REVIEW ARTICLES
Characterization and spatial distribution of octogenarian men
Darlene Mara dos Santos TavaresI; Pollyana Cristina dos Santos FerreiraII; Flavia Aparecida DiasIII; Paula Beatriz de OliveiraIV
INurse. PhD in Nursing. Associated Professor of the Nursing Department in Education and Community Health of the Nursing Graduation Course of the Federal University of Triângulo Mineiro. Leader of the Research Group in Collective Health. Uberaba, Minas Gerais, Brazil. E-mail: darlenetavares@enfermagem.uftm.edu.br.ABSTRACT: The objective was to describe the socioeconomic profile, health and quality of life of octogenarian men; map the regions of concentration of the elderly by number of disability and morbidity. Analytical, observational and cross sectoral study involving 121 octogenarians men living in Uberaba-MG, in 2008. The instrument applied were: Brazilian Questionnaire and Multidimensional Functional Assesment (BOMFAQ), World Health Organization Quality of Life - BREF (WHOQOL-BREF) and World Health Organization Quality of Life Assessment for Older Adults (WHOQOL-OLD). Descriptive analysis and odds ratios were used. Elderly married, living with a spouse, illiterate and with 1├4 years of education, income of a minimum wage, with 1├4 disabilities and 4├7 comorbidades were predominated in the study. Older people with bigger number of morbidity and disability live in regions where there was no coverage by the Family Health Strategy. These results can contribute to the planning of directed health actions, considering the specificities of this population.
Keywords: Octogenarians; men's health; quality of life; spatial distribution.
INTRODUCTION
Population aging is a worldwide phenomenon and the age group growing faster currently is people 80 years ol or more1. This population growth is due to the increase in life expectancy. In Brazil, there was an increase of 3.1 years in the last ten years. However, life expectancy for men is still lower when compared to women, being 69.4 for men and 77 years old for women2.
Considering the lowest life expectancy and other aspects related to men´s health, as the socio-cultural and politic-economic, in 2008 the Ministry of Health launched the National Policy of Integral Attention to Men´s Health, in order to identify the main health problems, enabling the promotion of actions to increase the life expectancy of the population3.
However, studies assessing the human health are still scarce, taking into account the different age groups and focusing on the elderly4,5.
Research conducted in Piauí assessed the gender differences among elderly and found that men reported greater difficulties to experience this stage of life, expressed in accepting certain conditions from the aging process, such as: retirement, the physical, emotional, economic and social losses appearing as chronic diseases. They stressed the unwillingness to live without autonomy and with dependence often worsened after the death of loved ones. Older women, on the other hand, showed greater acceptance and adaptation to these factors4.
In this sense, it becomes necessary the development of research that address men´s health during the aging process, because of their peculiarities in this age group still little explored.
Thus, considering the needs to identify the specificities of enduring elderly and their distribution in a given population, this study aimed to: describe the socioeconomic profile of health and quality of life (QOL) of elderly octogenarians men; to verify the association of functional incapacity with education and income; and to map the regions of concentration of this population by number of functional incapacity and morbidities.
LITERATURE REVIEW
The octogenarians are characterized by heterogeneity in comparison to younger elderly. Among elderly 80 years old and older, it is observed since those totally care independent to dependent ones6.
In addition to the functional comitment and dependency, the enduring elderly have a higher risk to develop chronic-degenerativas diseases2. It should be noted that the increase in comorbidities can result in negative impact on QOL of the elderly7.
In this context, besides the health and functionality, there is a concern of health professionals in identifying the QOL of this population, while considering as one of the determinants of increase or decrease in longevity8.
The definition of QOL is considered wide and variablel8, being described by the World Health Organization as “an individuals´ perception of their position in life in the context of culture and value system in which they lives and in relation to their goals, expectations, standards and concerns”9:1405. From this perspective, it is necessary to identify the perception of octogenarians around the values, concerns and objectives that permeate their QOL.
In addition, the scientific literature shows that the environment can intervene on the elderly´s health10. However, there are few studies that have used this tool with a focus on health care for the elderly, and even less of the male octogenarians11.
Thus, it becomes relevant to know the location of this population, in order to verify the presence of spatial clusters which require greater care in health. For the analysis of these relationships it is necessary the use of technologies aimed at the collection and processing of spatial information applied to the health sector.
METHODOLOGY
This research is part of a larger study, conducted by the Research Group in Collective Health of the Federal University of Triângulo Mineiro (UFTM), in 2008, which described the situation of health of elderly residents in the urban area of Uberaba-MG. In 2008, Uberaba had 292,377 inhabitants, where elderly represented 11.8% of the population12.
The sample population, of the larger study was calculated considering 95% of confidence, 80% test power, error margin of 4.0% to intervalares estimates and an estimated proportion of π = 0.5 for the proportions of interest, corresponding to 2,142 elderly.
The present study has descriptive, analytical, transversal and observational design. Among the elderly 2,142 those 80 years old or more were included, which did not have cognitive decline, male gender, urban-area residents of Uberaba and who have agreed to participate. 121 elderly were according to the inclusion criteria.
For the cognitive evaluation Mini Mental State Examination (MMSE)13. Cognitive decline was when the elderly obtained score less than or equal to 12 points13.
For socioeconomic data collection, comorbidities and functional capacity part of the Brazilian Questionnaire and Multidimensional functional Assessment (BOMFAQ) were used14. The variables studied were: marital status, education, individual monthly income, activities of daily living (ADLs), number of functional incapacity for ADLs and morbidities. Functional disability was considered when the elderly could not perform certain ADL.
For analysis of QOL the World Health Organization Quality of Life-BREF (WHOQOL-BREF) was used15. It has 26 questions, in which two refer generically to QOL and the rest represent four areas composing the instrument: physical, psychological, social relations and environment15.
The module World Health Organization Quality of Life Assessment for Older Adults (WHOQOL-OLD) also was used, specific for elderly. It consists 24 Likert scale items assigned to six facets: functioning of the senses; autonomy; past, present and future activities; social participation; death and dying and intimacy16.
The data collected during the period from August to December 2008, were typed by two people, in double-entry, in Excel® program. After checking the consistency between databases, data were transported to the software Statistical Package for the Social Sciences (SPSS) version 17.0 for analysis. The data were submitted to descriptive analysis through simple frequencies for the variables categories and mean and standard deviation for the numeric ones. To check associations the unadjusted odds ratio was used. Each domain of the WHOQOL-BREF and facet of the WHOQOL-OLD were analyzed separately, with their respective syntaxes. The scores range from 0 to 100 points, with the highest scores corresponding to greater QOL.
As for the spatial analysis, the programs MapInfo Professional 9.5 version and Terraview version 3.3.1 were used. For the elderly mapping, coordinates Universal Transverse Mercator (UTM), model of the Earth (SAD-69) were used, collected by the program Google Earth. Addresses not found on this program were collected by appropriate equipment, like Global Positioning System (GPS) type. The intensity of the events (number of events per unit area) was estimated by the Kernel estimation with adaptive radius of quartic function; each cell equivalent to 250 m.
The research was approved by the Ethic Committee in Research with Human Beings from UFTM, Opinion n° 897. The elderly were contacted at their homes, were presented the objectives of the research, the Informed Consent Term and provided relevant information. After the consent of the elderly and the signature of the Term, the interview started.
RESULTS AND DISCUSSION
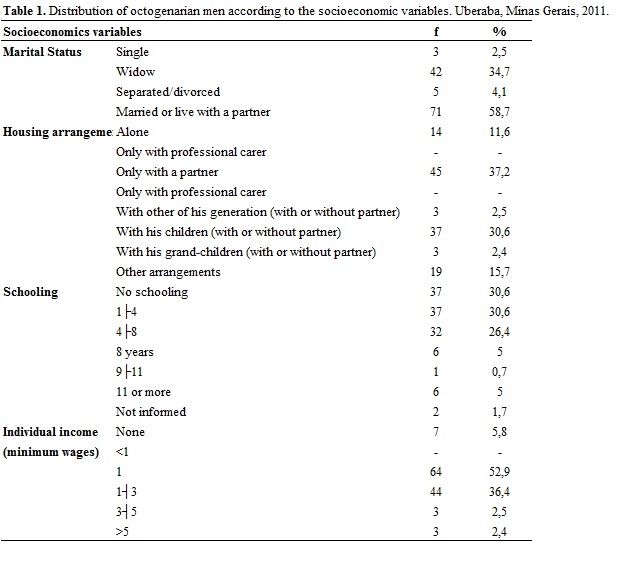
Most octogenarians men were married or lived with a partner 71 (58.7%), Table 1. Similar to the results achieved in the municipality of São Paulo that 69.8% of octogenarians men were married17. Research conducted in England presented lower percentage for octogenarians men (47%)18.
There is a tendency of men to marry with younger women and build new marital ties in widowhood, unlike women who tend to remain alone19. Living with a partner can contribute to the maintenance of the family link and support of the elderly.
It is hghlighted that 42 elderly (34.7%) were widows, according to Table 1. Similar found among octogenarians men in the municipality of São Paulo (34.1%)20. Changes to the familiar arrangement in this age group impose the need for readaptations17. Research found that among octogenarians men, widowhood is related to low satisfaction with life21. The nurse together with the elderly must seek alternatives to facilitate adaptations of this new family condition.
For the family and housing arrangement, those living only with the spouse have predominated, 45 (37.2%) according to the Table 1. Domiciliary inquiry held in Sao Paulo with older elderly presented higher percentage among men (55.1%)17. The presence of the spouse may be reflected in increased support to the octogenarian man. However, health professionals should be alert to the potential physical and emotional overload which can affect the caregiver, usually to the partner or wife of the elderly.
The illiterate elderly prevailed 37 (30.6%) and with 1├4 years of study 37 (30.6%), Table 1. Study conducted in Ribeirão Preto-SP verified higher percentage for octogenarians men with 1├4 years of study (70.4%) and lower for those without education (12.2%)17.
Education is a determining factor in the choice of the life habits of this population, and may interfere with the maintenance of the healthy aging and contribute to the occurrence of morbidities such as dementia20,22. In this sence, health professionals should be trained to develop strategies for health promotion and disease prevention, considering the educational level of the elderly.
The individual monthly income of most octogenarians, 64 (52.9%) was a minimum wage, as showed in the Table 1. This result is different in a research in the interior of São Paulo, in which octogenarians men received one to three minimum wages (62.3%)17.
It is known that a significant portion of Brazilians elderly, does not currently obtain their financial resources through paid labour activities. Thus, the pension system and assistance actions are key to minimize the negative impact of low incomes in population health23.
As for the functional capacity, 80 (66.1%) of octogenarians men were independent. Different result was found in an investigation conducted in England, where among the octogenarians, 66.3% had disabilities in ADLs basic and instrumental activities in of daily life (AIDL)18.
It is highlighted that 33 (27.3%) reported 1├5 disability and 8 (6.6%), five or more disabilities. The functional incapacity most frequent for the ADL was cutting the toenails - 37 (30.6%) and those related to mobility: up and down stairs - 16 (13.2%), walking close to home - 11 (9.1%) and walking - 8 (6.6%). In a previous study conducted in the same municipality, octogenarians men without difficulty to perform these activities have been predominant. However, when compared to the age groups, the degree of difficulty for performing ADLs rose with advancing age24.
These results suggest the need to investigate the factors generating the octogenarian´s dependence on the performance of ADLs related to mobility. During the aging process the man can experience losses and limitations that affect the physical and emotional health, leading to diseases problems4.
In this context, the possible limitations from the loss or reduction of mobility, as higher risk for falls, greater dependency and reduced social relations may interfere negatively in the QOL of the elderly. Health professionals can implement in the APS educational activities among the elderly and their families about the readjustment of the domiciliary environment, according to the needs identified among the octogenarians. Thus, it is stimulated safely and independently ADLs performance, favoring the maintenance of functional capacity.
The ADLs performed with great difficulty are the ones related to mobility, such as going up and down stairs - 22 (18.2%), walking - 15 (12.4%) and walk close to home - 12 (9.9%). In England, it was found that 42.1% of the octogenarians had limitations related to mobility18. It is possible that the difficulties and limitations to develop ADLs are related to the presence of chronic-degenerative diseases in this population, limiting the independence of older people25.
Concerning morbidities, 39 (32.2%) elderly reported 4├7, 36 (29.8%) mentioned 7├10, 26 (21.5%) between 1├4 and 18 (14.9%) among 10 or more morbidities. Only 2 (1.7%) elderly did not present morbidities. Among the morbidities, there were vision problems of elderly in 93(76.9%), cataracts in 69 (57%) and arterial hypertension in 68 (56.2%).
As for vision problems, other investigations carried out with octogenarians converge with this study18,20. The vision problems in the elderly bring concern since they can corroborate for the increase in accidents like falls20. Early identification of the problems of vision and the actions directed to correction or reducing this problem may contribute to the minimization of the falls, in addition to being a factor that favors the development of activities and social interaction.
In hypertension, in inquiry based on National Research for Sample of Domiciles (NRSD) the prevalence of hypertension was 36% among octogenarians men, lower than that obtained in this research26.
The octogenarian man incentive in maintaining healthy habits of life, involving the practice of physical activity, feeding, the abolition of the consumption of alcohol and tobacco and conducting routine examinations, contribute to the prevention of health problems, such as high blood pressure.
The self-evaluation of QOL showed that most of them, 88 (72.7%) consider it as good. Among octogenarians, satisfaction with life can be related to improving the state of health, particularly among men, as observed in a longitudinal survey conducted in Switzerland21.
Regarding their health, 88 (72.7%) were satisfied. Different result of these findings, NRSD study noted that the highest percentage of octogenarian men considered his health as regular (24.2%)26.
The analysis of QOL, according the WHOQOL-BREF, presented bigger scores in social relations (68.87), according to Table 2. Similar result obtained in a survey conducted with elderly octogenarians men and even nonagenarians, but with higher average score (78.22)27. Study conducted in Switzerland found that satisfaction with the quality of the social network was related to higher life satisfaction among octogenarians21. This domain assesses personal relationships, social support and sexual activity15. In this investigation, the highest score in this area can be related to marital status, since the highest percentage of elderly had stable relationship. It is possible that the elderly with a partner report better perception of social support.
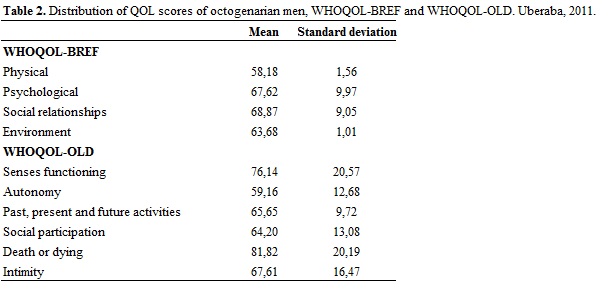
The lowest score of QOL was to the physical domain (58.19), Table 2. Similar result to the one achieved by octogenarians and even nonagenarians in a research conducted in Rio Grande do Sul (59.88)27.
Considering this area evaluates, among other factors, pain and discomfort, activities of everyday life, dependence on medication or treatment, it is assumed that the elderly have impacted morbidities have negatively impact on their QOL. Moreover, this fact may be related to the predominance of disabilities still functional mobility activities, thus affecting their independence and their daily life.
Social visibility of the aging process, even today, are culturally linked to loss of physical and mental abilities and the insertion of fragility. Thus, at this stage of life the man seeks to move away from the possibility of being considered fragile, common to the feminine universe, by the stigma of compromising his masculinity. So, they tend to show agile and with vitality28.
It is highlighted that the man usually do not search the APS service to carry out health promotion and disease prevention. Often, their access to health services occurs through the specialized attention, in the search for the recovery of damages. It should be noted that the resistance of man to seek on a regular basis the means of primary prevention of diseases echoes not only in financial overload for society, but primarily in physical suffering to the octogenarian and in emotional distress, and the repercussions for the family3.
The multidisciplinary team through health education activities can reinforce the need for the service to men in this age group emphasizing health promotion and disease prevention.
The QOL measured by WHOQOL-OLD obtained higher scores on the facet death and dying (81.83) according to Table 2. Among elderly, the longevity is faced with fears and concerns about the finiteness of life. However, the acceptance of death at that moment of life can bring comfort and peace to the elderly, contributing to better QOL of octogenarians29.
The lowest score was obtained in the facet of autonomy (59.17), according to Table 2. The loss of autonomy, as well as social isolation, the decline of functionality and the presence of chronic diseases can impact negatively on QOL of the elderly27. It is possible to ensure the autonomy of the elderly offering opportunities for choice, as for example, in the clothes he wants to wear, food of his choice, where he wants to sightsee, among others. The important thing is to recognize their capabilities and potentialities stimulating them in decisions, in order to enjoy their rights and maintain their physical and existential space30.
Education association was not observed (p=0,916; OR=0,95; IC=0,42-2,16) and income (p=0.353; OR=0.36;IC= 0.08-1.69) with the number of functional incapacity. Different results to those found in research in Minas Gerais, where not having education (OR=2.8;IC=1.7-4.8) and having low income (OR=2.7;IC=1.3-5.5) were associated with the functional disability31. However, in the study of Minas Gerais, they considered elderly men and women in different age groups, which may have contributed to the results obtained, different from this research.
In relation to spatial analysis, it was showed the concentration of elderly octogenarians in the southeast of the city of Uberaba and in lower density close to the central region. This fact may be related to the characteristics of urbanization of the municipality, revealing areas that need directed care, given the relationships between space and health.
The southeastern region has health services for primary and secondary care, even there are areas in this region where coverage by Family Health Strategy (FHS) is partial.
In this context, it is important that the health services of these localities, as the FHSs, prioritize a plan of attention to old octogenarian directed to spatial clusters, seeking him actively. In this way, it can contribute to the monitoring of their health needs, as well as establish actions aimed at improving their QOL considering the most affected aspects.
The elderly without functional disability were in the southeast of the city, those with 1├4 disability in the northeast and with 4 or more in the southwest. There was major clusters of elderly with the highest number of disability in peripheral regions of the municipality.
It is highlighted that the region southwest of the city, where there are more elderly with four or more functional disabilities for ADLs performing, lacks coverage by the FHS. Thus, it should be noted the need for governmental actions being prioritized in those locations in order to establish the monitoring of those elderly through the APS, with views to the maintenance and rehabilitation of the old functionality.
Elderly with 1├4 morbidities focused on southeast region of Uberaba, those with 4├7 in the southwest and northwest regions, with 7├10 in north near the central region, and 10 and more in south, next to the central region.
Those regions which elderly with greater number of morbidities also do not have coverage of the FHS. It should be noted that the basic care is a privileged field for the development of practices of care, by encouraging knowledge of the context in which the population lives, as well as their needs for assistance strategies32.
Thus, it is very important the expansion of services in the APS, so as to comply with the principles proposed by the Unified Health System (SUS), among them, the equity and universality, in order to dicrease the impact of diseases in the QOL of octogenarians elderly.
CONCLUSION
Octogenarians married or living with a partner, residing only with spouse, without education or with 1├4 years of study and individual monthly income of a minimum wage have predominated. Regarding the functional incapacity, 1├3 and 4├7for comorbidities. Education and income were not linked to the number of functional incapacity for performance of the ADLs.
The QOL measured by the WHOQOL-BREF showed the highest score in the social relations, and lowest in the physical domain. In the WHOQOL-OLD higher scores on death and dying facet and lower for autonomy were obtained.
The spatial analysis showed concentrations of octogenarians in the southeast of the municipality and in lower density close to the central region. The elderly with a greater number of functional incapacity were concentrated in peripheral regions and those with the largest number of comorbidities in the north and south, next to the central region.
These results reinforce the need of health service direct strategies to the needs of the octogenarian man. It is highlighted the need for expansion of the coverage of the APS, in addition to tracking and monitoring actions of morbidities and stimulating functionality with a view to maintaining autonomy and independence.
The lowest scores in the physical domain and autonomy facet show that the QOL of the elderly appears more compromised in these aspects. Thereby, health professionals should investigate the factors that have impacted negatively the QOL of this population, seeking possible solutions together to the elderly and their families.
The interaction of data concerning the socio-economic profile and the spatial distribution of octogenarian men can contribute to the planning of actions in directed health, considering the specificities of this population.
REFERENCES
1. Kirkwood TBL. A systematic look at an old problem: as life expectancy increases, a systems-biology approach is needed to ensure that we have a healthy old age. Nature. 2008; 451:644-7.
2. Brazilian Institute of Geography and Statistics. Synthesis of social indicators: an analysis of the living conditions of the population. Rio de Janeiro: IBGE; 2010.
3. Ministry of Health (Br). National Policy Integral Attention to Men's Health. Brasília (DF): Ministry of Health; 2008.
4. Figueiredo MLF, Tyrrel MAR, Carvalho CMRG, Luz MHBA, Amorim FCM, Loiola NLA. Gender differences in old age. Rev Bras Enferm. 2007; 60:422-7.
5. Couto MT, Pinheiro TF, Valença O, Machin R, Silva GSN, Gomes R, et al. The man in primary health care: discussing (in) visibility from the gender perspective. Interface–Comunic, Saude, Educ. 2010; 14:257-70.
6. Schmidt JA, Dal-Pizzol F, Xavier FMF, Heluany CCV. Application of the test clock in octogenarians and nonagenarians participants study in Siderópolis/SC. Psico. 2009; 40: 525-30.
7. Lima MG, Barros MBA, César CLG, Goldbaum M, Carandina L, Ciconelli RM. Impact of chronic disease on quality of life among the elderly in the state of São Paulo, Brazil: a population-based study. Rev Panam Salud Publica. 2009; 25: 314-21.
8. Alencar NA, Souza Jr. JV, Aragão JCB, Ferreira MA, Dantas E. Physical activity, functional autonomy and quality of life in active elderly and sedentary. Fisioter Mov. 2010; 23: 473-81.
9. The Whoqol Group. The world health organization quality of life assessment (WHOQOL): position paper from the world health organization. Soc Sci Med. 1995; 41: 1403-9.
10. Poortinga W, Dunstan FD, Fone DL. Perceptions of the neighbourhood environment and self rated health: a multilevel analysis of the Caerphilly Health and Social Needs Study. BMP Public Health. 2007; 7:785-85.
11. Magalhães MR, Corrente JE, Ruiz T, Simões LB. Spatial distribution of the elderly according to their concepts of quality of life. Rev APS. 2008; 11:374-9.
12. Ministry of Health (Br). DATASUS [internet site]. Health information. Resident population in Minas Gerais 2008. [cited in 25 Mar 2014]. Available in: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?ibge/cnv/popmg.def.
13. Icaza MC, Albala C. Projeto SABE. Minimental State Examination (MMSE) del estudio de dementia en Chile: análisis estatístico. Brasília (DF): OPAS; 1999.
14. Ramos LR. Growing old in São Paulo, Brazil. Assessment of Health status and family support of the elderly of different socio-economic strata living in the community [thesis]. London (UK): London School of Hygieni and Tropical Medicine; 1987.
15. Fleck MPA, Lousada S, Xavier M, Chachamovich E, Vieira G, Santos L, et al. Application of the Portuguese version of the abbreviated instrument for assessing the quality of life WHOQOL-BREF. Rev Saude Pública. 2000; 34:178-83.
16. Fleck MP, Chachamovich E, Trentini C. Development and validation of the Portuguese version of the WHOQOL-OLD module. Rev Saude Publica. 2006; 40:785-91.
17. Pedrazzi EC, Motta TTD, Vendrúsculo TRP, Fabrício-Wehbe SCC, Cruz IR, Rodrigues RAP. Living arrangement of older elderly. Rev Latino-Am Enfermagem [Online]. 2010 [cited in 18
Mar 2014]. 18(1):08 telas. Available in: http://www.scielo.br/pdf/rlae/v18n1/pt_04.pdf.
18. Zhao J, Barclay S, Farguhar M, Kinmonth AL, Brayne C, Fleming J. The oldest old in the last year of life: population-based findings from Cambridge City over-75s cohort study participants aged 85 and older at death. J Am Geriatr Soc. 2010; 58:1-11.
19. Lebrão ML. Aging in Brazil: aspects of demographic and epidemiological transition. Saúde Coletiva. 2007; 4:135-40.
20. Ferreira JVC. The older in city of São Paulo [dissertation]. São Paulo: University of São Paulo; 2006.
21. Berg AI, Hoffman L, Hassing LB, McClearn GE, Johansson B. What matters, and what matters most, for change in life satisfaction in the oldest-old? A study over 6 years among individuals 80+. Aging Ment Health. 2009; 13:191-201.
22. Ribeiro PCC, Nen AL, Cupertino APFB, Yassuda MS. Variability of active aging by gender, age and health. Psicologia em Estudo. 2009; 14:501-9.
23. Neri MC, Soares WL. Estimating the impact of income on health through income transfer to the elderly low-income programs in Brazil. Cad Saúde Pública. 2007; 23: 1845-56.
24. Tavares DMS, Pereira GA, Iwamoto HH, Miranzzi SSC, Rodrigues LR, Machado ARM. Functional disability among elderly residents of a municipality in Minas Gerais. Texto contexto – enferm. 2007; 16:32-9.
25. Camarano AA, organizador. Long-term care for the elderly: a new social risk to be assumed? Rio de Janeiro: Institute of Applied Economic Research (IPEA); 2010.
26. Lima-Costa MF, Barreto SM, Giatti L. Health conditions, functional status, use of health and drug spending among Brazilian elderly services: A descriptive study based on the National Sample Survey of Households. Cad Saúde Pública. 2003; 19:735-43.
27. Chepp CC. Cross-sectional study of quality of life through the scale of WHOQOL-BREF octogenarian and nonagenarian population of Siderópolis [monograph]. Criciúma (SC): University of Extremo Sul Catarinense; 2006.
28. Fernandes MGM, Garcia LG. The meaning of old age for elderly men and women. Saúde Soc. 2010; 19:771-83.
29. Maues CR, Paschoal SMP, Jaluul M, França CC, Jacob-Filho W. Evaluation of quality of life: comparison between young and elderly very elderly. Rev Bras Clin Med. 2010; 8:405-10.
30. Celich KLS. Domains of quality of life and capacity for decision-making in elderly participants of the third age group [thesis]. Porto Alegre (RS): Catholic University of Rio Grande do Sul; 2008.
31. Nunes MCR, Ribeiro RCL, Rosado LEFPL, Franceschini SC. Influence of demographic and epidemiological characteristics and functional capacity in elderly residents of Ubá, Minas Gerais. Revista Brasileira de Fisioterapia. 2009; 13:376-82.
32. Kebian LVA, Acioli S. Home visit: a place for health care practices by nurses and community health agents. Rev enferm UERJ. 2011; 19:403-9