FIGURE 1 – Four-digit chart related to nurses and doctors evocations to the inductor term: “Taking care of people with HIV/AIDS”, Rio de Janeiro, Brazil, 2014. (n = 81 participants, Fmín = 9; AEO = 2,9; Fcalc. = 12).
RESEARCH ARTICLES
Health care for people living with HIV/AIDS: social representations among nurses and doctors
Virginia Paiva Figueiredo NogueiraI; Antonio Marcos Tosoli GomesII; Yndira Yta MachadoIII; Denize Cristina de Oliveira IV
I
Nurse. Master in Nursing from the State University of Rio de Janeiro. Rio de Janeiro, Brazil. E-mail: virginiafigueiredo@yahoo.com.br
II
Nurse. PhD in Nursing from the Federal University of Rio de Janeiro. Professor, Medical-Surgical Nursing Department and Coordinator of the Post-graduate
Program in Nursing of the State University of Rio de Janeiro. Brazil. E-mail: mtosoli@gmail.com
III
Nurse. Master's Degree in Nursing from the State University of Rio de Janeiro. Brazil. E-mail: yndiramachado@gmail.com
IV
Nurse. PhD in Public Health from the University of São Paulo. Professor, Department of Nursing Fundamentals of the Nursing Faculty of the State University
of Rio de Janeiro. Brazil. E-mail: dcouerj@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2015.14466
ABSTRACT
This study aimed to identify nurses' and doctors' social representations of health care for people living with Human Immunodeficiency Virus and Acquired Immunodeficiency Syndrome (HIV/AIDS). This quantitative and qualitative descriptive study was guided by the structural approach to social representations theory. Eighteen health institutions in Rio de Janeiro, specializing in care for people with HIV/AIDS, were the scenarios for this study in 2011 and 2012. The participants were 54 doctors and 27 nurses, who answered the evocation questionnaire, which was subsequently analyzed using EVOC software. Salient results include these professionals' core representations, comprising positive elements, such as user embracement, information, treatment adherence and future. However, doctors and nurses were found to differ in their representations of the study object. It was concluded that professionals have a positive image of such care, signifying it on the basis of scientific knowledge and Ministry of Health recommendations.
Keywords: Social representations; healthcare; HIV; AIDS.
INTRODUCTION
This study presents the results of the dissertation in Health care to the person living with HIV/AIDS: social representations of nurses and doctors and integrates the multicenter study Transformation of health and nursing care in times of AIDS: social representations and memories of nurses and health professionals in Brazil (both in Portuguese).
In the 1980s, when the first case of Acquired Immune Deficiency Syndrome (AIDS) appeared in the United States, scientists, health professionals and the public were unaware of such a disease and of its etiological agent, which caused panic in people, including the professionals who did not know how to treat individuals who contracted the Human Immunodeficiency Virus (HIV), by the fear of contamination. During this period, health officials assumed that infectious diseases had been controlled, due to the technology and medical knowledge of that time, so that awakened behaviors and collective responses related to fear of contagion and of an unknown disease. In Brazil, the epidemic has evolved demonstrating social, economic and cultural contradictions 1.
The social and moral situation that arose with the advent of the AIDS epidemic associated with the effects of the disease, since the medical knowledge at that time was accompanied by social ignorance, favored the emergence of representations that circulated in the media and through conversations. Some qualified AIDS as a result of moral decay or God's punishment, making it a social stigma, causing rejection and generating rebellion or submission in the excluded ones2.
The virus and the syndrome, unknown, constituted the essential elements for the formation of social representations, were transformed into something known, HIV/AIDS, and were possible to be thought out and actionable. Since then, several representations of the syndrome and the people affected by it emerged. These have been modified, influenced by epidemiological changes, social organization and scientific development3.
With the advancement of research, it was discovered the cause of AIDS, tests were developed to detect the virus, there was also the development of prevention mechanisms, professional self-protection and antiretroviral drugs. But it is noteworthy that the feelings of patients during the discovery of their seropositivity to HIV are of pain and suffering, making it quite difficult to attend this client, both for them and for the professional, since this diagnosis is linked to feelings of death, loss, abandonment, prejudice, rejection by others, disruption of relationships and fear of the unknown 4.
In 1996, Brazil enacted Law No. 9,313, of November 13, 1996, which provides for the free distribution of medicines for all people affected by HIV/AIDS, even against the recommendations and warnings of the World Bank 5. The current public policies in the country in relation to the AIDS epidemic are focused on providing quality care for people living with HIV/AIDS. In this regard, the welfare services have been extended and hospitals have been accredited for meeting this population.
Even today, the infection by HIV encompasses approximately 2.1 million new people infected worldwide6. It is important to highlight the importance of disease prevention and health promotion that, with educational activities, tends to generate more awareness of the responsibility for health, especially among young people who were born in times of AIDS, with affordable treatment and a possible coexistence with HIV.
There are difficulties that interfere with the care of people living with HIV, with highlight to the ethical conflicts and fear of contagion by professionals7. So it is important to adopt an interdisciplinary approach among professionals, so that when difficulties arise in driving situations they deem very hard, they feel at ease to refer the patient to another professional, team member, allowing the customer to speak about their feelings, about their doubts and get guidance and information on the subject, as it is mainly in advising that the professional can perform these activities and all opportunities to clarify doubts of people living with HIV/AIDS (PLWHA) and their families are actions of utmost importance4.
Thus, the health care is a relationship established between individuals in view of the achievement of improving the health and quality of life. Therefore, care practices performed by professionals cannot be restricted to the technique, but should express themselves through attitudes and relationships with others who provide care8.
It is believed that the investigation of social representations of care for nurses and doctors who work with this clientele can help us to understand how care is seen and done as well as it can help in the understanding of the relationships between professionals and PLWHA.
Thus, this study questions: what are the social representations of health care for nurses and doctors? It is proposed as an object of study to know how these professionals represent health care to people living with HIV/AIDS. We aimed to identify the social representations of doctors and nurses about health care to that client.
THEORETICAL-METHODOLOGICAL FRAMEWORK
The Theory of Social Representations (TSR) in its structural approach gives emphasis to the structure of the cognitive content of representations, but also deals with the process of transformation from social practices9. Social representations are a form of knowledge developed and shared by society with a practical view for building a common reality for a social group 2.
The structural approach organizes social representation in two systems: the core, consisting of one or some cognitive elements linked to the collective memory and history of the group that formed the representation. It is presented as consensual, consistent, stable, resistant to change and little sensitive to the immediate social context, generating the basic sense of representation and organizing it as a whole. The peripheral system consists of all the other elements of representation and is characterized by integrating the experiences and individual stories, supports the diversity and contradictions of the group; it is able to move more easily in response to changes in the immediate social context; and performs the functions of adaptation of representation to reality, of flexible regulation of its content and of protecting the core system against the possibility of frequent changes10.
This is a descriptive study with quantitative and qualitative approach, guided by the theory of social representations in its structural approach. The study scenario was composed of 18 health facilities, where activities based in the determinations of the Department of (Sexually Transmitted Disease) STD, AIDS and Viral Hepatitis of the Ministry of Health are developed. These facilities were selected randomly so that they covered all program areas of the city of Rio de Janeiro. Among the services in which study participants have worked, we highlight: Anonymous Testing Center, Reference Center for HIV/AIDS, specialized clinics and services that have been grouped as others (immunology ambulatory, ward of infectious and parasitic diseases, day hospital, medical clinic procedure room and tuberculosis clinics).
Participants were 27 nurses and 54 doctors, totaling 81 professionals who answered the socio-professional questionnaire and free evocations to the inductor term Taking care of people with HIV/AIDS. In the collection of evocations, we asked professionals to speak the first five words that came to mind when they heard the term inducer.
The socio-professional questionnaire data were organized with the help of SPSS software and analyzed using descriptive statistics. For the analysis of evocations we used the four-digit chart by EVOC 2005 software in order to identify the structure of representational content.
The participation in the research was voluntary, from the acceptance of health professionals after knowing the research objectives. The meetings were held in workplaces and data collection took place in the city of Rio de Janeiro, from August 2011 to July 2012. The standards and implementation guidelines of research involving human beings were respected, according to Resolution 196/96, standing during the period of the study planning. The project was presented to the Ethics Committee of the State University of Rio de Janeiro, being approved under the protocol number 048.3.2010; we also used an Informed Consent Form, signed by the participants.
RESULTS AND DISCUSSION
The participants were mostly female (68%), with ages ranging in the age groups up to 35 years (32.10%) and from 46 to 55 years old (34.57%), lived with a partner (50.61%), professed the Catholic religion (49.38%), had a specialization (62.96%), worked at a specialized HIV/AIDS clinics (67.96%), reported updating themselves through periodicals, books, training and conferences (49.7%) and had been working with STD/AIDS from one to five years (30.8%).
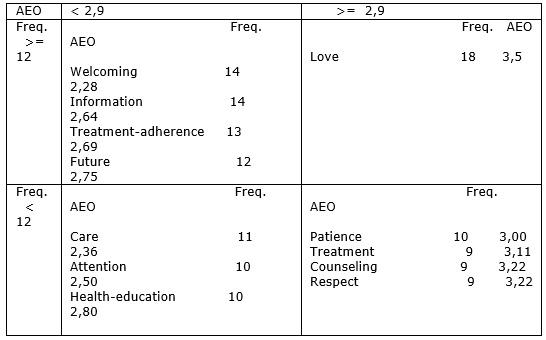
As a result, we obtained 377 words mentioned, among which 113 were different. Considering the dictionary of words that were raised by the participants, the EVOC software calculates the simple frequency of occurrence of each word evoked, weighted average of the occurrence and mean orders. From this information, it was defined as cutoff the minimum frequency of 9, having the mean frequency calculated- 12 and the average evocation order (AEO) - 2.90, which corresponds to the average position of each word in the analyzed corpus. This criterion was used according to the Zipf's law of distribution of words11.
The results of the evocations analysis or prototypical of the set of professionals of the studied city are shown in Figure 1.
FIGURE 1 – Four-digit chart related to nurses and doctors evocations to the inductor term: “Taking care of people with HIV/AIDS”, Rio de Janeiro, Brazil, 2014. (n = 81 participants, Fmín = 9; AEO = 2,9; Fcalc. = 12).
The data presented allow pointing out as the possible core constituents the words welcoming, information, treatment-adherence and future, which reflect the structure of the care process within the determinations of the Department of STD, AIDS and Viral Hepatitis, regarding its retranslation in care practice. Some issues related to this core are also noteworthy: the social representation is organized around the temporal process of care, that starts in the welcoming and aims to increase survival, especially nowadays, when AIDS exists as a chronic condition, permeating the transfer of information, the treatment adherence process; and the representation appears tensioned between the recommendations of the Ministry of Health, as we have pointed out, and the characteristics of each professional, such as zealousness in welcoming, the scientific basis and effectiveness in face of the health-disease process. See Figure 1.
In the lower left quadrant, corresponding to the contrast area, we identified care, attention and health-education, terms that reinforce the core and present same as unfolding of it, highlighting the term care, which is revealed as an imagery dimension of the representation. In the upper right quadrant, first periphery, there is the term love, indicating the dimension of affection, expressing attitude of care and concern for the other, which is a characteristic of professions that work in health care.
In the lower right quadrant, the second periphery, the words patience, treatment, counseling and respect were identified, revealing the practice dimension of care through which PLWHA can have a better quality of life.
We identified elements as likely components of the central system of representation, which are related to the actions and official recommendations from the Ministry of Health and to the essential characteristics of the medical and nursing professions, all positive elements. The results also show a representation of care related to professional ethics, commitment to life and health promotion. It is also emphasized the importance of conducting studies to reduce the regulatory pressure for better understanding of the object itself.
Seeking a better understanding of the studied group, comparative analysis was conducted among professionals who integrated the study, and then we performed an EVOC analysis separately of free evocations of doctors and nurses. According to the evocations of doctors (n = 54), the EVOC 2005 software identified a total of 246 words mentioned, of which 92 were different. The minimum frequency was 6, the average frequency was 9 and AEO reached 2.80. As for the evocation of the nurses (n = 27), the software has identified a total of 131 words, of which 63 were different. The minimum frequency was 4, the average of 6 and OME reached 2.90. From the four-digit chart relating to invocations of nurses and doctors, it was built Figure 2, that illustrates the set of words firstly and more often mentioned in the central core separated by professional category, followed by the contrast area, first and second peripheries.
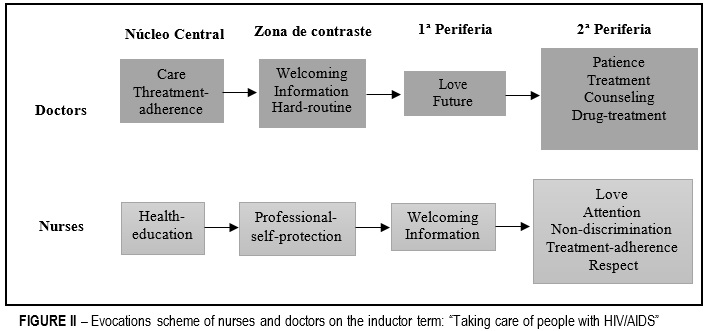
According to the evocations referred by medical professional category, the core was composed of: care, that brings the imagery dimension of representation, as if there were a mirror of the object itself, and treatment-adherence, that brings its practical dimension. It can be inferred that these evoked words are concerning to the professional work in carrying out their activities in which the welcoming is part of the humanization policy of the Brazilian Health System. For these professionals, it is evident that adherence to drug therapy is required to be successful in health care.
However, in the core of nurses' category, the most readily and most frequently word evoked was health-education, as shown in Figure 2. It is evident that, for nurses who make up this study, it is not possible to take care without educating; through the exchange of knowledge PLWHA can be helped to cope with the syndrome and the barriers that it can cause. In health education, the professional transmits knowledge to the customer so that he/she can learn more about their health condition, has the curiosity to know more about HIV infection, how to protect themselves and to take care of themselves, adapting to treatment with the aim of achieve better quality of life. However, terms such as nursing consultation have not emerged, which is an action privative to the nurse and that constitutes a mainstay of care action provided by this professional.
The contrasting elements zone, in the lower left quadrant, brings the words quoted by a few subjects, but that are valued as important by them 12,13. In the contrast zone of the words evoked by doctors the following terms were mentioned: hard-routine and information. As for the nurses, in the contrast zone we have the term professional-self-protection.
The word welcoming indicates an affective dimension; it is involved with the receptivity and listening to the person who receives the care actions 14,15. The terms hard-routine and information are related to the day to day of the professional who deals with the daily difficulties such as poor infrastructure to meet users properly, difficulty to order tests and to reveal the diagnosis to the customer, as well as to conduct drug treatment, stimulating the acceptance of the diagnosis and of the treatment by the customer, who needs information to learn more about AIDS.
The term hard-routine can demonstrate a negative imagery dimension of care representation. The term information can be related to the term health-education, evoked in the central core by nurses, but in a different way. The word reporting deals with organizing data, information and transmitting them to someone else; this differs from educating, when we dialogue with each other, with exchange of knowledge. The term reporting can be related, in doctors' opinion, to the practical dimension of their work to inform about diagnosis, drug prescription, laboratory tests and the health system.
The term professional-self-protection also relates to the daily work of nurses that in their practice, perform invasive procedures and maintain close contact to the client living with HIV/AIDS, which can lead to a greater representation of the possibility of contamination during work if they do not use the personal protective equipment at work at risk due to the risk of contamination in case of accidents where there is contact with contaminated blood and secretion. Currently, due to the large number of clients living with HIV/AIDS chronically, the term professional-self-protection can be anchored in the social memory of AIDS, which was initially linked to fear and death16, among other representations, or even to the emphasis on biosafety brought from the AIDS epidemic17.
The peripheral zone comprises words that were raised later and with greater or lesser frequency, expressing the representational elements that can be associated with life context and social practices, and therefore are unstable, allowing the inter-individual variability of the representation14 .
The first periphery, for doctors, was composed by the words love and future. The term love is related to the affective dimension of representation. The term future can demonstrate an imagery dimension of representation, evidencing that today PLWHA can think about the future by adhering to treatment and that one must have patience to endure all the effects of drug therapy and those that the infection itself causes to the body.
In the first periphery, for nurses, the terms welcoming and information emerged. The term welcoming appeared more readily and is related to the practice of care for PLWHA, where the welcoming is an essential tool in caring for this client and for all those undergoing HIV testing. The welcoming is a technical-assistance action to meet those seeking health services, so that they are welcomed and listened about their needs, implying a service provided with resolution15. The central core, health-education, is reinforced by the attitude related to the terms information and non-discrimination, located on the 1st and 2nd peripheries, respectively.
In the second periphery, that corresponds to the lower right quadrant, are the less frequent and less important terms for the representation; they are subject to more frequent changes in the function to protect the core and maintain the representation.
The second periphery of the medical evocation consists of the terms counseling, patience, treatment and drug-treatment that reinforce the importance of therapeutic actions for the customer's treatment adherence. Counseling emphasizes the need for this adherence to drug treatment according to the progression of HIV in the body. These terms also receive a strong influence of the practical dimension of professionals, through pharmacological treatment and guidelines of the National Policy to combat STD/AIDS. For nurses, the second periphery consists of treatment-adherence, love, attention, non-discrimination and respect, reinforcing the importance of treatment adherence and respect for the person living with HIV/AIDS; such respect is related to the act of caring.
With respect to the characterization of the probable central system of the representation under study for both professional categories, it can be said that it has essentially functional activation by the proximity of the subjects with the object investigated engaged, in which the most important elements for carrying out certain task are privileged in the representation and will constitute the core center, in this case, the care in health to people living with HIV/AIDS12, 13.
According to the likely central core for doctors and nurses, we can extract that doctors represent that care should be carried out by hosting the customer and their needs, and that treatment adherence is necessary for this health care to be actualized. For nurses, the core of their representation on the care shows that care is directly linked to health education, and that the starting point for any health action is counseling, clarification and information on HIV/AIDS and all which encompasses this issue, such as prevention and treatment, through communication and interpersonal skills. These representations can be linked to the professional training; the doctor with training in which care has curative characteristics and the nurse who is trained to care through education, listening and prevention.
Thus, we can tell, through the evocations of the professionals who participated in this study, that the central core of the representation of health care to PLWHA for doctors is guided in drug prescription based on the axes of the Ministry of Health, experienced in working routine and with the focus on drug treatment, i.e., one of medicine bases in order to maintain or achieve health. As for the nurses, the central core of the representation of care to people with HIV/AIDS is guided in health education, i.e., in the relationship and communication with the other, which is a nurse's own role, through concern for professional self-protection, attitudes and care actions. The central core of social representations of care for both professional categories is based on the knowledge reified for vocational training.
CONCLUSION
Through this study, we identified positive elements as probable components of the central core of social representations of nurses and doctors about the care to people living with HIV/AIDS. Terms such as welcoming, treatment-adherence, future and information are related to the actions and recommendations of Ministry of Health, and to the essential characteristics of the medical and nursing professions.
It was observed that nurses and doctors have different contents in the central core about representations of health care to people living with HIV/AIDS. The evocations of doctors reveal the health care based on treatment adherence as the main axis of their action. On the other hand, nurses expressed as the core of health care the term health-education, and the educational activities are bases for nursing care in the studied group. Private actions of the nurse, as the nursing consultation, were not mentioned.
The representations that emerged in this study may be anchored on the basis of the formation of professionals with scientific knowledge. However, it is not possible to say that the representations of doctors and nurses about health care to PLWHA are distinct, because other centrality confirmatory techniques are necessary to establish the existence of different representations.
It is also emphasized the importance of conducting studies to reduce the regulatory pressure for better understanding of the studied object.
REFERENCES
1.Villarinho MV, Padilha MI, Berardinelli LMM, Borenstein MS, Meirelles BHS, Andrade SR. Public health policies facing the epidemic of AIDS and the assistance for people with the disease. Rev Bras Enferm. [online]. 2013 [cited on: 20 nov 2014]; 66: 271-7. Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-71672013000200018&lng=en.
2.Jodelet D. Representações sociais: um domínio em expansão. In: Jodelet D, organizadora. As representações sociais. Rio de Janeiro: EdUerj; 2001: 17-44.
3.Formozo GA, Oliveira DC. Social representations of the care provided to HIV seropositive patients. Rev Bras Enferm, 2010; 63: 230-7.
4.Luz PM, Miranda KCL. The philosophical and historical bases of the care and the call of sexual partners in HIV/AIDS as a form to look after. Ciênc saúde coletiva. 2010; 15 (Supl. 1): 1143-8.
5.Ministério da Saúde (Br). Lei nº 9.313, de 13 de novembro de 1996. Dispões sobre a distribuição gratuita de medicamentos aos portadores do HIV e doentes de AIDS [legislação na internet]. Diário Oficial da União. Brasília, 1996 [citado em 10 jul 2014]. Available from: http://www6.senado.gov.br/legislacao/ListaTextoIntegral.action?id=122864.
6.United Nations Program on HIV/AIDS. The gap report. Joint United Nations Programme on HIV/AIDS (UNAIDS). Genebra (Swi): UNAIDS; 2014. [citado em 2014 Nov 20] Disposable in: http://www.unAIDS.org/en/media/unAIDS/contentassets/documents/unAIDSpublication/2014/UNAIDS_Gap_report_en.pdf.
7.Sadala MLA, Marques SA. Twenty years of care for persons living with HIV/AIDS in Brazil: the health professionals' perspective. Cad Saúde Pública [online], 2006; 22: 2369-78. [cited 20 nov 2014] Available from: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0102-311X2006001100011&lng=en&nrm=iso.
8.Formozo GA, Oliveira DC, Costa TL, Gomes AMT. Interpersonal relations in health care: an approach to the problem. Rev enferm UERJ. 2012; 20: 124-7. [cited 20 nov 2014] Available from: http://www.facenf.uerj.br/v20n1/v20n1a21.pdf.
9.Sá CP. A Construção do objeto de pesquisa em representações sociais. Rio de Janeiro: Eduerj; 1998.
10.Sá CP. As representações sociais na história recente e na atualidade da psicologia social. In: Jacó-Vilela AM, Ferreira AAL e Portugal FT, organizadores. História da psicologia: rumos e percursos. Rio de Janeiro: Nau Ed.; 2007. p. 587-606.
11.Oliveira DC, Marques SC, Gomes AMT, Teixeira MCTV. Análise das evocações livres: uma técnica de análise estrutural das representações sociais. In: Paredes AS. Perspectivas teórico-metodológicas em representações sociais. João Pessoa (PB): Editora Universitária UFPB; 2005: 573-603.
12.Abric J-C. A abordagem estrutural das representações sociais: desenvolvimentos recentes. Em P. H. F. Campos & M. C. S. Loureiro. Representações sociais e práticas educativas. Goiânia (GO): Ed. UCG; 2003: 37-57.
13.Costa TL, Oliveira DC, Formozo GA, Gomes AMT. Structural analysis of social representations of antiretroviral therapy among people living with HIV/AIDS: possibilities of coexistence, normativity and ressignification. Psicologia e Saber Social, 2013; 2: 104-14.
14.Oliveira DC, Gomes AMT, Marques SC. Análise estatística de dados textuais na pesquisa das representações sociais: alguns princípios e uma aplicação ao campo da saúde. In: Menin MSS, Shimizu AM, organizadores. Experiência e representação social: questões teóricas e metodológicas. São Paulo: Casa do Psicólogo; 2005: p. 157-200.
15.Falk MLR, Falk JW, Oliveira FA, Motta MS. Welcoming as a humanization directive: perceptions from users and health professionals. Rev APS, 2010; 13: 4-9. [cited 20 nov 2014] Available from: http://aps.ufjf.emnuvens.com.br/aps/article/view/350/291.
16.Oliveira DC. Construction and transformation of social representations of Aids and implications for health care. Rev Latino-Am Enfermagem [online]. 2013 [cited 20 out 2014];21(esp):[10]. Available from: http://www.scielo.br/pdf/rlae/v21nspe/pt_34.pdf.
17.Gir E, Prado MA, Canini SRMS, Hayashida M. The impact of AIDS in nursing practice: a public health problem. DST Jornal brasileiro de doenças sexualmente transmissíveis. 2005; 17: 39-43. [cited 20 nov 2014] Available from: http://www.dst.uff.br/revista17-1-2005/oimpactodaaids.pdf.