(*) Angina, Acute Myocardial Infarction or Heart Attack
(**) Help from friends, relatives or neighbors in case of need
ORIGINAL RESEARCH
Hospitalization-related risk factors in older adults receiving primary health care
Fabiana Maria Rodrigues Lopes de OliveiraI; Kátia Nêyla de Freitas Macedo CostaII; Maria de Lourdes de Farias PontesIII; Patrícia Serpa de Souza BatistaIV; Keylla Talitha Fernandes BarbosaV; Maria das Graças Melo FernandesVI
I
Master in Nursing from the Federal University of Paraíba. Professor,
University Center of João Pessoa. Paraíba, Brazil. E-mail:
fabianarodriguesenf@yahoo.com.br
II
PhD from the Federal University of Ceará. Professor, Federal University of
Paraíba. João Pessoa, Paraíba, Brazil. E-mail: katianeyla@yahoo.com.br
III
PhD from the University of São Paulo. Professor, Federal University of
Paraíba. João Pessoa, Paraíba, Brazil. E-mail: pontesshalom@gmail.com
IV
PhD in Education from the Federal University of Paraíba. Professor, Federal
University of Paraíba. João Pessoa, Paraíba, Brazil. E-mail: patriciaserpa@oi.com.br
V
Master in Nursing from the Federal University of Paraíba. Professor,
University Center of João Pessoa. João Pessoa, Paraíba, Brazil. E-mail: keyllafernandes@gmail.com
VI
PhD in Health Sciences and Sociology. Professor, Federal University of
Paraíba. João Pessoa, Paraíba, Brazil. E-mail:
graacafernandes@hotmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2018.15488
ABSTRACT
Objective: to evaluate risk factors associated with the hospitalization of older adults using a hospital admission risk prediction instrument. Method: in this cross-sectional study of a sample of 368 older adults enrolled in the Family Health Strategy, data were collected from February to April 2014, and treated by descriptive analysis and binary logistic regression modelling. The project was approved by the research ethics committee (CAAE number: 22372413.5.0000.5188). Results: the older adults at high risk of hospitalization predominantly reported fair self-rated health; a hospital admission and more than six medical appointments in the prior year; diabetes; cardiovascular disease; female sex; social support; and age 60-74 years. Conclusion: considering the adverse effects of hospitalization on the health of older adults, and the possibility of preventing them, nursing professionals should know the risk factors for hospitalization in order to reduce the occurrence of such events.
Descriptors: Risk factors; hospitalization; health of the elderly; primary health care.
INTRODUCTION
Population aging is a phenomenon influenced by socio-cultural, economic and political aspects, and is seen as a state of dependency and fragility. At this stage of life, there is a decrease in the functional performance and capacity of some systems, as well as growth in the formation of autoantibodies, which culminates in increased susceptibility to various health problems1-3.
In this context, there is an increase in the incidence of chronic conditions directly related to a change in the morbidity and mortality profile and demand for health services. Thus, in view of the changing pattern of illnesses, Brazil has faced a reality of excessive spending on hospital admissions, treatment and rehabilitation. In addition to the economic costs, hospitalization of elderly patients generates several consequences that directly affect their functionality and quality of life. As a matter of fact, for the majority of the elderly, the event of a hospitalization can be a factor that accelerates the process of fragility and consequent morbidity and mortality rates4-6.
To reduce the growing number of hospitalizations in the elderly population, it is necessary to know the factors that are associated to these events so that health care can be planned with a focus on their specificities. With this goal in mind, a risk prediction instrument for repeated hospital admission was developed in the US through a cohort study, named Probability of Repeated Admission (PRA), covering eight risk factors for hospitalization in the elderly population, namely: male gender, age over 75 years, availability of caregiver, poor self-perception of health, presence of cardiovascular disease, presence of Diabetes mellitus, hospitalization in the last 12 months, and six medical visits in the last 12 months7.
In the Brazilian reality, studies have confirmed that this instrument is effective for detecting the risk of repeated hospitalization in the elderly8-13. In this context, the present research aimed to evaluate the risk factors associated with the hospitalization of elderly people through the Probability of Repeated Admission instrument.
LITERATURE REVIEW
Hospitalization incurs considerable damages to the health of the elderly, including impairment of functional capacity. Functional decline during hospitalization is often associated with increased dependence, reduced quality of life and autonomy, increased risk for falls, institutionalization and premature death14,15.
From 2001 to 2004, when the elderly accounted for 8.4% of the Brazilian population, the hospitalization rate in this segment increased by 13%. In 2009, the elderly were involved in 21% of hospitalizations in Brazil16. It is thus necessary to adopt health actions with a preventive perspective in order to reduce the number of hospitalizations, as proposed by activities developed in the Family Health Strategy (FHS), which has health promotion and prevention of diseases as main ideology8.
The approach of elderly people in the FHS aims to keep them in the community through prevention, treatment and rehabilitation, and active search for risk factors that affect these people. It is important to highlight that prevention of hospitalization of elderly people should be a target in all levels of health care; however, it is in primary care that this task becomes more feasible and efficient because it is the main entry point to the Unified Health System and it is closer to the daily life of the elderly. Thus, hospitalization in advanced ages should only be considered when the resolving capacity at the primary care level becomes inefficient17.
METHODOLOGY
This is a descriptive, cross-sectional study with a quantitative approach carried out at the homes of elderly people enrolled in the FHS of the city of João Pessoa, Paraíba.
The study population comprised 66,808 elderly people. A probabilistic sample was calculated for the study. The following formula was used for calculation: n = Z2 PQ/d2, where n = minimum sample size; Z = reduced variable; P = probability of finding the phenomenon studied; Q = 1-P; d = desired accuracy. A p = 50% was adopted because this is a multidimensional evaluation, and the sample error parameter adopted was of 5%. The final sample consisted of 368 elderly.
Individuals older than 60 years of age of both sexes enrolled in the FHS in the abovementioned city were included. Elderly people who showed hearing deficits and speech problems that made communication difficult were excluded.
Data collection took place from February to April 2014 through structured interviews conducted by students of the Undergraduate Nursing Course of the Federal University of Paraíba. The students were previously trained and had the help of community health agents. An instrument containing two parts was used in the interviews; the first part addressed the sociodemographic and clinical characterization of the elderly, and the second contained the PRA. Family Health Units were randomly and proportionally selected from the Health Sanitary District. In the field, the researcher raffled a micro-area and one of its streets. Then the households were randomly selected, so that after the first house was drawn, the next third house in the sequence would be selected, and so forth..
For quantitative analysis, data were initially typed and organized into a computerized database, using the Statistical Package for Social Science (SPSS), version 20.0.Later, data were treated through descriptive statistics, applying the calculation of simple and mean frequencies. A Binary Logistic Regression Model was also used to evaluate the risks represented by the PRA factors. The Logistic Regression presented specificity of 98.3% and sensitivity of 13.9%.
Throughout the process, the ethical aspects that rule research involving human beings were observed according to Resolution nº 466/2012 of the National Health Council18. The elderly people signed the Informed Consent Form. The project was approved by the Ethics and Research Committee of the Health Sciences Center with protocol no 575/13 and CAAE: 22372413.5.0000.5188.
RESULTS AND DISCUSSION
Profile of the elderly
The study population consisted of 368 elderly people, with a prevalence of women, aged between 60 and 74 years, brown, and married, followed by widow/widower. The predominance of the female sex in the elderly population is seen as a worldwide trend, being this phenomenon named in the gerontological literature as feminization of aging. In Brazil, in 2000, there were 81 men for every 100 women. Projections indicate that by 2020 there will be 78 men for every 100 women. This trend is most evident with the advancing of age because of the increasing divergence of life expectancy between the sexes. In 2000, there were 60 men for every 100 women in the group of 80 years or more4.
Regarding skin color, the results of this article differ from those found in a study on risk of hospitalization in Rio de Janeiro in which 63.2% of the subjects reported white color, followed by 26.3% reporting brown color9. Such divergence may be related to the socioeconomic level of the elderly interviewed. In the present study, the sample consisted of elderly people enrolled in the FHS, while in the former study, the interviewees lived in neighborhoods in the northern part of the city of Rio de Janeiro and were clients of a self-management health care foundation and federal public servant pensioners.
The racial composition of the Brazilian elderly population has undergone some transformations. According to the 2010Demographic Census, in the year 2000, white elderly people were majority, followed by brown and black people, and in 2010, there was a decrease in the proportion of white elderly people and an increase in the number of brown and black skinned people19. Amid the constant economic, demographic, political and social changes of the country, inequalities in the health conditions of racial groups are well-known. Brown and black skinned elderly predominate in the younger age groups, and have a high dependence on the Unified Health System, lower schooling, and low income in regions with the worst health indicators in the country, when compared to white elderly. This disparity is the result of denial of social rights throughout life which reflect on a poor quality of life during senescence20.
Regarding the marital situation, the findings of this research are in line with a study carried out with elderly people assisted in the primary care network21. Marital status is the demographic characteristic that shows the greatest correlation with sex-related differences and the cultural behavior that influences it. In this context, women culturally tend to become widows, and men have a greater ease of remarriage, which, consequently, causes an increase in married and widowed people in this population. According to the National Household Sample Survey 22,23 conducted in 2009, the largest proportion of widowed persons are women, and the number of widows is four-fold greater than that of widower, while the number of married men aged 70 and over surpassed by 40.3% the female population.
Prediction of risks for repeated hospitalization
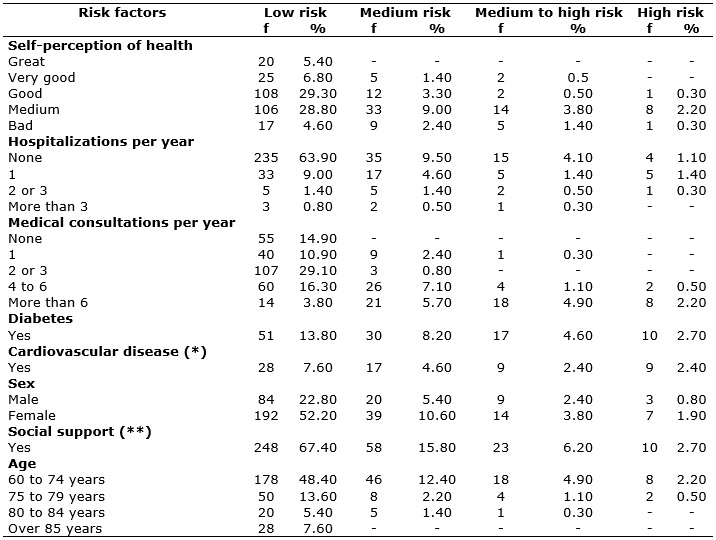
Data on the risk factors addressed in the PRA are presented in Table 1.
TABLE 1:
Distribution of risk factors stratified by levels in the study population.
João Pessoa, Paraíba. (N = 368)
(*)
Angina, Acute Myocardial Infarction or Heart Attack
(**)
Help from friends, relatives or neighbors in case of need
As for the self-perception of health, there was a predominance of the good option among the individuals who were under low risk, while the medium self-perception of health predominated among the higher risk groups. These findings are similar to those of a study carried out with elderly people in a teaching health center13. Self-perception of health is a variable of good reliability that encompasses physical elements, psychological components, well-being and satisfaction with life. Thus, the elderly's understanding of their state of health involves not only physical limitations, but especially the social and psychological relevance of their health situation, and above all, their way of facing the adversities of life24.
A study carried out in 2008 through the National Household Sample Survey shows that about 70% of the Brazilian adult population evaluated their overall health status as good or very good, and that this evaluation is associated with individuals who were never smokers and who were physically active, did not report chronic diseases, and did not went to medical consultations in the last 12 months25. On the other hand, elderly who mentioned a poor health state end up using more medication and attend with a higher frequency to medical consultations, which is associated with a higher number of hospitalizations26.
Regarding the number of hospital admissions in the last year, the response no hospitalization prevailed among the investigated elderly who presented low risk. In turn, among the elderly with high risk, the predominant response was at least one hospitalization in the last year. These data corroborate the findings of a study on repeated admissions involving 764 elderly people in which 87% of the interviewees who had low risk reported not having been hospitalized in the last 12 months, while 83.6% of the elderly with high risk had at least one hospitalization in the previous year9.
A study carried out in an outpatient clinic of the public network, elderly people who reported at least one hospitalization had a 3.5-fold higher risk than the group who did not report hospitalizations in the last twelve months12. It is worth emphasizing that hospitalization is a factor that, besides increasing the worsening of the overall health status of elderly people, also exposes them a greater chance of developing other diseases.
Regarding the number of medical consultations, in the present study, the elderly attended at least two or three medical appointments in the previous year, reaching a prevalence of more than six visits in the group with high risk for hospitalization. This is similar to that found in a study carried out in the primary care which showed that 68.8% of the sample had gone to two or more medical consultations in the last 12 months prior to the interview11. Another study that used the same instrument at the international level showed that the group of elderly at high risk for hospitalization was 2.1-fold more likely to have more than six medical appointments in the following year when compared to the low-risk group 27. It should be noted that the high number of medical consultations is associated with worse health levels, as well as poor self-perception of health.
Regarding the presence of Diabetes mellitus and cardiovascular disease, this study showed results that agree with a study carried out with individuals older than 65 years in the city of Botucatu in which about 18% of the participants presented diabetes and at least 19% reported cardiovascular diseases13. Due to the changes that elderly people experience as they get older, there is an increase in vulnerability, risk of illnesses, and incidence of chronic conditions that may lead to loss of functionality and autonomy.
A study conducted in Belém do Pará on the global functionality of hospitalized elderly showed that 67% of hospitalizations were due to cardiovascular disease and 50% due to endocrine and metabolic diseases28. Another study carried out with 422 hypertensive individuals monitored by a family health unit found that among the interviewees who reported hospitalization in the last 12 months, 45.10% had had cardiovascular problems29. Moreover, according to the World Health Organization30, there are more than 347 million diabetic people in the world and cardiovascular diseases account for 50% to 80% of deaths in people with this health impairment.
Regarding sex, the findings of this study differ from those of a study on repeated admissions in Rio de Janeiro with 764 elderly people, where the majority of people at high risk were male9. This may be associated with the relatively greater number of women investigated in the present study. There is a relationship between male sex and more frequent hospital admissions. This is a gender issue in which men and women under the influence of distinct cultural elements develop self-care patterns that are also divergent. Thus, throughout the life, men, in general, do not have self- care attitudes, due to a socially defined question. The lack of responsibility for the own health identified among males and the absence of health preventive and promotion practices lead to an aging with more morbidities, more adverse health conditions, as well as a high mortality rate and hospitalizations31,32.
In this research, regardless of risk stratification, about 92% of the elderly reported having help from a friend, relative or neighbor in case of need, which is in line with the findings of studies that used PRA in the Brazilian reality8-13. In the United States, in which this instrument was applied, the absence of a caregiver when needed is directly related to a reduction of the risk of hospitalization since it reveals a sign of self-sufficiency of the elderly33.
In the Brazilian reality, the importance of social support to enhance survival has been proved. Although it is not yet clear how social support acts in the immune system, it is believed to act as a buffer, making it impossible for the body to respond to large losses caused by illnesses; another hypothesis is that social support reinforces the feeling of control over one's life, guaranteeing positive results on health 34.
There are differences of meaning when the PRA is applied in a different sociocultural context for which it was created. Thus, a study on repeated hospitalization in Rio de Janeiro suggests that, in the Brazilian reality, the issue of social support should be replaced by the identification of another variable, namely, living alone, which has been widely pointed out in the literature as a factor that increases the vulnerability of the elderly and, consequently, the number of hospitalizations9.
Regarding age, the age group between 60 and 74 years predominated in the low-risk group, which is similar the findings of a study that verified the predictive validity of PRA9. However, in this study, the prevalence of this age group also occurred in the group of elderly individuals who showed a high risk for hospitalization, which differs from is found in the pertinent literature, which affirms a higher risk among elderly individuals aged 75 years or more9,13. This may be related to the greater proportion of young elderly investigated in the present study.
The older the elderly person, the greater is the number of hospitalizations because over the years, there is a greater physiological and functional decline that causes more pathologies and health problems. According to data from the National Household Sample Survey, from the age 60 onwards, hospitalization coefficients began to increase from 9.9% to 18.2% in elderly people aged 80 years and over35. Moreover, the rate of hospital admission in the age group of 80 years and over is three times higher than that of the group aged 55-59 years, indicating that the older the elderly, the greater is the risk for hospitalization36.
CONCLUSION
The socio-demographic profile of the studied population was characterized by the prevalence of females; ages of 60-74 years; brown skinned; married, followed by widows/widowers. In this study, elderly people with a good health self-perception; no hospitalization in the last year; two or three medical consultations in the last 12 months; non-diabetic; presenting no cardiovascular disease; of female sex; with caregivers available for their assistance in case of need, and aged between 60 and 74 years predominated among the elderly who had lower risk for hospitalization. In turn, elderly with medium self-perception of health; at least one hospitalization in the last year; more than six medical consultations in the last year; diabetic; with cardiovascular diseases; of the female sex; with availability of caregiver; and with age range between 60 and 74 years predominated in the group that showed a high risk for hospitalization.
The limitation of this study is the fact that the instrument used has not been validated for the Brazilian reality. Despite the social and political differences in the world context, the variables contained in this instrument are linked to repeated hospitalizations in the elderly of any socioeconomic reality. Another limitation of the present research is the cross-sectional approach that does not allow inferring cause and effect relationships of the evaluated variables. In this context, we recommend longitudinal studies addressing the theme in question.
Considering the abovementioned considerations, it is noticeable that the risk factors contained in the PRA are closely associated with hospitalization in the elderly population. Thus, we emphasize that repeated hospitalizations are avoidable in the aging process as long as emphasis be placed on prevention of injuries and health promotion. Thus, the study recommends that health professionals adopt measures of risk classification, prevention of diseases and health promotion among elderly people in order to know the risk factors associated to hospitalizations and, based on this, health actions based on the specifics of these clients be implemented so as to avoid the occurrence of undesirable events such as worsening of chronic conditions and the hospitalization outcome.
REFERENCES
1.Fechine BRA, Trompieri N. The aging process: the main changes that occur with the elderly over the years. International Scientific Rev. 2012 [cited in Aug 20, 2017]; 1 (20): 106-32. Available from: http://ucbweb2.castelobranco.br/webcaf/arquivos/15482/10910/envelhecimento.pdf
2.Barros MAA, Oliveira DST, Carvalho MAP, Fernandes MGM, Costa KNFM, Santos KFO. Characteristics of the diseases and care provided to the elderly in a mobile pre-hospital service. Rev. enferm. UERJ. 2013; 21 (1): 569-74.
3.Pulchinelli Júnior A, Cury Júnior AJ, Gimenes AC. Clinical laboratory findings in the elderly. J. bras. patol. med. lab. (Online). 2012; 48 (3): 169-74.
4.Chaimowicz F. Elderly Health. 2nd ed. Belo Horizonte (MG): NESCON-UFMG; 2013.
5. Nunes BP, Soares MU, Wachs LS, Volz PM, Saes MO, Duro SMS, et al. Hospitalization in the elderly: association with multi-morbidity, basic care and health plan. Rev. public health (Online). 2017; 51 (43): 1-10.
6. Dantas IC, Pinto Junior EP, Medeiros KKAS, Souza EA. Profile of morbimortality and the challenges for home care of Brazilian elderly. Rev. Kairós geront. 2017; 20 (1): pp. 93-108.
7.Boult C, Dowd B, McCaffrey D, Boult L, Hernandez R, Krulewitch H. Screening elders for risk of hospital admission. J. Am. geriatr. soc. 1993; 41 (1): 811-7.
8.Negri LSA, Ruy GF, CollodettiI JB, Pinto LF, Soranz DR. Application of an instrument for the early detection and predictability of diseases in the elderly population. Ciênc. saúde coletiva (Online). 2004; 9 (4): 1033-46.
9.Perez M, Lourenço RA. FIBRA-RJ Network: fragility and risk of hospitalization in the elderly in the city of Rio de Janeiro, Brazil. Cad. Public Health (Online). 2013; 29 (7): 1381-91.
10.Dutra MM, Moriguchi EH, Lampert MA, Poli-de-Figueired CE. Predictive validity of an instrument to identify elderly people at risk of hospitalization. Rev. public health (Online). 2011; 45 (1): 106-12.
11.Estrella K, Oliveira CEF, Sant'Anna AA, Caldas CP. Detection of risk for hospital admission in the elderly population: a study from the point on entrance into the supplementary health system. Cad Public Health (Online). 2009; 25 (3): 507-12.
12.Veras RP. In search of adequate health care for the elderly: review of the literature and application of an instrument for early detection and predictability of diseases. Cad. Public Health (Online). 2003; 19 (3): 705-15.
13.Guerra IC, Ramos-Cerqueira ATA. Risk of repeated hospitalizations in elderly users of a teaching health center. Cad. Public Health (Online). 2007; 23 (3): 585-92.
14.Sthal HC, Wey BH, Castilho PV. Degree of dependency of hospitalized elderly people on basic activities of daily living. Text & context enferm. 2011; 20 (1): 59-67.
15.Cruz AG, Gomes AMT, Parreira PMD. Attitudes of nurses towards hospitalized elderly persons. Rev. enferm. UERJ. 2016; 24 (3): e14726.
16. Ministry of Health (Br). SUS Hospital Information System. Morbidity of SUS hospital, by place of hospitalization, Brazil. Brasília (DF): Ministry of Health, 2010.
17. Brazilian Institute of Geography and Statistics. Demographic census 2010: demographic trends in the period 1950/2000. [internet] 2010 [cited on 17 Jul 2017]. Available from: http://www.ibge.gov.br/home/estatistica/populacao/censo2000/tendencias_demograficas/comentarios.pdf
18. Ministry of Health (Br). National Health Council. Ethics and Research Commission. Resolution 466/2012 on research involving human beings. Brasília (DF): CNS; 2012.
19. Brazilian Institute of Geography and Statistics. Demographic census 2010: characteristics of the population and households, results of the universe. [internet] 2011 [cited in Sept. 30, 2017]. Available from: http://www.ibge.gov.br/english/estatistica/populacao/censo2010/caracteristicas_da_populacao/resultados_do_universo.pdf .
20.Oliveira BLCA, Thomaz EBAF, Silva RA. Association between color/race and health indicators for the elderly in Brazil: a study based on the National Household Sample Survey (2008). Cad. Public Health (Online). 2014; 30 (7): 1-15.
21.Victor JF, Ximenes LB, Almeida PC, Vasconcelos FF. Sociodemographic and clinical profile of elderly people assisted at the Basic Family Health Unit. Acta Paul. Enferm (Online). 2009; 22 (1): 49-54
22. National Sample Household Survey. Comments: indicators for the period from 2004 to 2009. 2010. [Internet] [cited in Sept 20, 2017]. Available from: http://www.ibge.gov.br/home/estatistica/populacao/trabalhoerendimento/pnad2009/comentarios2009.pdf
23. National Household Sample Survey. Comments: Indicators for the period from 2009 to 2011. [Internet] 2012. [cited in Sep 17, 2017]. Available from: ftp://ftp.ibge.gov.br/Trabalho_e_Rendimento/Pesquisa_Nacional_por_Amostra_de_Domicilios_anual/2011/Sintese_Indicadores/sintese_pnad2011
24. Pavão ALB, Werneck GL, Campos MR. Self-assessment of health status and association with socio-demographic factors, life habits and morbidity in the population: a national survey. Cad. Public Health (Online). 2013; 29 (4): 723-34.
25. Moraes JR, Moreira JPL, Luiz RR. Association between self-reported adult health status and location of the domicile: an ordinal logistic regression analysis using PNAD 2008. Ciênc. Saúde coletiva (Online). 2011; 16 (9): 3769-80.
26.Department of Information Technology of SUS. Health Information: Demographic and socioeconomic. [internet] [cited in Oct 17, 2017]. Available from: http://www2.datasus.gov.br/DATASUS/index.php?area=0206
27.Wagner JT, Bachmann LM, Boult C, Harari D, Renteln-Kruse W, Egger M, Beck JC, Stuck AE. Predicting the risk of hospital admission in older persons - validation of a Brief Self-Administered Questionnaire in three European countries. JAGS. 2006;54(8):1271-6.
28.Pereira EEB, Souza ABF, Carneiro SR, Sarges ESNF. Global functionality of hospitalized elderly. Rev. bras. geriatr. gerontol. (Online). 2014; 17 (1): 165-76.
29.Barreto MS, Marcon SS. Hospitalization due to hypertension problems in primary care patients. Acta paul. enferm. 2013; 26 (4): 313-7.
30.World Health Organization. Diabetes [internet]. 2013 [cited in Oct 2, 2017]. Available from: http://www.who.int/diabetes/en/
31. Alves RF, Silva RP, Ernesto MV, Lima AGB, Souza FM. Gender and health: the care of men in debate. Psicol. teor. prat. 2011; 13 (3): 152-66.
32.Gomes R, Nascimento EF, Araujo FC. Why do men seek health services less than women? Explanations of men with low schooling and men with higher education. Cad. Public Health (Online). 2007; 23 (3): 565-74.
33.Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, et al. Frailty in older adults: evidence for a phenotype. J. gerontol. Ser. A, Biol. sci. med. sci. 2001; 56:146-56.
34.Amaral FLJS, Guerra RO, Nascimento AFF, Maciel ACC. Social support and frailty syndrome in community dwelling elderly. Ciênc. Saúde coletiva (Online). 2013; 18 (6): 1835-46.
35. National Household Sample Survey: an overview of health in Brazil, access and use of services, health conditions and risk factors and health protection, 2008 [Internet]. 2010 [cited in Aug 17, 2017]. Available from: http://bvsms.saude.gov.br/bvs/publicacoes/pnad_panorama_saude_brasil.pdf
36.Góis ALB, Veras RP. Information on hospital morbidity in elderly patients in hospitalizations of the Brazilian Unified Health System. Ciênc. saúde coletiva (Online). 2010; 15 (6): 2859-69.