ORIGINAL RESEARCH
Mapping of nursing diagnoses, results and interventions in an oncology unit
Myria Ribeiro da SilvaI; Dejeane de Oliveira Silva II; Tássia Irineu dos SantosIII; Patrícia Peres de Oliveira IV; Andrea Bezerra RodriguesV; Dulce Aparecida BarbosaVI
I
Nurse. Ph.D. Adjunct Professor. State University of Santa Cruz. Bahia,
Brazil. E-mail: myriarib@uol.com.br
II
Nurse. Ph.D. Adjunct Professor. State University of Santa Cruz. Bahia,
Brazil. E-mail: dejeanebarros@hotmail.com
III
Nurse. State University of Santa Cruz. Bahia, Brazil. E-mail: tassiairineu@gmail.com
IV
Nurse. Ph.D. Adjunct Professor. Federal University of São João del-Rei.
Divinópolis, Minas Gerais, Brazil. E-mail: pperesoliveira@gmail.com
V
Nurse. Ph.D. Adjunct Professor. Federal University of Ceará. Fortaleza,
Ceará, Brazil. E-mail: andreabrodrigues@gmail.com
VI
Nurse. Ph.D. Associate Professor. Federal University of São Paulo. São
Paulo, Brazil. E-mail: dulce.barbosa@unifesp.br
DOI: http://dx.doi.org/10.12957/reuerj.2017.15133
ABSTRACT
Objective: to identify the main nursing diagnoses, interventions and results described by the North American Nursing Diagnosis Association (NANDA), Nursing Outcomes Classification (NOC), and Nursing Intervention Classification (NIC), for cancer inpatients. Method: this quantitative cross-sectional study was conducted between March and October 2014 at the oncology unit of a philanthropic hospital in south Bahia State in a sample of 157 patients. Data were analyzed by descriptive statistics. Results: seven NANDA diagnoses, 12 NOC outcomes and 12 NIC interventions were highlighted. The main diagnoses, results and interventions/activities were considered to be those formulated for more than 78 (50.0%) of the study participants. Conclusion: it was possible to identify and select nursing diagnoses, interventions and results for application in clinical practice, with a view to informing the care process and knowledge of nursing taxonomies.
Keywords: Nursing process; neoplasms; oncology service, hospital; nursing care.
INTRODUCTION
According to the World Health Organization (WHO), cancer is the leading cause of death worldwide1,2 and it can reach about 21.4 million new cases by 2030 and 13.2 million will die due to aging and population growth, as well as the reduction of infant mortality and deaths from infectious diseases2,3. According to the National Cancer Institute (INCA), the estimated number of new cancer cases in 2016 was 596,000 in Brazil3.
These data point to the need for preventive and control actions considered today important challenges for public health and for the scientific community4. Therefore, the performance of professionals who maintain full, effective and excellent quality care is essential 4,5.
Thus, it is fundamental that besides to curative care, professionals are capable of performing the early detection of cancer risk factors, as well as organizing strategies for their prevention4. These behaviors may contribute to reducing mortality for many types of malignant neoplasm or even improving the quality of life of people with cancer.
Therefore, nursing can act based on the identification of human responses and the establishment of strategies that provide for the recovery of health or the improvement of an individual or collective well-being. For this, the nurse needs to use tools such as the nursing process (NP), which is a way of systematizing the care provided to the person, family or community, focusing on the integrality of care and the interaction between professional-patient-family4,6,7. NP is based on scientific reasoning, clinical reasoning provides the provision of humanized care and involves five moments: research, nursing diagnosis, planning, implementation, and evaluation6,7.
The reception and care of the cancer patient are complex due to the characteristics of the illness, requesting responsibilities from the nurse that is exclusive to him, knowledge and technical-scientific skills, as well as interpersonal skills4.
The Brazilian Federal Nursing Council regulated the Systematization of Nursing Care (SAE), through Resolution number 358/2009, and this implies the employment of the NP in all the public and private health institutions of the country8.
Standardized nursing languages were developed, such as NANDA9, NOC10, and NIC11 to reach the scientificity and to meet this precision.
Considering the complexity of the subject, the question was: what are the diagnoses, results and nursing interventions present in hospitalized patients?
The motivation of this research came from being an unexplored topic of great importance. There are few publications in the area of oncology nursing, involving the NP, indicating the need to establish the mapping of the main diagnoses, results and nursing interventions/activities to achieve better care for cancer patients, since it allows nurses to identify with the needs of care for the people for whom they are responsible. From this perspective, this study is of great importance for the nursing professional.
The aim of this study was to identify the main nursing diagnoses, interventions and outcomes described by the North American Nursing Diagnosis Association (NANDA), Nursing Intervention Classification (NOC), for inpatient cancer patients.
LITERATURE REVIEW
The term cancer is used to represent a set of more than 100 diseases, with diverse origins and causes. Among the main risk factors for the development of the disease are the inadequate life habit, smoking, and genetic inheritance, being the lifestyle responsible for more than 80.0% of the cases of cancer1-3.
From a genetic mutation, the cancer cells can accumulate. The main characteristic of the malignant tumor is its capacity to destructively invade other places than its origin and to spread by metastasis to distant parts of the body4,6.
The choice of treatment depends on the type of cancer and it should be comprehensive, it can be done through surgery, radiotherapy, chemotherapy, hormone therapy, immunotherapy or bone marrow transplantation 6,12. Due to its effects, the patient needs attention to his physical, psychological and social needs, including family participation 6, because the illness requires re-adaptation and coping strategies for the new situations13.
Health professionals who live with people with cancer perceive that such a disease causes a great emotional and social impact on the family and the individual who experiences this disease. Also, it requires constant restructuring, entailing a continuous challenge of the person for his body, his family, his social role, his future plans and his personal values 4.
Critical reasoning provides a foundation for nurses to plan patient/client, family, or community care4,6. ND provides a clinical judgment of the person´s responses to current or potential health processes or health problems. In this way, it allows establishing subsidies for the identification of nursing interventions that achieve the best health outcomes that nurses are responsible5-7. Together with ND, the NANDA9, NOC10, and NIC11 classifications are used to systematize nursing care and nursing interventions and outcomes can provide adequate foundations for evidence-based guidelines7.
In this context, the nursing team has the responsibility of assisting the individual with cancer and his/her family, both physically and psychologically, and health care. For this, nurses must use NP 8,14, based on the knowledge inherent to NANDA, and together with the evidence-based interventions of NIC and patient-sensitive outcomes within the NOC will support the contributions of the profession to patient care, adding value to the health team and visibility for the profession 7,15.
METHODOLOGY
This is a cross-sectional study with a quantitative approach, carried out at the oncology unit of a public hospital located in the southern region of the state of Bahia, Brazil. Based on convenience sampling. The inclusion criteria were cancer patients admitted to that hospital, from March to October 2014, and who agreed to participate in the study by completing and signing the Informed Consent Term (TCLE). There were 157 patients participating in the study.
The inclusion criteria in the research were people aged over 18 years, with the oncological disease, conscious, and the level of consciousness was verified by applying the Glasgow Coma Scale, with a score equal to 15.
Anamnesis and clinical examination were carried out to collect data and the clients' medical records as a secondary source of data, in particular the history (research form), evolution and nursing annotations, since these provide information addressing the requirements of nurses provided, those related to the development of the health condition, containing questions related to sociodemographic data, surgical and disease antecedents, as well as laboratory data.
The study was submitted and approved by the Research Ethics Committee of the State University of Santa Cruz/UESC, opinion number 436807/2013. Before the collection, a formal request for authorization to collect the data was made to the person responsible for the oncology unit.
The study participants were informed about the purpose of the study, the confidential nature and possibility of interruption of their participation without any type of harm, after the acceptance, they signed the TCLE.
The data processing was performed in Epi Info software version 7, with double entry to ensure database consistency. The analysis was performed in the Statistical Package for Social Science, version 20.0, by absolute and relative frequencies to obtain the frequency of nursing diagnoses, results and interventions obtaining a profile of the NP, ND scores, results and interventions/activities were formulated for more than 78 (50.0%) of the study participants.
The ND, results and interventions/activities were compared with the literature and evaluated by three experts in the field that is more than ten years of practice in the profession, with master's and/or completed doctorate, publications in congresses, books and/or journals indexed in the area of diagnosis, results and nursing interventions in the last five years.
RESULTS AND DISCUSSION
Of the 157 cancer patients participating in the study, 121 (38.2%) were in the age from 18 to 91 years old, with a mean age of 54 years old and 85 (54.2%) were female patients. Similar data were found in the incidence of cancer in Brazil, for the state of Bahia, where 52.0% of the cases of cancer are women3. The insertion of women in the labor field and the consequent alteration of the gender roles and social relationships corroborated the commitment of women's health since other risk factors facilitate the involvement of chronic diseases and the susceptibility to cancer in the women of modern society12.
Regarding the current occupation, 58 (37.0%) of the patients were retired, 80 (51.0%) received up to two minimum wages, corroborating data found in the literature4,16.
It was possible to verify an average of seven days of hospitalization, with the longest stay of 39 days, and the main type of malignant neoplasm was the cervix, reaching 31 (19.7%) of the patients, followed by prostate cancer in 16 (10.4%) men, malignant head and neck neoplasia with 12 (7.8%), lung cancer 11 (7.4%), esophageal cancer 11 (7.4%), breast neoplasm 7 (4.6%), Hodgkin's lymphoma 6 (3.7%). In 5 (3.2%) cases there were each of the following malignancies: rectal, b-cell lymphoma, ovary, spinal column, hepatic, non-Hodgkin's lymphoma, leukemia, skin, brain, colon, pancreas, and multiple myeloma e; only 1 (0.6%) patient with penile cancer.
Breast cancer in women in the state of Bahia is the most prevalent, followed by cervical cancer; in men, prostate cancer had a higher incidence, followed by colon and rectum cancer3.
The reasons for hospital admission verified in the study were: 36 (23.0%) cases due to fatigue and anorexia, described in the records analyzed. Subsequently, 33 (21.0%) participants were admitted for antineoplastic treatment, 25 (16.0%) patients due to febrile neutropenia, 24 (15.0%) cases were related to pain. Then, there were hospitalizations of Anasarca in 11 patients (7.0%), hemotransfusion due to anemia and thrombocytopenia, in 11 (7.0%), pleural effusion in 9 (6.0%), hemorrhage in 6 (3.8%), palliative treatment in 2 (1.2%).
In this study, the use of ND was understood as a work tool to be accomplished in the daily routine of the nurse, facilitator of its process, because it presents a specific terminology for nursing and with that, it provides more autonomy17.
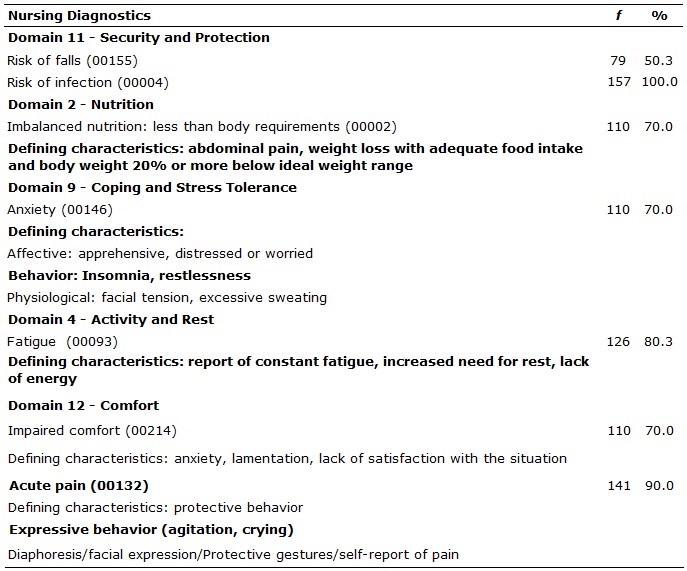
It is important to show the most ND frequent based in NANDA9, followed by the defining characteristics, related and risk factors that gave support to their elaboration. Two NDs belonging to the safety and protection domain were identified: risk of falls with 79 (50.3%) and risk of infection with 157 (100%) and comfort domain: impaired comfort with 110 (70.0%) and acute pain with 141 (90.0%), according to Table 1.
Table 1:
Defining characteristics, related and risk factors of nursing diagnoses of
patients with the oncological disease (N=157). Itabuna-BA, Brazil, 2014
The risk of falls detected in 79 (50.3%) patients conceived as a vulnerability for falls that can cause physical damage, was related to fatigue, anemia, unknown environment (hospital), old age for the elderly, use of anxiolytics.
The risk of infection ND is defined as the increased risk of the individual being invaded by pathogenic organisms9. It is the most present in hospitalized patients, due to several factors of the hospitalization process, demanding a preventive attitude that should guide nursing actions in the care plan, considering their interconnection with other ND 4. In this study, the risk of infection was associated with treatment-related factors (chemotherapy, radiotherapy, the presence of invasive routes, drug therapy), as well as neutropenia, thrombocytopenia, and anemia.
The prevention and control of infection demand technical and behavioral measures, repercussions on the quality of health, and consequent reduction of efforts, problems, complications, and costs4,16.
Regarding the comfort domain, the ND of impaired comfort is defined as the perceived lack of sense of comfort, relief and transcendence in the physical, psychospiritual, environmental, cultural and social dimensions. 9 The defining characteristics were: anxiety, mourning, and lack of satisfaction with the situation. The related factors included: treatment-related side effects, lack of control of the situation, symptoms related to the disease.
The comfort of the patient is considered paramount for his recovery since it can be understood as physical and mental well-being. The understanding of comfort conglomerates calm which means tranquility or satisfaction, relief not to have discomfort, and transcendence that is the stage of overcoming pain4,16.
Acute pain is defined as an unpleasant sensation that arises from actual or potential tissue injury; sudden or slow onset, of mild to severe intensity, lasting less than six months.9 Pain is a subjective experience, its perception is made by the personal report or demonstration of the pain sufferer, oncological pain, an expression used for to characterize the pain, in most cases of multiple etiologies that add up and potentiate, of a person with cancer4.
Regarding the nutrition domain, the ND of unbalanced nutrition: less than the body needs were identified in 110 (70.0%) of respondents, defined as insufficient intake of nutrients to meet metabolic needs9. The defining characteristics were: abdominal pain, weight loss with adequate food intake and body weight 20.0% or more below ideal. Related factors were: impaired ability to absorb food, impaired ability to digest food, impaired ability to ingest food, biological factors.
Most of the individuals with cancer present caloric-protein malnutrition. This factor is justified by the imbalance between the intake and the nutritional needs of these patients, compromising their nutritional status, which leads to an increase in morbidity and mortality in cancer and favoring cachexia, one of the complications in patients with malignant neoplasia12,14.
Regarding the domain coping/tolerance to stress, there were: anxiety 110 (70.0%), understood as an uncomfortable feeling of discomfort or fear; a feeling of apprehension motivated by the anticipation of danger9 . The main factors were: threat and change in health status. It was found as affective defining characteristics: to show being apprehensive, distressed or worried; behavioral: restlessness and insomnia; physiological: facial tension and increased perspiration. Studies indicate that several characteristics of cancer and its treatment can affect mental and physical balance, leading to anxiety4,12.
In the activity/rest domain, the ND of fatigue was identified in 126 (80.3%) of the patients, characterized by constant fatigue, increased need for rest, lack of energy; related to anemia and malnutrition. Fatigue is frequent in people with cancer, but little valued and considered as an expected and acceptable effect in individuals with malignant neoplasia 4. Also, there are reports of the subjective experience of generalized fatigue, weakness, exhaustion and lack of energy, related to prolonged stress12.
Before proceeding to the nursing outcomes and interventions, it is important to note that studies on ND are diverse. On the other hand, those investigating the results according to NOC10, and interventions according to IAS11 are still scarce, especially in care to cancer patients.
Initially, 43 different NOC10 results were used for cancer patients. Of them, 12 results were formulated for more than 78 (50.0%) of the study participants. With the help of the NOC10, it was possible to evaluate and quantify the cancer patient's condition, allowing precise and prioritized interventions. Nursing results based on the Nursing Results Classification (NOC)10 of the participants with cancer are shown in Table 2.
Table 2:
Nursing Outcomes of patients with the oncological disease (N=157).
Itabuna-BA, Brazil, 2014
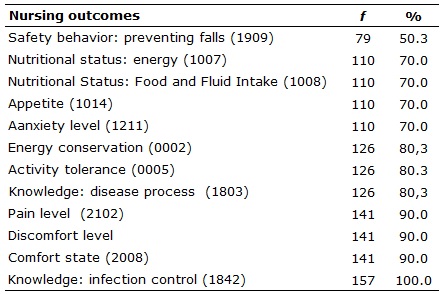
The 12 established results were knowledge: safety behavior: prevention of falls 79 (50.3%), nutritional status: energy 110 (70.0%), nutritional status: food and fluid intake 110 (70.0%), appetite 110 (70.0%), anxiety level 110 (70.0%), energy conservation 126 (80.3%), activity tolerance 126 (80.3%), knowledge: 3%), pain level 141 (90.0%), discomfort level 141 (90.0%), comfort state 141 (90.0%), knowledge: infection control (100.0%).
Nursing interventions/activities for cancer participants were comprehensive and justified by the variety and complexity of oncological diseases found. Guidelines are initiated and tailored to the needs of patients. Interventions and respective nursing activities based on the Classification of Nursing Interventions (NIC)11 of the study participants with cancer are presented in Table 3.
Table 3:
Nursing interventions and their respective activities of patients with the
oncological disease (N=157). Itabuna-BA, Brazil, 2014
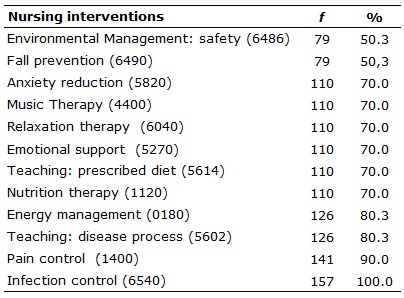
Regarding the interventions of NIC11, 48 interventions were implemented for the cancer patients, but 12 of them were applied in more than 78 (50.0%) of the study participants, being: environmental control: safety 79 (50 (70.0%), 110 (70.0%), relaxation therapy 110 (70.0%), emotional support 110 (70.0%), (80.3%), teaching: process of the disease 126 (80.3%), teaching of the disease 126 (80.3%), %), pain control 141 (90.0%), infection control 157 (100.0%).
The results of this research were presented in a meeting with all the nursing professionals of the oncological unit of the hospital scenario of the study to provide a reflection and possible changes, both technical-scientific and respect for the individuality of the people, since it is something possible and needs to be built together, between nurses and patients of the cancer area.
CONCLUSION
This study addressed the NANDA, NOC and NIC classifications in an oncology unit of a philanthropic hospital in the southern region of Bahia. It was possible to identify how the SAE, through the use of NP, can stimulate the assistance.
The identification of NDs, results and nursing interventions from this study provided new knowledge regarding oncological patient care, as well as the reach of systematized nursing practice for the authors and nursing professionals of the hospital setting of this research. Also, the clinical data accumulated using the terminology classified in the NANDA, NOC, and NIC provided information to support the development of parameters for the practice of nursing care in people with cancer.
It is worth stressing the limitations of the study because, although it covers the NP for cancer patients, this is not an absolute reality for all people with cancer, the unpredictability of the course of care to the individual, while being unique, may bring other impositions and conflicts that should be considered and evaluated by nursing professionals. Another limitation was because it was performed in a hospital, hindering to generalize the results of this study.
REFERENCES
1.Siegel RL, Miller KD, Jemal A. Cancer statistics, 2015. CA Cancer J Clin.2015;65(1):5-29.
2.Fitzmaurice C, Allen C, Barber RM, Barregard L, Bhutta ZA, Brenner H, et al. Global, regional, and national cancer incidence, mortality, years of life lost, years lived with disability, and disability-adjusted life-years for 32 cancer groups, 1990 to 2015: a systematic analysis for the global burden of disease study. JAMA Oncol.2017;3(4):524-48.
3.Ministério da Saúde(Br). Instituto Nacional do Câncer José de AlencarGomes da Silva (INCA). Estimativas 2016: incidência de câncer no Brasil [serial on the Internet]. Rio de Janeiro: INCA; 2016 [cited on July 28, 2016]. Available on: http://www.inca.gov.br/estimativa/2016/estimativa-2016-v11.pdf
4.Sousa RM, Santo FHE, Santana RF, Lopes MVO. Diagnósticos de enfermagem identificados em pacientes onco-hematólogicos: mapeamento cruzado. Esc Anna Nery.2015;19(1):54-65.
5.Silva JA, Hansel CG, Silva J. Qualidade de vida na perspectiva de idosos com câncer: implicações para enfermagem na atenção básica.Rev enferm UERJ. [serial on the Internet]. 2016 [cited on Nov 25, 2016]; 24(3): e9621. Available on: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/9621/19405
6.Yilmaz AA, Ozdemir L.Development and implementation of the Clinical Decision Support System for patients with cancer and nurses' experiences regarding the system. Int J Nurs Knowl. 2017; 28(1):4-12.
7.Park H. Identifying core NANDA-I Nursing Diagnoses, NIC Interventions, NOC Outcomes, and NNN linkages for heart failure.Int J Nurs Knowl.2014;25(1):30-8.
8.Conselho Federal de Enfermagem(Br). Resolução no 358/2009. Dispõe sobre a Sistematização da Assistência de Enfermagem e a implementação do processo de enfermagem em ambientes, públicos ou privados, em que ocorre o cuidado profissional de enfermagem, e dá outras providências. Brasília (DF):Conselho Federal de Enfermagem; 2009.
9.Herdman TH, Kamitsuru S. Nursing diagnoses: definitions and classification 2015-2017. Oxford (UK): Wiley-Blackwell; 2014.
10.Moorhead S, Johnson M, Maas ML, Swanson E. Classificação dos resultados de enfermagem (NOC). 5ª ed.Rio de Janeiro: Elsevier; 2016.
11.Bulechek GM, Butcher HK, Dochterman JM, Wagner CM. Classificação das intervenções de enfermagem (NIC). 6ª ed. Rio de Janeiro:Elsevier; 2016.
12.Farhadi M, Reisi-Dehkordi N, Kalantari M, Zargham-Boroujeni A. Efficacy of group meaning centered hope therapy of cancer patients and their families on patients' quality of life.Iran J Nurs Midwifery. 2014; 19:290-4.
13.Benito L, Lluch MT, Falcó AM, García M, Puig M. Identifying nursing interventions in a Cancer Screening Program using nursing interventions classification taxonomy.Int J Nurs Knowl. 2017; 28(2):70-5.
14.Silva MEDC, Silva LDC, Dantas Araújo DOR, Duarte IS, Sousa JFM. Assistência de enfermagem ao paciente oncológico no hospital. Rev enferm UFPI. [serial on the Internet] 2013 [cited on Nov 10, 2016]; 2(5):69-75. Available on: http://www.ojs.ufpi.br/index.php/reufpi/article/view/1359/pdf
15.Santos LF, Oliveira LMAC, Montefusco SRA, Barbosa MA. Diagnósticos e intervenções de enfermagem em famílias de crianças hospitalizadas.Rev enferm UERJ. [serial on the Internet]. 2016 [cited on Nov 25, 2016]; 24(4): e8253. Available on: http://www.facenf.uerj.br/v24n4/v24n4a07.pdf
16.Silva MR, Silva DO, Santos EC, Oliveira PP, Sales AS, Rodrigues AB. Diagnósticos, resultados e intervenções de enfermagem para pessoas submetidas a cirurgias ortopédicas e traumatológicas. Rev enferm UFPE online [serial on the Internet]. 2017 [cited on Sep 14, 2017]; 11(Supl.5): 2033-45. Available on: https://periodicos.ufpe.br/revistas/revistaenfermagem/article/viewFile/23357/18977
17.Oliveira Lopes MV, Silva VM, Herdman TH. Causation and validation of nursing diagnoses: a middle range theory.Int J Nurs Knowl.2017;28(1):53-9.