FIGURE 1: Table of four houses referring to evocations of health professionals to the term HIV/AIDS inducer. Rio de Janeiro and Niterói - RJ, Brazil, 2014 (n=214 subjects, minf = 11; Rang average = 3.0; AverageF = 26)
ORIGINAL RESEARCH
Health personnel's social representations of HIV/AIDS: a structural analysis
Yndira Yta MachadoI; Denize Cristina de OliveiraII; Virginia Paiva Figueiredo NogueiraIII; Antonio Marcos Gomes TosoliIV
I
Nurse. Master´s by the Graduate Program in Nursing of the State University
of Rio de Janeiro. Brazil. E-mail: yndiramachado@gmail.com
II
Nurse. Ph.D. in Nursing. Professor of the Graduate Program in Nursing of
the State University of Rio de Janeiro. Brazil. E-mail: dcouerj@gmail.com
III
Nurse. Master´s by the Graduate Program in Nursing of the State University
of Rio de Janeiro. Brazil. E-mail:
virginiafigueiredo@yahoo.com.br
IV
Nurse. Ph.D. in Nursing. Professor, Graduate Program in Nursing of the
State University of Rio de Janeiro. Brazil. E-mail: mtosoli@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2016.14463
ABSTRACT
Objective: to examine the structure of social representation of HIV/AIDS to health personnel. Method: a quali-quantitative, descriptive study was conducted with 214 health personnel from Rio de Janeiro and Niteroi Data were collected using two questionnaires, one socio-professional and the other, free evocation, and were analyzed using the SPSS and EVOC software. Results: the central core of the health personnel's social representations of HIV/AIDS was found to include the terms prejudice, fear, prevention and care. The terms prejudice and fear suggest that adverse meanings present in these personnel's memories are maintained. On the other hand, the terms care and prevention characterize the value that health personnel attribute to preventive practices required to combat the disease. Conclusion: the techniques applied here contributed to a better understanding of the content and structure of the representations in question, but more studies are needed of the role of social norms in this process.
Keywords: Social representations; free evocations; HIV/AIDS; health professionals.
INTRODUCTION
The Acquired Immune Deficiency Syndrome (AIDS) was recognized in the mid-1981 in the United States of America (USA) from the identification of a large number of adult male patients, homosexuals, and San Francisco residents with similar signs and symptoms1. In Brazil, the syndrome was characterized from the beginning of the 80s, as a health sector problem causing most of the public policies emanating from this sector, and even executes programmatic actions to prevent and control the epidemic2.
Currently, the epidemic of the human immunodeficiency virus (HIV) and AIDS is characterized as a mosaic of regional sub-epidemics3,4. Thus, given the profound inequalities of Brazilian society, the spread of HIV infection shows a multi-dimensional epidemic that has undergone significant epidemiological changes over the years4.
AIDS appears as the first disease entity in which the biomedical, symbolic and social constructions happened together. This configuration, delimited three outstanding phases in the context of the epidemic, as stated by Jonathan Mann in 1987: the epidemic of HIV infection - a silent and imperceptible spread of the virus; the AIDS epidemic - manifested by the appearance of symptoms of infectious disease; and the epidemic of social, cultural, the economic and political responses to AIDS, characterized by charged reactions of stigma, discrimination and sometimes denial and disgust of the community5.
In the Social Representation Theory (SRT), the relationship between the construction, the socio-historical process of transformation of representations, social group and social practices in the every day of the same group, in the face of the objects represented the epidemic presents a different configuration6.
The political and epidemiological contexts allow circumscribing four historical moments experienced by people living with HIV/AIDS (PLWHA), as regards the formation of representations, access to care and quality of life, considering their approach to the HIV/AIDS phenomenon. An initial characterized by the beginning of the epidemic, in the 80s; a second time after the regulation of the Universal Antiretroviral Act, from 1996; a third time with a significant mortality fall and resurgence of hope for the future, 2000; and a fourth time - in recent years - with the chronicity of AIDS, in which the representations have been given the notion of death as peripheral, forming new ways of thinking pathology and bringing quality of life to the scene of the immediate concerns5, 6.
Faced with the reported observations, the objective of this study was to analyze the structure of social representation of HIV/AIDS for health professionals working in outpatient clinics in the cities of Rio de Janeiro and Niterói.
In this sense, it was aimed to analyze the structure of social representation of HIV/AIDS for health professionals working in outpatient clinics in the cities of Rio de Janeiro and Niteroi.
THEORETICAL METHODOLOGICAL REFERENCE
Social representations are defined as a set of concepts, propositions and explanations that are built in everyday life, and as a vehicle of its constitution of interpersonal communications7. The theory proposed by Moscovici is considered a great theory, for which emerged complementary approaches and among them, the Central Nucleus Theory, to make it more heuristics to the social practice and research8.
The main idea of the Central Nucleus Theory is that the organization of a social representation presents around a central core consisting of one or more elements that give meaning to representation. The core is determined by the type and nature of the object represented by the types of relationships that the group has with this object and the system of values and social norms that constitute the ideological environment of the group 9.
This is an exploratory, descriptive study with the qualitative and quantitative approach, based on the SRT, which can be defined as socially produced knowledge and shared with a practical purpose and contributes to the construction of a reality common to a social group. It may also be designated as common sense to know10.
The study was developed in care outpatient clinics in HIV/AIDS in the cities of Rio de Janeiro and Niterói, conducted with 214 health professionals who work directly in care for PLWHA. For data collection, a questionnaire about participants characteristics was applied and other containing the collection of free evocations, being held in 2012.
The application of free evocation technique in social studies allows groups to study the social stereotypes that are shared spontaneously by members of the group, and to view the structural dimensions of the particular semantic universe of social representations11.
To perform the collection of free evocations, we ask professionals who agreed to participate in the study to produce five words or phrases with the inductor topic HIV/AIDS.
Data analysis was carried out through two SPSS and EVOC 2005 software. Thus, in the analysis of the data of personal identification and socio-professional instrument SPSS software was used, a statistical software with the function of assisting researchers in handling, analysis and presentation of data analysis results12. For the analysis of free evocations, the EVOC 2005 software was used, which allows the seizure of the organization of the social representation of content and its structure.
The standards and guidelines have been respected to perform studies involving human beings. At the time of data collection, the current resolution was 196 of October 10, 1996, of the National Health Council (CNS). The project was presented to the Ethics Committee of the State University of Rio de Janeiro, was approved with protocol number 048.3.2010.
RESULTS AND DISCUSSION
Analysis of the distribution of study participants by gender, shows a female concentration of individuals of 172 (80.4%) of the total respondents quantitative while 42 (19.6%) are male. The age of the study group was 46 to 55, representing 92 (43%), followed by the age group up to 35 years old with 45 (21%) and professionals aged over 56 years old with 39 (18.2%). Finally, there were the respondents aged between 36 and 45 years old with a total of 38 (17.8%).
The higher the level of training, it is observed that the largest quantity of professional expertise with 103 (48.1%); followed by professionals with master's/doctorate with 41 (19.2%); 36 (16.8%) have only high school, and the lowest percentage was only graduates, totaling 33 (15.4%).
The distribution of participants according to the acting sector were 26 (12.1%) professionals develop their activities in Center Counseling and Testing, 29 (13.6%) in Specialized Care Service, followed by 15 (7 %) active in reference centers and 126 (58.9%) work in specialized clinics.
Analysis of the social representation of health professionals structures about HIV/AIDS
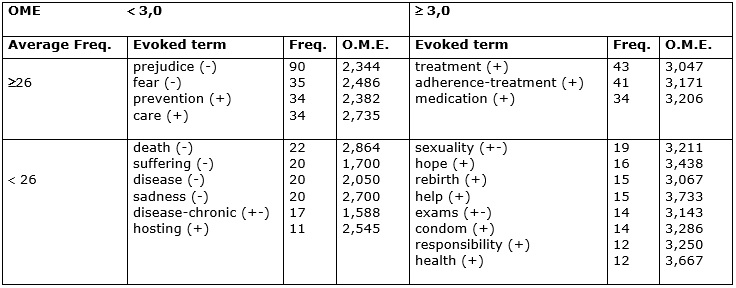
The product of free evocations were 1056 words, and of them, 201 are different. The cutoff points set for this analysis are: minimum frequency (11), medium frequency (26) and average evocation rang (3.0) corresponding to the average position of each word in the corpus analyzed, as shown in Figure 1, which presents the prototypical analysis of the results of all professionals of both municipalities.
FIGURE 1:
Table of four houses referring to evocations of health professionals to the
term HIV/AIDS inducer. Rio de Janeiro and Niterói - RJ, Brazil, 2014 (n=214
subjects, minf = 11; Rang average = 3.0; AverageF = 26)
The presented data allow the possible key elements, which constitute the core of the representation of HIV/AIDS to health professionals: prejudice, fear, prevention, and care.
The prejudice word stands out for having the highest frequency, leaving the other three in quantitative balance and quite far from the first. In the order of evocation, the words prejudice, then prevention and fear are prioritized by professional and have the lowest average orders evocations (OME). The word care has the lowest frequency and the highest average order of evocation, allowing questioning its central position.
Fear and prejudice evocations have normative characteristics, linked to the study group's value system, which allows the core exercise dual evaluative and pragmatic role13. As for the care and prevention, evocations indicate a functional dimension, thus presenting a functional character.
The functional character focuses on the representation and the constitution of the core most important elements for the realization and justification of a task, that is, elements linked to an action, which in the case of this study refers to fighting the disease through the technologies available to combating HIV/AIDS13.
The prejudice word had the highest frequency of evocation and was the most readily evoked, and it can be characterized as the most important element of the analysis. This term is characterized by the intersection of the memory of the study group on the epidemic of HIV/AIDS, including opinions formed before the formation of scientific knowledge about the virus and the syndrome, emotionally conditioned behavior based on beliefs and generalizations, determining dislike and stigmatization of individuals or groups who have HIV/AIDS.
In the case of a disease like AIDS, studies indicate that the general ignorance about the ways of transmission can intensify prejudice and unfavorable attitudes toward those who were infected with HIV, as occurred with other diseases14. The word prejudice corresponds to what Mann was named in 1987 as the third epidemic; that is the epidemic of meanings, effective as or more deleterious and synergistic to the epidemic of HIV/AIDS, as stigmatization and discrimination 15.
The second most common element is the fear, that associated with the word prejudice is the normative character of representation. The fear generated by HIV/AIDS and incorporated the social representation emerges as a negative feeling capable of generating prejudice, and that can reinforce the concepts present in the core, and has a counter-normative character, especially when expressed by health professionals. This group is supposed to support their symbolic constructions in reality elements related to the real risks of contagion and coping possibilities of the disease.
The diseases that cause the most fear are considered not only lethal but also dehumanizing, with the combination of unique physical and behavioral changes. Also, there is the anchoring of the AIDS plague, long used as a metaphor for the worst collective ills, allowing a moralization of the disease, through an atmosphere of its generalization16.
In one study, it was found changes in social representations of AIDS in the health professional group, elements that previously formed the core of representation migrated to the periphery, as the term death. Previously negative central elements became positive after the transition from the concept of fatal disease to chronic disease6.
The prevention and care elements have pragmatic character and therefore it has an association with the practices developed by professionals in the context of HIV/AIDS and suggest a positive attitude towards the object. The word prevention was the second most readily evoked among others present on the likely central core.
The prevention actions within the private life are significant position in the context of AIDS, for example, the intense relationship between prevention and the use of condoms during sexual intercourse
Control actions and fight the disease represent an important advancement in health strategy and articulate prevention and care interventions, as well as surveillance of cases of HIV/AIDS, as provided in the above-mentioned national policy. Therefore, it is understood that it should be more widely used and incorporated in the discourse of professionals and the general population so that they can understand their social roles in the consolidation of policies17.
The term care associated with the prevention features the introduction of positive elements in the representation of HIV/AIDS and is associated with the professional care provided to PLWHA, but also with self-care that the professional should have to avoid contamination.
In this sense, care cognition is characterized by two dimensions related to knowledge and affection, the self-protection measures to HIV in their personal lives and the care provided by health professionals to their customers, just as in cognition prevention.
The health team establishes a relationship permeated the care, both for moral, ethical and social values, as the interference environment. Therefore, the care process influenced by personal training and caregiver's personality acquired through their experiences, beliefs, and culture 18.
The peripheral system of social representation consists of the first and second edge. The first periphery promotes the interface between the concrete reality and the central system and has the characteristic to support the diversity and the group of contradictions13.
The elements of the first periphery are treatment, adherence treatment and drug presenting a conceptual and pragmatic dimension of health professionals about the drug fighting technologies to HIV/AIDS. These terms are elements related to the advancement of antiretroviral therapy (ART).
The most important aspect when it comes to AIDS treatment in Brazil, according to participants, is the availability of medicines in public health and professional initiatives that promote adherence to treatment.
The institution of antiretroviral therapy aims to reduce morbidity and mortality of PLWHA, improving the quality and life expectancy, not eradicate HIV infection. Since the emergence of the first antiretroviral regimens, we sought to define criteria for initiation of treatment based on risk estimates of opportunistic infections, progression to AIDS and death 19.
The introduction of this therapy led to a significant reduction in the mortality rate as well as an increase in life span, leading to their classification as a disease with characteristics closer to chronicity 20. Thus, the presence of cognition treatment also points to the possibility of a change process in the context of social representations of AIDS, which were at the beginning of the epidemic, strongly linked to the idea of death15,21,22.
In the adherence to antiretroviral treatment, it is now part of the care strategies to PLWHA since 1996 with the introduction of antiretroviral therapy and is the main tool to control the disease and its spread to increase survival and quality of life of those people.
The second periphery of representation ensures, in part, the stability of representation, giving protection for the central corel9, consisted of eight elements which are: sexuality , hope, rebirth, help, testing, condoms, responsibility, and health . These elements express positive attitudinal meanings in an affective dimension and humanistic character directed to a better quality of life for PLWHA. They also suggest a more complex view of the health-disease involving subjectivity and perception of the need for a social network to help those living with the disease.
The terms help, responsibility and health give the experience of the professional in direct contact with PLWHA, as well as their responsibility and action for the health of it, has a conceptual and affective dimension.
The sexuality and condom elements have a dimension imagery related to the experience of sexuality associated with protection as well as the actions developed by the professionals associated with the use of condoms as protection against exposure to HIV.
Hope and revival translate the affective dimension of representation and are related to disease, chronic, this in contrast elements, as well as treatment and adhesion treatment present in the first periphery, since the insertion of ART increased the quality and life expectancy of PLWHA, approaching the representation of hope and away the image of death, featuring AIDS as a disease-chronic.
With the advent of the discovery of antiretroviral drugs and the possibility of controlling the disease and their complications, the feeling of impending death gives the feeling of hope for the future. The possibility of living has generated the expectation of conquering new horizons and the ability for people to reorganize their lives23.
The bottom left quadrant or contrast zone may reveal elements which reinforce the present notions in the central core and first periphery, or reveal the existence of a subgroup maintains a separate representation of the majority. It can also point representational changes going from the center to the periphery6,13.
In this quadrant, there are the terms of death, suffering, disease, sorrow, sickness, and chronic care, which reinforce the counter-normative elements of the central core. This counter-normative characterized by the influence of the memory of the beginning of the epidemic in the present representation. These elements are highlighted by an imagery size of disease, negative character, anchored in memory as still part of the social representations of health professionals related to the death of people with the disease at the beginning of the epidemic.
The significance of imminent death is established at the time of diagnosis, considering it is the moment of confrontation with the border situation between life/health and death/illness. After contact with health professionals and other PLWHA, associated with the absence of symptoms of the disease, death no longer arises as something immediate. However, confirmation of the fragility of life becomes the center of everything; it is not known how to act, and this confrontation with no concrete reality can generate much suffering24.
In research, changes were observed in the social representations of AIDS to health professionals. Elements that previously formed the core of the representation migrated to the periphery, as the term death. Previously negative central elements became positive after the transition from the concept of fatal disease to chronic disease, causing a decrease in the importance of death as a result of the process of transformation of social representations of AIDS by health professionals as human relationships build a complex symbolism able to expand the knowledge associated with the syndrome and professional health practices6.
The HIV/AIDS is now considered a chronic disease in patients with good adherence and continuity of antiretroviral treatment. Although the success of ART is unquestionable, the cure is not possible, and PLWHA should maintain adherence to lifelong, facing the risk of toxic effects of drugs. Moreover, despite the control of infection, there is the chronicity of the virus and the presence of inflammation at high risk of complications often associated with aging. This presents a challenge to many health systems since the epidemic is far from being controlled and is only changing its face25.
Contrasting elements as suffering and sadness are negative affective elements. The suffering commonly occurs in PLWHA and may relate to different experienced emotional distress, such as prejudice, living with the disease or an expression of solidarity. This negative feeling intensifies the irreversibility of the disease condition associated with feelings of fear, death, rejection, anxiety and sadness 26.
The PLWHA still living a double journey of suffering, on one hand the physical suffering caused by a disease that is still deadly, even with advances in medicine with so-called antiretroviral cocktails; on the other hand, there is the social suffering caused by exclusionary gaze on the carrier, on many occasions, can be even more serious and devastating 27. The appearance of undesirable effects associated with prolonged use of antiretroviral determines the presence of negative lexicons as suffering and sadness6.
The host element refers to affective actions of health care and also an action provided for in the National Humanization Policy (HumanizaSUS)28. The host is the time that the patient is received in the service and hospitality that concerns both the opening of public services to demand, as the vocation of any responsibility for the health problems of a locality29.
CONCLUSION
In this study, we identified various contents and dimensions that make up the social representation of HIV/AIDS for professionals who assist the PLWHA in the municipalities of Rio de Janeiro and Niterói. Among these contents, elements fond memory, attitudes, knowledge, feelings and images are a highlight.
The social representation of HIV/AIDS for health professionals was built having as central elements of prejudice and fear felt towards the disease, representing the memory of representation features. Although there have been changes in the profile of the disease, treatment and also of PLWHA in the present, past marks such as stigma and prejudice are still present in the representations of these professionals, aiming for their permanence in current representations.
On the other hand, the representation is structured in a pragmatic dimension of positive practices about coping with the disease, characterized by the words present in the core. These meanings characterize the value attributed by professionals to preventive practices necessary to cope with the disease and virus, as well as reflect the implied care practices.
A limitation of this study points out the difficulty of the researcher at the time of collection of free evocations data was the evocation of the words by health professionals.
Also, further studies should be undertaken to confirm the centrality of the elements of social representation, using other forms of complementary analysis.
It is believed that this research will help to understand how professionals think about HIV/AIDS and provide reflections that enable a professional improvement, to improve care to PLWHA.
REFERENCES
1.Galvão J. AIDS no Brasil: a agenda de construção de uma epidemia. São Paulo: Editora 34; 2000.
2.Farah MFS. Gênero e políticas publicas. Rev. de Estudos Feministas. 2004; 12: 47-71.
3.Castilho EA, Chequer P, Szwarcwald CL. A AIDS no Brasil. In: Rouquayrol MZ & Almeida Filho, N. Epidemiologia e saúde. 5ªed. Rio de Janeiro: MEDSI; 1999.
4 Brito AM, Castilho EA, Szwarcwald CL. AIDS e infecção pelo HIV no Brasil: uma epidemia multifacetada. Rev. Sociedade Brasileira de Medicina Tropical. 2000; 34: 207-17.
5.Oliveira DC. A teoria de representações sociais como grade de leitura da saúde e da doença: a constituição de um campo interdisciplinar. In: Almeida AMO, Santos MFS, Trindade ZA. Teoria das representações sociais 50 Anos. Brasília: Technopolitik; 2011: 585-624.
6.Oliveira DC. Construção e transformação das representações sociais da AIDS e implicações para os cuidados de saúde. Rev. Latino-Am. Enfer. 2013; 21(Spec):[10 screens]: 276-86.
7.Moscovici S. Social Cognition: perspectives on everyday understanding. London: Academic Press; 1978.
8.Sá CP. Núcleo central das representações sociais. 2ª ed. Petrópolis: Vozes; 2002.
9.Abric JC. A abordagem estrutural das representações sociais. In: Moreira ASP & Oliveira DC, organizadores. Estudos Interdisciplinares de Representação Social. 2ª ed. Goiânia: AB editora; 2000: 27-38.
10.Jodelet D. Representações sociais: um domínio em expansão. In: Jodelet D, organizadora. As representações sociais. Rio de Janeiro: EdUerj; 2001: 17-44. 11.Oliveira DC, Marques SC, Gomes AMT, Teixeira MCTV. Análise das evocações livres: uma técnica de análise estrutural das representações sociais. In: Paredes AS. Perspectivas teórico-metodológicas em representações sociais. João Pessoa (PB): Editora Universitária UFPB; 2005: 573-603.
12.Maroco J. Análise Estatística: com o SPSS Stattistics. 5ªed. Lisboa: Pero Pinheiro; 2011.
13.Abric JC. A abordagem estrutural das representações sociais: desenvolvimentos recentes. In: Campos PHF, Loureiro S, organizadores. Representações sociais e práticas educativas. Goiânia: UCG; 2003.
14.Seidl EMF, Ribeiro TRA, Galinkin AL. Opiniões de jovens universitários sobre pessoas com HIV/AIDS: um estudo exploratório sobre preconceito. Psico-USF (Impr.), 2010; 15: 103-12.
15.Oliveira DC, Lorenzini EA, Giami A, Vargens OMC; Acioli SO; Gomes AMT et al. Representações e memória profissional da AIDS de enfermeiras no Brasil: estudo bicêntrico Rio de Janeiro/Florianópolis. Psicol. teor. prat. 2007; 9: 114-118.
16.Sontag S. AIDS e suas metáforas. São Paulo: Companhia das Letras, 2007.
17.Valois BRG. Representações sociais da AIDS por enfermeiras das redes básica e hospitalar. [Dissertação] Rio de Janeiro: Universidade do Estado do Rio de Janeiro, 2012.
18.Mendes PW, Castro ES, Ferreira MA. As vertentes do cuidado de enfermagem: o técnico e o expressivo na assistência hospitalar. Esc. Anna Nery. 2003; 7: 239-46.
19.Ministério da Saúde (Br). Boletim epidemiológico HIV/AIDS. Ano II num.01. até semana epidemiológica 26ª – dezembro de 2013 [Internet]. Brasília; 2013. [cited on 2014 Sep. 22]. Available from: http://www.aids.gov.br
20.Schaurich D, Coelho DF, Motta MGC. A cronicidade no processo saúde-doença: repensando a epidemia da AIDS após os antirretrovirais. Rev. enferm. UERJ. 2006; 14(3): 455-62.
21.Camargo BV. Sexualidade e representações sociais da AIDS. R. Ci. Hum. 2000; 8: 97-110.
22.Ragon CST. Atenção odontológica na soropositividade para HIV: um estudo de representações sociais. IV Jornada internacional de representações sociais. II Conferência Brasileira sobre Representações Sociais. João Pessoa; 2005: 2566-83.
23.Thiengo PCS. A Representação Social do cuidado ao paciente soropositivo ao HIV/AIDS entre profissionais de saúde. [Master degree] Rio de Janeiro: Universidade do Estado do Rio de Janeiro, 2013.
24.Gomes AMT, Silva EMP, Oliveira DC. Representações sociais da AIDS para as pessoas que vivem com HIV e suas interfaces cotidianas. Rev. Latino-Am. Enfermagem. 2011; 19: [08 screens].
25.Palmisano L, Vella S. A brief history of antiretroviral therapy of HIV infection: success and challenges. Ann 1st Super Sanita, 2011; 47: 44-8.
26.Costa TL, Oliveira DC, Formozo GA, Gomes AMT Pessoas com HIV/AIDS nas representações sociais de enfermeiros: análise dos elementos centrais, contranormativos e atitudinais. Rev. Latino-Am. Enfermagem. 2012; 20: 1091-99.
27.Barbará A, Sachetti VAR, Crepaldi M.A. Contribuições das representações sociais ao estudo da AIDS. Interação Psicol. 2005; 9: 331-39.
28.Ministério da Saúde (Br). Acolhimento e Classificação de Risco nos Serviços de Urgência.Série B. Textos Básicos de Saúde. Brasília; 2009.
29.Campos GWS. Considerações sobre a arte e a ciência de mudar: revolução das coisas e reforma das pessoas. O caso da saúde. In: Merhy EE, Campos GWS, Cecílio LCO. Inventando a mudança na saúde. São Paulo: Hucitec;1994.
30.Franco TB, Bueno WS, Merhy EE. O acolhimento e os processos de trabalho em saúde: o caso de Betim, Minas Gerais, Brasil. Cad. Saúde Pública. 1999; 15: 345-53.