stress imposed by the disease condition itself, physical limitations and risk of death, closing a vicious circle that intensifies disease progression14.
Considering the most common risk factors to CAD and CVD, on the preventive perspective or even those who are already have these diseases, family participation, in support to the elderly, is important. Often such older people tend to consume more drugs and special diets, rather than receiving physical activity prescription and also stress control, conditions which generally require support from family.
The change in women's status (primary caregivers) and social and family values will continue to affect the availability of family support for the elderly11. The priority in health care of the elderly must turn to strategies that enable healthier life, monitoring indicators able to assess the morbidity, the impact of disease and/or disability in the quality of life for seniors and their families15.
The pursuit of healthy aging is a current challenge, and is of utmost importance in order to offer the elderly greater autonomy, quality of life, beyond the care of preexisting conditions. In these actions, professionals should be aware not only to the physical and physiological changes resulting from the aging process, but also to changes in socio-familiar dynamics, which are crucial in functional capacity and hence in healthy aging16. Thus, health professionals should investigate the factors that have negatively impacted the quality of life of older people, looking for possible solutions together with their families17.
Dimensioning unhealthy lifestyles (fat intake, obesity, uncontrolled stress, sedentary lifestyle, among others) and predisposing to CAD, and the relations of family support, is justified in itself, in that it can provide data for interventions in the elderly at risk or affected by this diseases.
METHODOLOGY
This is a quantitative and descriptive study, which is a description of certain quantitative trait of populations as a whole18.
This type of research meets the intentions of this study since it will present features for risks of coronary artery disease and the family support relationships in the elderly population of Uberaba, in addition to provide data for further investigation and may give support to public policies targeted tot the elderly population, with a view to reducing cardiovascular risks.
The city of Uberaba/MG had a population, in 2009, of 296,261 inhabitants, of which 10.2% were people aged 60 or more. The research was conducted with users of age greater than or equal of 60, registered in health family units (HFU), and who were in attendance during the study period.
Data collection took place from June to August 2010. Respondents were selected in the units or in their homes, every five elderly in the listing of community health workers (CHWs), after guidance on research conditions, with the signing of free and informed consent term. The sample, thus, was chosen by convenience. Data collection was carried out by researchers or trained CHWs, in homes or private room at HFU.
Inclusion criteria were: being 60 years old or older, registered in the HFU and being drawn without replacement every five elderly in the listing of community health workers. Exclusion criteria were provided: elderly who refused to participate in the study, not be drawn, a score equal to or less than 12 on the Mini Mental State Examination (MMSE), or refusing or not being in their homes at the time of interview. The sample consisted of 853 elderly. The MMSE is a validated instrument that assesses cognitive status and considers cognitive decline when the elderly get score equal to or less than 12 points19.
It was applied, after obtaining score equal or higher than 13 on the MMSE, a questionnaire constructed by the researchers, with 39 closed questions, to the elderly who met the inclusion criteria. For this article, the following variables were presented: socio-demographic - age, gender, retirement, family income, race and marital status; risk factors for CAD - smoking, alcohol, physical activity, health hazards; family support - number of residents in the household, numbers of children, number of children living in the same household, family support in the food, medication, physical activity, financial resources, family living and family support on health.
The project was submitted to the Ethics Committee of the Federal University of Triangulo Mineiro and approved under the number 1527.
Data were analyzed by Statistical Package for Social Sciences (SPSS) 16 and numeric data were presented in absolute and percentage values. Categories were analyzed through simple frequency distribution. Results were shown in tables to better understanding.
RESULTS AND DISCUSSION
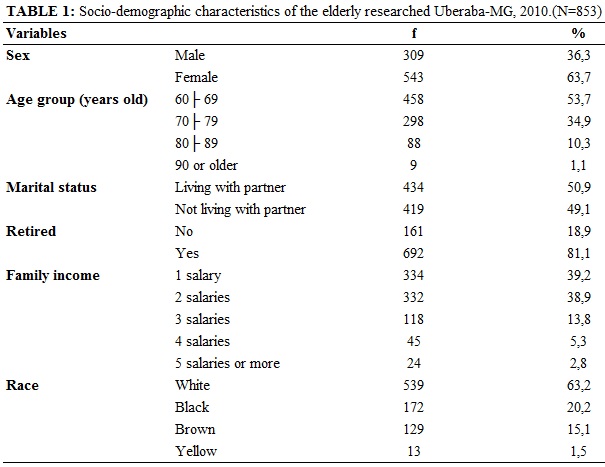
The study included 853 elderly enrolled in family health teams belonging to the three health districts in the city of Uberaba, Minas Gerais. Among the participants, 543 (63.7%) were female and 310 (36.3%) males, of which 539 (63.2%) were white, 172 (20.2%) black, 129 (15.1%) mixed and 13 (1.5%) yellow. The most prevalent age range was between 60 and 69, 458 (53.7%), followed by 70 to 79 years old, 298 (34.9%). Regarding marital status, 434 (50.9%) reported living with a partner and 419 (49.1%) did not live with a partner. About having a paid occupation, only 128 (15%) reported working and 725 (85%) were not working. Most - 692 (81.1%) - reported being retired, and 334 (39.2%) lived with a family income of a minimum wage and 332 (38.9%) with two salaries; only 24 (2.8 %) with five or more salaries, according to Table 1.
Low family income, living without a partner and being female seem to be conditions predisposing to greater dependence on family support. Some studies on seniors’ profile have shown similar data to herein20,21. A study in Pelotas, with 991 elderly, showed more women without partners and with significant association to physical inactivity and functional disability20. Study in Guarapuava with 359 elderly pointed low-income, predominantly women and living with partner21.
Low income limits access to goods and services, as adequate food and housing. As to occupation, research shows that retirement pensions are the main source of income of the Brazilian elderly22.
Regarding the lifestyle that can interfere with the health of the elderly and to promote CAD, it was observed that most - 674 (79%) - reported not smoking and 179 (21%) smoke, of which 82 (46%) smoke 1 to 9 cigarettes per day, and 33 (18.8%) 20 or more. The alcohol consumption was reported by 103 (12.1%) and of these, 29 (28.15%) consume five glasses per week, and 11 (10.7%) five glasses per day or more. Most - 503 (59%) – does not perform any physical activity (PA) and of the 350 (41%) who exercise, the most practiced activity is walking, with 305 (87.1%). Of the major injuries, hypertension appears in 441 (65%), Diabetes Mellitus (DM) in 190 (28%) and dyslipidemias in 32 (4.8%), according to Table 2.
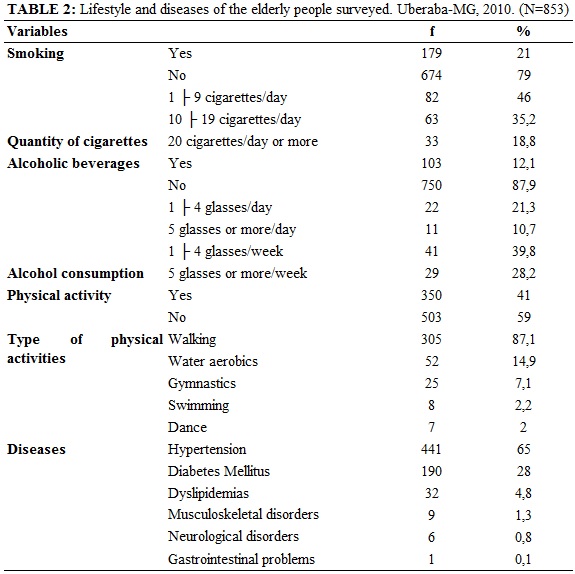
The lifestyle can interfere with the health of older people and lead to a possible CAD. Hypertension, sedentarism, diabetes mellitus, smoking and alcoholism, followed by dyslipidemia were found as important risk factors in the study group. Studies on elderly profile showed as risk factors: hypertension, diabetes mellitus and alcoholism5,23,24.
Hypertension is an important condition for CAD. Study on the prevalence and risk factors in the association between CAD and aortic aneurysm states that, comparing patients with and without CAD, the most frequent risk situations were in the group of patients with coronary disease, however only hypertension and dyslipidemia were statistically significant25.
Another relevant factor is the non-fulfillment of PA by elderly respondents. Studies show that there is a decrease in the activity level related to increasing age, contrary to the theory of activity that argues for the need of the elderly to maintain activity levels despite the losses associated with aging26. A study of elderly with Acute Coronary Syndrome (ACS) showed a sedentary lifestyle as a major risk factor27.
Diabetes mellitus appears as a third factor in this study. Similarly to ACS, study observed DM as an important risk factor27, as well as in another study on risk factors for CAD5. DM is growing rapidly with the aging population and the poor metabolic control is a risk factor for the development of micro vascular and macro vascular complications, which substantially increase the morbidity and mortality associated with these diseases28. Study on CAD and DM showed that in patients with type 1 DM have in CAD the leading cause of death, in which the risk of mortality increases 4 to 9 times in men and 4 to 29 times in women29.
When considering that 179 (21%) of respondents refer smoking, it is remarkable that they are at higher risk of developing diseases related to smoking, as they tend to longer and more intense exposures to tobacco, compared to younger populations24. Tobacco, besides causing cardiac abnormalities, can lead to other pathological conditions; it is a modifiable habit that deserves intervention in the elderly.
Alcoholism appears as the fifth important factor. It is known that alcohol can lead to a number of pathological conditions. A study showed that more than 10% were alcoholics, and this dependence was more present in men30. This is an important condition both as a predisposing factor for CAD, as its worsening; besides, it makes the elderly care more complex.
Regarding the number of people living in household, 305 (35.8%) live with two people, 134 (15.7%) live alone and 118 (13.8%) with five or more people. Regarding family structure was observed that most - 812 (95.2%) - have children, with a prevalence of 292 (34.2%) with five or more. Of those who reported having children, 379 (46.6%) live with one or more children.
When questioning about who would take care of the elderly in case of any disease, 437 (51.3%) reported being the children, 296 (34.7%) recorded the spouse and 27 (3.2%) responded that no one would take care of them.
With respect to family support and more specifically to family life for the elderly, it was observed that 424 (49.7%) reported to be great, 358 (42%) good, 53 (6.2%) regular and 18 (2.1%) bad. Most - 697 (81.7%) - stated that the family came with their health. Regarding the cooperation of the family, most do not receive it, as follows: 734 (86%) exercise, 569 (66.7) medication, 524 (61.4%) and 516 family resources (60.5%) in food, as Table 3.
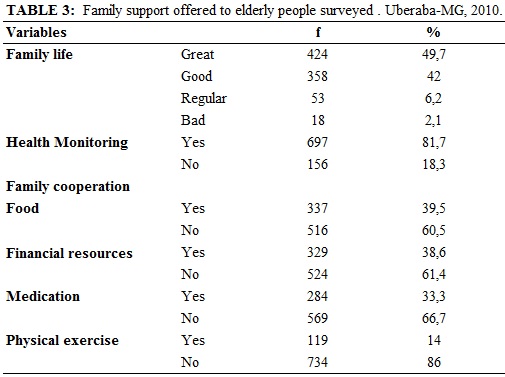
Regarding the type of support, the majority states that the family has great and good relationships, in addition to monitoring their health status, but on the other hand they do not cooperate for physical exercise, medication, financial resources and food.
It was found that there is a significant number of elderly people who live alone and some of them reported that in adverse situation nobody takes care of them, although most of them have children and slightly more than half live with partner, or even the with a child.
Research on the health needs of the elderly shows that household care is provided by family members, especially daughters. The study cites the National Policy for the Elderly, which points out that the family should be responsible for the care of the elderly in relation to meeting their needs. If the spouse cannot take care, the role is assumed by the children. Thus, the health professional that assists the elderly needs to have a broader view of the aging process and the importance of family support network for the elderly31.
Another study indicates that family caregivers are all women, without training to take care of the elderly, who reported not having received formal education of health professionals for such care, carrying them from their previous experiences32. This further reinforces the importance of health professionals in elderly care and support to the family.
Study of the elderly in a UBS, in Fortaleza-CE, showed that the percentage of those living alone is significant, 11.7%. Furthermore, 44.9% lived in multigenerational household, prevailing households with three generations (presence of children and grandchildren). Seniors living in multigenerational households tend to be poorer, more dependent and may not represent a cultural option, but an arrangement to ensure the survival of family members33.
The family cooperation in the categories physical exercise (PE) and medication shown to be low and reveal the need for attention to elderly people surveyed, whereas PE is necessary to preserve the autonomy and functionality, among others; and, on medication, considering it to be of polypharmacy consumer group, errors in the use or in prescription understanding can influence the quality of life of the elderly. A review found, in several studies, that physical exercise has been shown to be effective in the prevention and control of hypertension and heart disease34. Regarding the use of medications, a survey showed that the elderly perceive incomplete medical advice and the need for family support, in addition to cooperation in the use of polypharmacy and its consequences35. The support of family resources, including food quality and quantity are also aspects that must have monitoring and support from family and health professionals.
CONCLUSION
The demographic profile of the population studied is characterized by predominantly female, white, 60 to 69 years old, living with a partner, being retired and family income of 1 to 2 minimum wages.
The main risk factors listed for CAD were: high blood pressure, physical inactivity, diabetes mellitus, smoking, alcohol consumption and dyslipidemia.
Regarding family support for the elderly, it was shown that the family life is great, followed by good, and most have monitored their health status. In turn, cooperation on the food, financial resources and medication is low (most do not receive cooperation). On the issue of physical exercise, the situation is even worse, since in addition to sedentarism, most seniors receive no family support.
The study points out the need for action on health promotion and disease prevention for the elderly, which can reduce their care dependency, help in economics, material and others. The family must provide support to their elderly, who sometimes need to have the attention of health professionals, especially nurses.
The services and health professionals need to develop strategies that show the family responsibility for their elderly. And the State has the important role of creating public policies to support the elderly, when the family is unable to do so.
REFERENCES
1.Instituto Brasileiro de Geografia e Estatística -IBGE. Projeção da população do Brasil, 2013. [on-line] [citado em 05 out 2014]. Disponível em: http://www.ibge.gov.br/apps/populacao/projecao/index.html
2.World Health Organization. Active ageing: a police framework. A contribution of the World Health Organization to the second United Nations World Assembly on Aging. Madrid (Sp): WHO; 2002.
3.Mendes MRSSB, Gusmão JL, Faro ACM, Leite RCBO. A situação social do idoso no Brasil: uma breve consideração. Acta Paul Enferm. 2005;18:422-6.
4.Ministério da Saúde (Br). Secretaria da Atenção à Saúde. Departamento de Atenção Básica. Cadernos de Atenção Básica. Envelhecimento e saúde da pessoa idosa. Brasília (DF): Editora MS; 2007.
5.Silva SS, Caritá EC, Morais ERED. Fatores de risco para doença arterial coronariana em idosos: análise por enfermeiros utilizando ferramenta computacional. Esc Anna Nery. 2010; 14:797-802.
6.Oliveira AMS, Menezes TMO. A enfermeira no cuidado ao idoso na estratégia saúde da família:
sentidos do vivido. Rev enferm UERJ. 2014; 22:513-8.
7.DATASUS. Sistema de Informações Hospitalares -SIH: Ministério da Saúde. 2013. [citado em 18 out 2013]. Disponível em: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sih/cnv/qiuf.def.
8.Silveira RE, Santos AS, Sousa MC, Monteiro TSA. Gastos relacionados a hospitalizações de idosos no Brasil: perspectivas de uma década. Einsten. 2013; 11:514-20.
9.Inouye K, Barham EJ, Pedrazzani ES, Pavarini SCI. Percepções de suporte familiar e qualidade de vida entre idosos segundo a vulnerabilidade social. Psicologia: Refl Crít. 2010; 23:582-92.
10.Veras RP. Experiências e tendências internacionais de modelos de cuidado para com o idoso. Ciênc saúde coletiva. 2012; 17:231-8.
11.Instituto Brasileiro de Geografia e Estatística. Síntese de Indicadores Sociais, 2011. [on-line]. [citado em 16 dez 2011]. Disponível em: http://www.ibge.gov.br.
12.Pinho RA, Araújo MC, Ghisi GLM, Benetti M. Doença arterial coronariana, exercício físico e estresse oxidativo. Arquivo Brasileiro de Cardiologia. 2010; 94:549-55.
13.Jacinto LAT, Santos AS, Dias FA, Silveira RE, Silvano CM. Fatores de risco para doença arterial coronariana em idosos: perspectivas para a atuação da enfermagem. Nursing (São Paulo) 2012; 15:326-30.
14.Moriel G, Roscani MG, Matsubara LS, Cerqueira ATAR, Matsubara BB. Qualidade de vida em pacientes com doença ateroclerótica coronariana grave e estável. Arquivo Brasileiro de Cardiologia. 2010; 95: 691-7.
15.Moraes EN. Atenção à saúde do idoso: aspectos conceituais. Brasília (DF): Organização Pan-Americana da Saúde; 2012. 98 p. [citado 05 de Nov de 2014]. Disponível em: http://apsredes.org/site2012/wp-content/uploads/2012/05/Saude-do-Idoso-WEB1.pdf
16.Ferreira OGL, Maciel SC, Costa SMG, Silva AO, Moreira MAS. Envelhecimento ativo e sua relação com a independência funcional. Texto contexto – enferm. 2012; 21:513-8.
17.Tavares DMS, Ferreira PCS, Dias FA, Oliveira PB. Caracterização e distribuição espacial de homens octogenários. Rev enferm UERJ. 2014; 22:558-64.
18.Lakatos EM, Marconi MA. Fundamentos da metodologia científica. 7ª ed. São Paulo: Editora Atlas; 2010.
19.Icaza MC, Albala C. Projeto SABE. Minimental State Examination (MMSE) del estudio de dementia en Chile: análisis estatístico. Brasília (DF): OPAS; 1999.
20.Ducca GFD, Silva SG, Thumé E, Santos IS, Hallal PC. Indicadores da institucionalização de idosos: estudos de casos e controles. Rev Saude Publica. 2012; 46:147-53.
21.Pilger C, Menon MH, Mathias TAF. Características sociodemográficas e de saúde de idosos: contribuições para os serviços de saúde. Rev Latino-Am Enfermagem. [Scielo-Scientific Electronic Library Online]. 2011; [citado em 18 mar 2014]. 19(5):09 telas. Disponível em: http://www.scielo.br/pdf/rlae/v19n5/pt_22.pdf
22.Victor JF, Ximenes LB, Almeida PC, Vasconcelos FF. Perfil sociodemográfico e clínico de idosos atendidos em Unidade Básica de Saúde da Família. Acta Paul Enferm. 2009; 22:49-54.
23.Andrade W, Araújo A, Campos K. Estudo descritivo sobre a fragilidade de idosos assistidos em uma unidade de saúde da família. Revista de Enfermagem do Centro-Oeste Mineiro 2012; [citado em 12 out 2014] Disponível em: http://seer.ufsj.edu.br/index.php/recom/article/view/111/237
24.Ferreira CC, Peixoto MRG, Barbosa MA, Silveira EA. Prevalência de fatores de risco cardiovascular em idosos usuários do Sistema Único de Saúde de Goiânia. Arquivo Brasileiro de Cardiologia. 2010; 95:621-8.
25.Ferro CRC, Oliveira DC, Guerra FFG, Lucena AJ, Nunes FP, Ortiz ST et al. A prevalência e fatores de risco na Associação entre doença arterial coronariana e aneurisma de aorta. Arquivo Brasileiro de Cardiologia. 2007; 88:40-4.
26.Ribeiro PCC, Neri AL, Cupertino APFB, Yassuda MS. Variabilidade no envelhecimento ativo segundo gênero, idade e saúde. Psicol estud. 2009; 14:501-9.
27.Lemos KF, Davis R, Moraes MA, Azzolin K. Prevalência de fatores de risco para síndrome coronariana aguda em pacientes atendidos em uma emergência. Rev Gaúcha Enferm. 2010; 31:129-35.
28.Nogueira AMT, Temóteo TL, Carvalho CMRG, Carvalho AMO, Borges MESMM, Luz MHBA, Teles JBM. Estudo multidimensional de idosos diabéticos atendidos em ambulatório do Sistema Único de Saúde. Rev enferm UERJ. 2010; 18:25-31.
29.Oliveira DC, Brito Junior FS, Fernandes RW. A. Doença arterial coronariana subclínica em pacientes com Diabetes Mellitus tipo 1 em hemodiálise. Arquivo Brasileiro de Cardiologia; 2009; 93:15-21.
30.Melo Neto JS, Mendes AP, Aragão IG, Alves SA, Corrêa PR, Romano EM. Perfil dos pacientes atendidos no setor de fisioterapia cardiorrespiratória de uma clínica escola de São José do Rio Preto – SP. Arq Ciênc Saúde. 2012; 19:108-13.
31.Lima CA, Tocantins FR. Necessidades de saúde do idoso: perspectivas para a enfermagem. Rev Bras Enferm. 2009; 62:367-73.
32.Martins JJ, Pereira Nascimento ER, Erdmann AL, Candemil MC, Belaver GM. O cuidado no contexto domiciliar: o discurso de idosos/familiares e profissionais. Rev enferm UERJ. 2009; 17:556-62.
33.Victor JF, Ximenes LB, Almeida PC, Vasconcelos FF. Perfil sociodemográfico e clínico de idosos atendidos em unidade básica de saúde da família. Acta Paul Enferm. 2009; 22:49-54.
34.Nogueira IC, Santos ZMSA, Mont’Alverne DGB, Martins ABT, Magalhães CBA. Efeitos do exercício físico no controle da hipertensão arterial em idosos: uma revisão sistemática. Rev Bras de Geriatr Geront. 2012; 15:587-601.
35.Silvano CM, Contim D, Santos AS, Gonçalves JRL. O fenômeno da polifarmácia no idoso frágil. Rev pesq cuid fundam. 2012; 4:2995-3005.