RESEARCH ARTICLES
Nursing consultation to hypertensive patients in family health strategy
Antônia Sylca de Jesus SousaI; Marilia Braga MarquesII; Thereza Maria Magalhães MoreiraIII; Ana Danúsia Izidório Rodrigues de AraújoIV; Ana Zaira da SilvaV; Ana Larissa Gomes MachadoVI
I
Nurse. Master in Nursing. Professor at Universidade Federal do Piauí. Floriano, Piauí, Brasil. e-mail: sylcasousa88@hotmail.com
II
Nurse. Doutoral student at the pos-graduation program on Nursing at Universidade Federal do Ceará. Professor at Universidade Federal do Ceará. Fortaleza,
Ceará, Brasil. e-mail: marilia@ufpi.edu.br
III
Nurse. Doctor in Nursing. Professor at Universidade Estadual do Ceará. Leader of the Research Group on Epidemiology, Cares in Chronicity and Nursing.
Fortaleza, Ceará, Brasil. e-mail: tmmmoreira@yahoo.com
IV
Nurse. Member of the Research Group on Collective Health Care. Picos, Piauí, Brasil. e-mail: anadanusia_15@hotmail.com
V
Nurse. Master student at the pos-graduation program on Clinical care in Nursing and Health. Fortaleza, Ceará, Brasil. e-mail: anazaira18@hotmail.com
VI
Nurse. Doctoral student at the pos-graduation program on Nursing at Universidade Federal do Ceará. Professor at Universidade Federal do Piauí. Picos,
Piauí, Brasil. e-mail: analarissa2001@yahoo.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2015.15597
ABSTRACT
The goal of this study was to describe the actions of nurses from a primary care unit in Picos, Piauí, Brazil, regarding the care of patients suffering from Systemic Arterial Hypertension. This was a descriptive, cross-sectional study, done with 26 nurses who work with family health. The period of the study was from August 2010 to June 2011. Data were collected using a semistructured questionnaire based on a review of the literature, and validated with the use of the Delphi technique. The socioeconomical and professional characteristics of the participants were assessed, as well as the actions performed by the nurses on patients with hypertension. We found that the implementation of the nursing processes is deficient, and the improvement of nursing techniques for acting in primary care is necessary, perfecting the assistance using aspects of the treatment nurses give to patients with hypertension.
Keywords : Nursing; hypertension; family health; consultation.
INTRODUCTION
Systemic arterial hypertension (SAH) is a multifactorial syndrome, in which complex interactions among genetic, environmental and psychosocial factors cause the increase of the blood pressure. As it has been of high national and worldwide incidence, it is now considered as one of the main risk factors for cardiac, cerebrovascular and renal complications 1.2.
From 1990 to 2004, the prevalence of this disease in some locations in Brazil increased from 22.3% to 43.9% 3, reaching more than 30% of the adult population and more than 50% of the elderly in the country 4 . Strategies such as changes in lifestyle and eating habits are essential to avoid the determinants of risk factors for hypertension.Therefore, the early diagnosis of this pathology is of great interest for preventing its complications 5.
It's possible to observe a high index of blood pressure control among users accompanied in primary care compared to other models of care, which shows a the positive impact of the activities carried out by professionals in this health care level 6.
As team members of the Family Health Strategy (FHS), nurses should develop their practice favoring the reorganization of primary care to hypertensive clients, contemplating the development of prevention, promotion and rehabilitation actions for individuals. The care through nursing visits help reach excellence in care, because the needs of the individual are evaluated continuously.The implementation of a structured program also provides the possibility of the individual`s critical evaluation in care, facilitating clinical settings and multidisciplinary communication 7.8.
In the FHS, the nurses stand out as propagators of information and clarification about the importance of healthy habits to control blood pressure and contribute to the implementation of interventions in favor of health. They bring multidisciplinary groups and assistance/educational actions together. Moreover they also help implement programs and consultations, deepening their 7 knowledge.
The nursing professional is responsible for the leadership in the implementation and evaluation of nursing processes (NP), in which the definition of interventions is based on a nursing diagnosis (ND) in order to classify the care provided with a standardized language that can provide a systematization of information and nursing assistance.Thus, the planning and the implementation of nursing care are individualized, and aimed at assisting effectively in improvements of the health situation.The intervention can be performed in different care settings, with several methodologies and tools, applied to patients and families of patients with various health problems 8.11.
The nursing consultations predominate over medical consultations in primary care to hypertensive patients 12. However, some of the aspects aren't being addressed in the consultations, which may cause damage in the disease control and and in the prevention of complications 13.It is required that nurses working in the FHS develop specific skills for the satisfactory completion of the nursing consultation to people with hypertension.
Therefore, the objective of this study was to describe the actions taken by nurses in primary care aimed at monitoring the people with hypertension.
LITERATURE REVIEW
Hypertension is a multifactorial clinical condition characterized by high and sustained levels of blood pressure (BP). It is frequently associated to functional and / or structural changes in target organs (heart, brain, kidneys and blood vessels); along with metabolic changes that may increase the risks of fatal and non-fatal cardiovascular events 4.
The risk factors for the development of hypertension are age, sex, race, family history, rich food intake of fats and salt, obesity, sedentary lifestyle, stress, smoking, alcohol consumption and use of oral contraceptives 6 .These factors are the main aggravating factors to heart diseases and cerebrovascular and renal complications 13.
The high percentage of comorbities of hypertension arises with late diagnosis and inadequate treatment, demanding the need for research on nursing practices geared to the care of people with this type of pathology. 12.
When discussing the importance of a multidisciplinary approach to the care of people with hypertension, there is the need for changes in the health care practices, because it is a multifactorial pathology that requires an interdisciplinar assistance for the greater effectiveness of the treatment 14.
Constant monitoring is required, through routine visits so that aspects as life, non-pharmacological treatment, adverse effects, personal and family lifestyle and the control of blood pressure, are constantly checked by the nurse and reinforced at each meeting. Considering incorporating changes in one's lifestyle is essential for the demands of self-care and requires dedication and motivation of the individual 15,17.
The health interventions developed for individuals with hypertension should transcend conventional practices in primary care.When conducting educational activities that facilitate the promotion of health, encouraging them to self-care, it should also be explored, besides the individual consultation, the group approach. The patients with hypertension are not only consumers of the guidelines in groups, but they are agents and co-producers of a learning process and therefore have a double dimension: they are at the same time, work object of the educational agents and subjects of their own education 18.
The nurses, in their professional practice, must meet the demands of these clients, systematizing their actions, requiring the implementation of the NP, so that their work and knowledge will lead to continuous rethinking of their professional practice 19, which will also allow them to develop actions that transcend the biomedical model which is still very rooted in the care practice to people with hypertension 20.
METHODOLOGY
This is a descriptive study 21 conducted with nurses working in the FHS units in the city of Picos-PI, from August 2010 to June 2011.
The population was composed by 30 nurses working in urban and rural cities. Given the difficulty of access to the units in the countryside, the subjects were selected randomly. The participants were 26 nurses of the units in urban areas and 6 nurses working in rural areas.
The study consisted of four phases. At first, there was a literature revision targeting to build the data collection instrument, a questionnaire which included socioeconomic data, profile and experience of the participants as well as the actions developed in the nursing consultations to hypertensive patients in the FHS.
In the second phase, quiz questions related to the actions developed in the nursing consultations were validated by experts using the Delphi technique, which is the judgment of the displayed items, during which a group of judges evaluates the content and assess it using questionnaires 22.
In the third phase of the study, meetings with nurses were carried out to collect socioeconomic and professional data and schedule the follow-up of three nursing consultation with hypertensive persons to be observed by the researcher. To provide better guidance of the notes taken, we used the questionnaire validated by the judges about the actions addressed in the nursing consultation of the individual with hypertension.
In the fourth phase, nurses were invited to participate of an interview where they were asked the same question: which aspects are contemplated in the nursing consultation with hypertensive people? To ensure the anonymity of the participants of this study, they were identified by the order of the consultations, through the use of terms (E1, E2, E3, ..., E26).
For data analysis we used descriptive statistics. The presentation of the findings were displayed in pictures and tables.The research was conducted after each user had acknowledged the methodology and objectives of the study, agreeing and signing the Term of Informed Consent (IC).The development of the study followed the principles expressed in resolution no. 466/12 of the National Health Council (CNS), which establishes the ethical principles of research involving human beings 23, and was part of the project entitled "Nursing Practice in the Prevention and Control of Chronic Non-communicable Diseases", No. CAAE: 0269.0 .045.000.10.
RESULTS AND DISCUSSION
The data relating to socio-economic and professional profile of the research participants nurses are shown in Table 1.
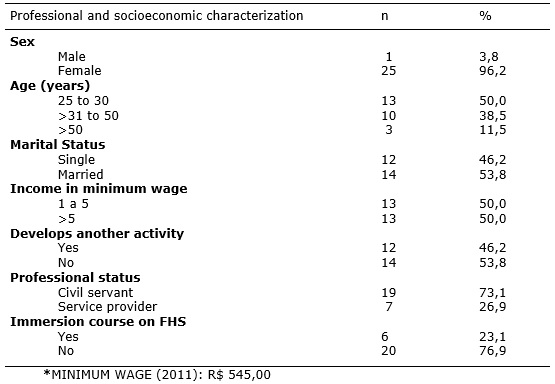
TABLE 1: Professional and socioeconomic characterization of the nurses, Picos, March - April, 2011.
There was a predominance of females among the studied nurses, in which 25 (96.2%) of them had the age range from 20 to 30 years old, 13 (50.0%) were married, 14 (53.8%), appeared to be young professionals working in the FHS city. It was noticed also that 12 (46.2%) of the nurses developed some other work, showing us their work in primary care is not their unique job. It is known that to act as a member of the FHS team, nurses must work about eight hours daily 24, but exclusivity isn't required in this activity.
There was predominance of civil servant professionals, 19 (73.1%), a considerably small figure, and an even smaller number, 7 (26.9%), consisted of professionals performing provided service.The work in the FHS requires the professional to reside in the city where they work, this condition is favored by those who are civil servants24.
Among the interviewed nurses, 20 (76.9%) did not undergo an immersion course prior to being hired to act with population assisted by the USF. It is recommended that training should be started along with the start of the work at the FHS through the introductory course for all staff 24.
During the observation of the nursing consultations with hypertensive clients, we have noted that 14 (53.4%) nurses performed nursing consultation with hypertensive patients systematically, but we have also noted a fairly high number of professionals, 12 (46, 1%), which did not perform the consultation.
The reports of the nurses regarding the steps of the nursing process contemplated in the appointment with the person with hypertension are summarized in Picture 1.
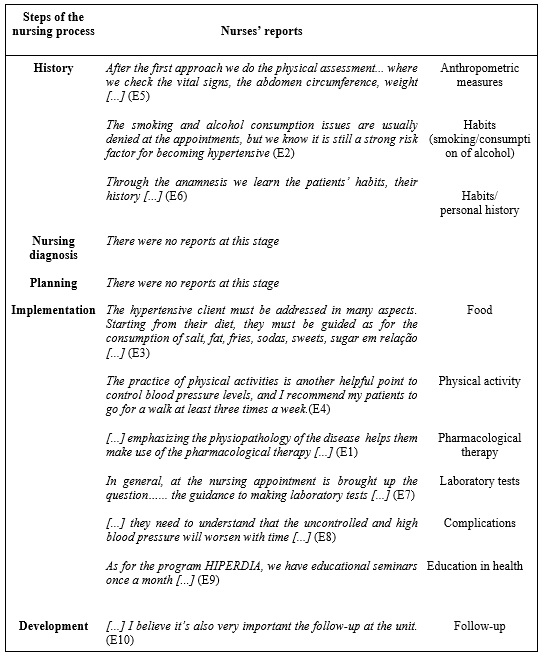
PICTURE 1:
Nurses' reports about the appointments with hypertensive patients, according to the steps of the nursing process Picos, March- April, 2011
The aspects that nurses reported while their performance in nursing consultation were: the first step of the process, which is the nursing history, collecting data and providing information about the anthropometric measurements, habits (smoking / drinking) and personal history. They also performed the implementation through guidance on diet, physical activity, pharmacological therapies, laboratory tests, complications on the pathology and health education activities; Finally, the developments, accompanying the patient on a routine basis at the Health Unit.
The actions reported by the nurses lead to the reflection on how the conduct of nursing consultation should not be restricted to these steps, in which only the disease is being focused, instead of assisting the individual holistically.
In an analytical analysis of the nursing process in Brazil 25, it is possible to see that the nursing process (PE) loses its essence when it's addressed in a fragmented way, which occurred in most studies, 74 (66%). They did not address the integrated steps of this process, but only a few separate, independent and fragmented steps. Among these NP fragments, most, 16 (14.3%), referred to the nursing diagnosis, showing the concern of professionals to work with human responses to processes and pathological conditions, an even more reductionist view of the human being.
From the observation of nursing consultations during the data collection, it was noticed which aspects were evaluated by nurses, shown in Table 2.
TABLE 2: The work of nurses at appointment with hypertensive patients at FHS. Picos-PI, March- April, 2011.
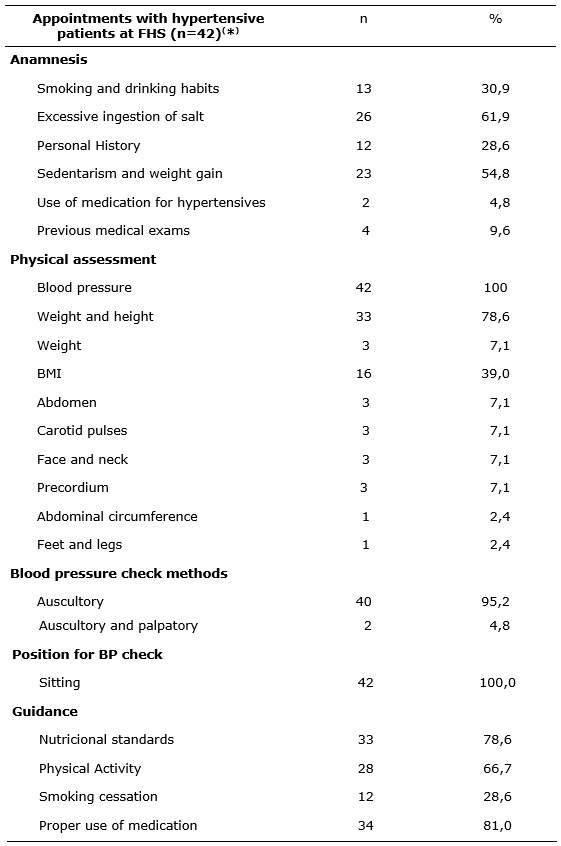
*It were observed two appointements with hypertensive patients for each nurse.
It is observed that, in the anamnesis, the investigation of excessive consumption of salt along with a sedentary lifestyle / weight gain were prioritized, characterized by 26 (61.9%) and 23 (54.8%) occurrences, and the other fundamental items at this stage of the consultation were underemphasized.
The Brazilian population has a food standard rich in salt, sugar and fats, and some factors - such as being overweight - have been correlated with the rise in the blood pressure since young ages. This scenario requires further investigation of the professional during the consultation in order to contribute to early detection and treatment of this disease 4.
As for the aspects covered during the physical examination, nurses, if at all, made the check the of blood pressure with the patient seated, but 40 (95.2%) professionals only used the auscultatory method, which differs from the prioritized in the literature 4, where one should make use of the auscultatory and palpatory methods both. In another research on physical examination 15, the fact that techniques such as palpation and auscultation are being neglected by the nurses, brought attention to this matter.
Among the standards of the consultation with hypertensive clients, the activity most frequently performed by nurses in this study were the guidelines on the proper use of medication, 34 (81.0%), maintenance of nutritional standards, 33 (78.6%) , regular physical activities, 28 (66.7%) and the encouragement for smoking cessation, 12 (28.6%).
In another study related to nursing consultation with people with hypertension 14, 22 records related to the action guide were found, representing only 2.1% of all intervention records of the research. The interventions related to the awareness of patients with hypertension are still incipient in terms of bringing them to adopt favorable favorable to the control of risk factors, may be explained by the complexity involved with the act of dealing with behavioral and subjective questions related to the treatments.
CONCLUSION
The present study verified some gaps in the implementation of the nursing process while conducting nursing consultations to hypertensive patients in primary care. These findings evidence the need for the ongoing education of nurses in primary care in order to provide a systematized care to the individual with hypertension.
It also appears that the implementation of nursing consultations to hypertensive patients did not become part of the routine in the primary care services that were investigated. It should be noted, however, that some nurses perform the appointments and bring awareness to clients about their health condition, setting with them goals and plans for how to continue the treatment.
This research presents certain limitation as for the small sample analyzed. Given the difficulty of access to professionals and to some basic units. It is suggested, therefore, that further research for interventions be carried out aiming at changing the practice performed in this scenario through courses and training to nurses while still in service.
REFERENCES
1.Berardinelli LMM, Figueiredo TFL, Oliveira AS, Santos I, Giron MN, Ramos JP. Hipertensão arterial e conhecimento popular: potencializando o cuidado. Rev enferm UERJ, 2013; 21: 446-51.
2.Fava SMCL, Figueiredo AS, Franceli AB, Nogueira MS, Cavalari E. Diagnóstico de enfermagem e proposta de intervenções para clientes com hipertensão arterial. Rev enferm UERJ, 2010; 18: 536-40.
3.Ministério da Saúde (Br). Departamento de Ações Programáticas Estratégicas. Plano de Reorganização da Atenção à Hipertensão Arterial e ao Diabetes mellitus. Brasília; 2001.
4.Sociedade Brasileira de Cardiologia; Sociedade Brasileira de Hipertensão; Sociedade Brasileira de Nefrologia. VI Diretrizes Brasileiras de Hipertensão. Arq Bras Cardiol, 2010; 95: 1-51.
5.Almeida APR, Silva FAA, Santiago JCS, Moreira TMM, Oliveira ASS, Machado ALG. Caracterização sociodemográfica e hábitos de vida de acadêmicos: identificando fatores de risco para hipertensão arterial. Rev enferm UERJ, 2013; 21: 760-5.
6.Gomes TJO, Silva MVR, Santos AA. Controle da pressão arterial em pacientes atendidos pelo programa hiperdia em uma unidade de saúde da família. Rev Bras Hipertens, 2010; 17: 132-9.
7.Curcio R, Lima MHM, Torres HC. Protocolo para consulta de enfermagem: assistência a pacientes com diabetes melittus tipo 2 em insulinoterapia. Rev Gaúcha Enferm., 2009; 30: 552-7.
8.Vieira RQ, Oliveira EC, Lima JV, Rubbo AB. História da assistência de enfermagem brasileira acerca da hipertensão arterial (1949-1988). HIST. ENF. REV. ELETR (HERE), 2014; 5: 67-82.
9.Santos JC, Florêncio RS, Oliveira CJ, Moreira TMM. Adesão do idoso ao tratamento para hipertensão arterial e intervenções de enfermagem. Rev Rene, 2012; 13: 343-53.
10.Scain SF, Franzen E, Santos LB, Heldt E. Acurácia das intervenções de enfermagem para pacientes com diabetes mellitus tipo 2 em consulta ambulatorial. Rev Gaúcha Enferm.; 2013, 34:14-20.
11.Barreto MS, Marcon SS. Participação o familiar no tratamento da hipertensão Arterial na perspectiva do doente. Texto Contexto Enferm, 2014; 23: 38-46.
12.Hoepfner C, Franco SC. Inércia clínica e controle da hipertensão arterial nas unidades de atenção primária à saúde. Arq Bras Cardiol., 2010; 95: 223-9.
13.Barros ALBL, Vieira FS, Assis CC, Zeitoun SS. Alterações do nível pressórico e fatores de risco em graduandos de enfermagem. Acta Paul Enferm., 2009; 22:773-8.
14.Costa FBC, Oliveira CJ, Araújo TL. Intervenções de enfermagem em portadores de hipertensão arterial: análise documental. Rev enferm UERJ, 2008; 16:482-8.
15.Manzini FC, Simonetti JP. Consulta de enfermagem aplicada a clientes portadores de hipertensão arterial: uso da teoria do autocuidado de Orem. Rev Latino-Am Enfermagem, 2009;17:114-20.
16.Alves EBL. Acompanhamento de enfermagem aos idosos hipertensos: relato de experiência. InterScientia; 2014; 2: 3-15.
17.Borges JWP, Pinheiro NMG, Souza ACC. Hipertensão comunicada e hipertensão compreendida: saberes e práticas de enfermagem em um Programa de Saúde da Família de Fortaleza, Ceará. Ciência & Saúde Coletiva, 2012; 17: 179-18.
18.Toledo MM, Rodrigues SC, Chiesa AM. Educação em saúde no enfrentamento da hipertensão arterial: uma nova ótica para um velho problema. Texto contexto – enferm., 2007; 16: 233-8.
19.Felipe GF, Abreu RNDC, Moreira TMM. Aspectos contemplados na consulta de enfermagem ao paciente com hipertensão atendido no programa saúde da família. Rev esc enferm USP., 2008; 42:520-7.
20.Reiners AAO, Nogueira MS. Conscientização do usuário hipertenso para a adesão ao tratamento. Rev Latino-Am Enfermagem., 2009; 17: 59-65.
21.Andrade MM. Pesquisa científica: noções introdutórias. In:______. Introdução à metodologia do trabalho científico. 7ª ed. São Paulo: Atlas; 2006.
22.Duffield C. The delphi technique: a comparison of results obtained using two expert panels. Lut.J.Nurs.Stud, 1993; 30: 277-37.
23. Brasil. Conselho Nacional de Saúde (Br). Resolução n.466/12. Dispõe sobre diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Brasília (DF): Conselho Nacional de Saúde; 2012.
24.Ministério da Saúde (Br). Estratégias para o cuidado da pessoa com doença crônica: hipertensão arterial sistêmica. Brasília: Ministério da Saúde, 2013.
25.Aguiar DT, Meneses GGM, Pinto FJM, Moreira TMM, Fialho AVM. Processo de enfermagem: análise de dissertações e teses de enfermagem no Brasil de 1979-2007. Cogitare Enferm, 2010; 15: 742-8.