ORIGINAL RESEARCH
Access to family health unit from the hypertensive's perspective
Inês Leoneza de SouzaI; Elisabete Pimenta Araújo PazII; Raphael Mendonça GuimarãesIII; Adelson Antonio CastroIV
I
Nurse. Ph.D. in Nursing. Faculty Member in the Nursing Course at the
Universidade Federal do Rio de Janeiro Campus Macaé. Brazil. E-mail: inesleoneza@uol.com.br
II
Nurse. Ph.D. in Nursing. Associate Professor at the Anna Nery Nursing
School, Universidade Federal do Rio de Janeiro. Brazil. E-mail: bete.paz@gmail.com
III
Nurse. Ph.D. in Collective Health. Ph.D scholar at the Escola Politécnica
de Saúde Joaquim Venâncio. Escola Nacional de Saúde Pública. Rio de
Janeiro, Brazil. E-mail:
raphael.guimaraes@fiocruz.br
IV
Physicist. Ph.D. in Medical Sciences. Ph.D. scholar on Technology Transfer,
Unidades de Pesquisas Núcleo de Inovação Tecnológica – Rio de Janeiro.
Brazil. E-mail: adelson@nitrio.org.br
DOI: http://dx.doi.org/10.12957/reuerj.2017.14442
ABSTRACT
Objective: to analyze the degree of orientation offered by primary units in relation to the attribute first contact access from the perspective of hypertensive users. Methods: cross-sectional study using Primary Care Assessment Tool-Brazil. Data were collected with 373 hypertensive patients over 20 years of age, in the city of Macaé, Brazil. Results: the predominance of the following individual characteristics was verified: 49% were between 40 and 59 years old; 74% were female; 38.1% had incomplete elementary education; 59.5% had income of up to 2 minimum wages (about US$548.00). A score of 7.65 was obtained for first contact access, superior to the mean of 6.6 of the standard score, and a score of 2.40 for accessibility. Conclusion: the results indicate a satisfactory use of the units in relation to first contact access and unsatisfactory related to accessibility to services, which shows the need for investments in the reorganization of the process of meeting the demands and priorities of users.
Keywords: Family health; access; primary health care; evaluation of health services.
INTRODUCTION
This article is extracted from the Ph.D. dissertation entitledCare quality in health family strategy in Macaé, RJ, Brazil, developed on the graduate program of the Anna Nery Nursing School at the Universidade Federal do Rio de Janeiro (EEAN/UFRJ).
Access to health services in Brazil has been reported as a major health care – related problem. It has been increasingly regarded from the stand of social justice and equity in meeting the needs of the population1,2, insofar as it facilitates people's access to services and professionals, as well as it is central to ensuring quality in health services as a care source2,3.
Access translates characteristics of action supply and interferes with the relation between individuals' demands and the use of health services, that is, the power to utilize them from social and health demands or access. Access mirrors the degree of adjustment between users' needs and health care resources and it is regarded as a component to supply and health services evaluation4.
Evaluating care quality is not a recent practice. Evaluation in the health area has been enhanced after World War II to best account for the role of the State through public programs5,6. Since 2003 the Health Department in Brazil has institutionalized evaluation within the scope of primary care at the Single Health System as a strategy for qualifying that level of care both in management and in care assistance7,8.
This article aims at analyzing the guidance degree about family health strategy (FHS) at primary units in face of first-time access from the stand of hypertensive users.
LITERATURE REVIEW
In primary health care (PHC) context, quite a few health problem complexities lie in the way of professionals. Permanent evaluation proves to be one the main mechanisms to address action and services planning needs as well as to improve performance. The Primary Care Assessment Tool (PCATool) stands out as one of the most widely accepted instruments to that evaluation, which allows for evaluating core attributes as well as those derived from primary care. It also shows excellent assessment properties with local services performance9,10.
By regarding the PHC as the first instance for population contact and access to health system, as well as by acknowledging its resolution capacity as high as 80 per cent over the most common health problems, the country has progressively invested in the expansion of primary units on the family health strategy as a strategy to reorganize, consolidate, and qualify basic actions supplied to population11.
At those units multiple professional teams play an outstanding role on care actions to those bearing chronic diseases, such as systemic blood hypertension. It involves diagnosis, treatment, reduction of complications on account of high prevalence of risk factors to cardiovascular diseases, and strategies which favor bond, good rapport between users and the teams, longitudinal follow-up, coordination of care to other levels of care, and prevention of complications – which might lead to hospitalization and cardiovascular death and to improvement in life quality12.
Assistance to those bearing systemic hypertension (SH) is not PHC exclusive, but best action opportunities happen on that care level because it is a priority to an adult's health care, requiring longitudinal care, a core attribute at PHC. A few pieces of research on evaluation and assistance comparison were conducted in different parts of the country, on the specific basis of the PCATool methodology. Persistent gaps came out concerning health service evaluation at PHC by its users12-14.
As approached in other research, non-transmissible chronic diseases (NTCD), SH in particular, aggravate population's health substantially and cause irreversible damage to self-reliance, independence, and quality of living15.
Therefore, PHC health professionals, nurses in particular, are relevant to control strategies over SH and users' reception. They favor access to monitoring actions in clinic results, support adhesion practices to treatment as well as efforts to provide the patient with the care required to adequate health control and how to go about it. However, concerning the care supplied at HFS, access-related problems are still outstanding about the users at the units16.
To assess the way hypertensive assisted by family health teams in Macaé, Rio de Janeiro, Brazil evaluate access to those PHC units, we have set out to investigate that assistance reality because treatment of SH can be undergone neither on a single-professional nor on one-way basis. It is also influenced by the way the service network is organized, especially in relation to the first contact access at PHC attribute in that municipality.
METHODOLOGY
Cross-sectional study conducted in Macaé, located in the northern part of the state of Rio de Janeiro, Brazil. The municipality lies over an extension of 1,216 km² and has a population estimated at 217,951 inhabitants in 2017. Concerning the services network, it depends on out-patient units, medical specializations, and reference centers. The primary care network has 31 primary units, nine (09) of which in the backlands and twenty-four (24) family health units in the urban area.
The research was conducted in seven family health units in the urban area. Each of them has one (01) interdisciplinary team registered with the national directory of health establishments (NDHE). Teams are integrated by a medical doctor, a nurse, from four to six community health agents, a nurse technician, a surgeon dentist, a dental hygiene technician, a physiotherapist, and a general service assistant. Office hours at family health units run from 8 a.m. to 5 p.m. from Mondays through Fridays.
Three hundred seventy-three (373) hypertensive users registered with the units took part in the study. Participants were randomly selected out of the roll of hypertensive adults at each unit, on the basis of a simple stratified sample, considering a reliability level of 95%. Inclusion criteria were as follows: age > 20 years with a SH; residing within the area covered up by the team; showing at least one visit to the service in the past twelve months with a record on the report of the primary care information system (PCIS) 2012/ 2013.
This article abode by both the ethical research principles and the recommendations in Resolution no.466/2012 of the National Health Council (NHC) of the Health Department in Brazil, which provides for the research with human beings, on the basis of the dissertation project under no. 480.233/2013.
Participants were assured with both secrecy and anonymity concerning information they should provide. In face of their agreement, the Free and Clarified Consent Term (FCCT) was signed up on an individual basis.
To evaluate the first contact access attribute integrated by utilization and access components, the adult version for the PCATool-Brazil was used as a data collection instrument. In general, the tool has 87 questions and the answers show on a Likert-like scale, with value attribution ranging from 1 to 4 to each answer where 1= absolutely not, 2= not likely, 3= likely, and 4= absolutely and 9 corresponds to I don't know/I don't remember. To obtain the general score for PHC, the value average on the items comprising the attribute and its components was calculated according to the following formula: Score = (C1+C2+C3+C4+C5+C6+C7+C8+C9+C10+C11+C12) /12. The score average takes 6.6 as cut-point. Whenever the score is lower than 6.6, the attribute is classified as low PHC. Whenever scores are higher than 6.6, result is classified as high PHC score.
From December, 2013 to March, 2014 participants were interviewed by undergraduate research students from health work education program (HWE) networks17 as well as by volunteer students trained both for tool use and for interview procedures. Interviews were conducted when users attended the free demand service and lasted twenty-five minutes on average. In the first interview round users answered questions on social demographic variables, such as age, gender, schooling, birthplace, family income, family size; and in the second round the adult version PCATool was used .
Data were organized on a spreadsheet, exported to version 20.0 Statistical package for the social sciences (SPSS) and statistically analyzed. Significance level taken was 5% (p<0,05).
RESULTS AND DISCUSSION
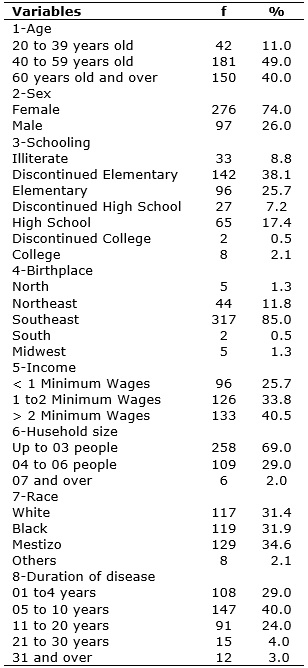
Social demographic characteristics of the 373 participants on the sample show on Table 1.
TABLE 1: Social demographic characterization of hypertensive adults > 20
years old registered with the FHU in Macaé/RJ/Brazil, from December 2013 to
March, 2014. (N=373)
Predominant age in the group ranged from 40 to 59 years old, followed by the elderly. Most interviewees were females, with discontinued elementary schooling (38.1%), evidence to low school levels among the interviewees. The Southeastern region in Brazil stood out for highest birthplace incidence (85%). Concerning monthly income 59.5% of participants showed monthly income of up to two minimum wages. As for self-referred race, there was poorly significant prevalence of those who were self-declared mestizos (34.6%). Concerning diagnosis and follow-up of systemic hypertension 40% of the sample reported 5 to 10 year - follow-up with a health professional.
Guidance from family health units proved to be distant from first contact access to services, especially concerning the attribute first contact access on the access component by the hypertensive registered at the family health strategy units, as shown on Table 2.
TABLE 2: Score average and satisfaction of results on the Access Attribute on
hypertensive evaluation > 20 years old registered at the FHU in Macaé,
Rio de Janeiro, Brazil from December, 2013 to March, 2014 (N=373)

An average of 7.65 was obtained for first contact access on the utilization component, which surpasses the 6.6 average score value. That result was regarded as high conversion score of the PCATool instrument. Variables integrating that attribute were the priority search for the family health unit before any other service, heading for the family health unit whenever there is a health problem, and the need to see a professional on the team if there is suggestion for a specialist's evaluation.
On the other hand, the 2.40 score to first contact access is distant from the average score value, a fact which might confirm users' difficulty to have their demands met at the units. Access variables integrating that attribute included the units' business hours, service provided on the very first day of the visit to unit, phone access to professionals, uncomplicated agenda for scheduling revision visits, and over a thirty minute-wait to schedule the visit sought.
Concerning satisfaction with first contact access, also shown on Table 2, we have observed the inversely proportional relation on the use of services (21.7%) against 99.2% of users unhappy about first contact access on the access component. That discloses strong family health users' difficulties about having their demands met.
When satisfaction and social variables are associated a statistically significant relation was found on the following items: utilization, affiliation to unit, age group and race, according to Table 3.
TABLE 3:
Variables associated to dissatisfaction by the hypertensive registered
with the FHUs Macaé, Rio de Janeiro, Brazil, related to Access, from
December 2013 to March 2014.
(N=373)
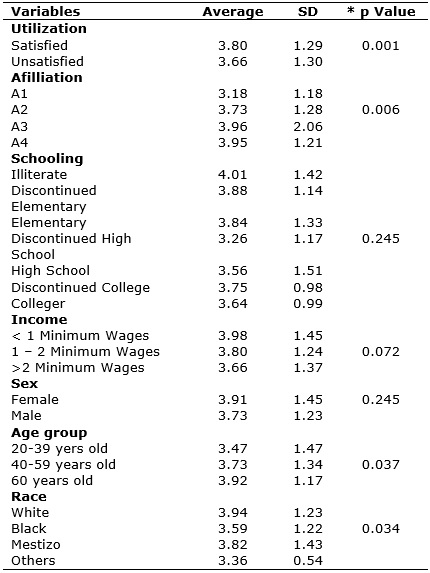
Despite not ensuring a statistically significant result on account of the trust level obtained, there should be larger discussion on the following issues: discontinued average schooling, income ranging from 1 to 2 minimum wages, being a female, being from 40 to 59 years of age, and being black. This way there might be identification of a cause-effect relation with attributes and their components.
As for social demographic data, results showed women were those who mostly sought family health units for services. That nears the result found in both a study on access in a medium sized municipality in Bahia18 , Brazil and a study on food consumption among the hypertensive, conducted in Dourados – MS, Brazil19. Female prevalence in health care service can be accounted for both by higher demand for health care among women who are also more strongly concerned and by the age factor, for the number of women after 50 with hypertension is higher than that of men20.
Results show a difference in responses at first contact access on the utilization component when compared to the access component. Users regard utilization access as satisfactory (78.3%), which can be accounted for on the basis of the small distance between units and users' residences. That distance favors the demand for services whenever they need them; and they regard access as unsatisfactory (99.2%). That is, they identify the unit as providing the service they are after, but they report coming across hindrances concerning both integrality of services provided and professionals at the health units with FHS, such as the long wait to obtain an appointment, starting at an evaluation on the selection model by problem seriousness, with no guiding criteria to that evaluation. Similar results were found in nation-wide studies on the evaluation of family health strategies, which characterized the poor guidance at those units in relation to PHC21,22.
A relevant guiding evaluation aspect to Primary Health Care in Brazil, which has helped adequate and effective implementation of the Single Health System (SHS), lies on the National Program for Access and Quality Improvement in Primary Care (PAQI-PC). With its implantation in the municipalities, difficulties began to be discussed as of 2011. Today, the program goes through its second round, which is regarded as very precocious in face of the complexities, costs, and exhaustive nature23of the nation-wide process, both to the PHC evaluated teams involved and to the evaluators' teams in the health system.
The aspects evaluated as unsatisfactory draw attention to the low capacity of the units studied to meet population's demands and expectations because service supply is still based on the model centered on attention to those problems and symptoms that are urgent to users, with no direction to health promotion actions required to the improvement in performance along hypertension care24.
It is worth highlighting the study conducted with producers at the farmers' market in Feira de Santana – Bahia, Brazil, on their perception of chronic diseases as a way to face that chronic condition. That was a proposition to investing in health education and to understanding SH and its complications to foster healthy habits, respect one's culture and way of living, and reduce suffering (upon adhesion to treatment) and morbid mortality resulting from SH25.
In the statistical analysis of the variables accounting for users' dissatisfaction about family health units, the affiliation component obtained low evaluations by interviewees, showing a 3.68 average, far from the 6.6 average score. During the research, the medical doctor's absence in business hours stood out as well as it did the poorly skilled professional in charge of assistance. It can be said that the interviewees acknowledge the health unit as capable of providing first assistance, but they do not acknowledge professionals as a reference for regular health follow-ups, for they understand that is not ensured on the care model available at the units.
A similar result was found in the study conducted in Passos, Minas Gerais, Brazil, where the FHS showed the highest scores on all attributes, exception made to First Contact Access26. The low score on the first contact access attribute results from high levels of negative evaluations to business-hour related items, with special emphasis on the item related to how professionals at the unit provide night shift services to ill users as well as to how the population communicates with the service.
Access is regarded as the adequacy between supply and demand for health services; a piece of research similar to this study was conducted on Family Health Strategy Evaluation from Health Professionals' stand in Serra, Espírito Santo, Brazil. The access attribute obtained the lowest score value, a result that translates a health service problem since it is by means of first contact access that the professional conducts reception, can strengthen the professional-user-service bond, and can provide guidance about the required care27.
Therefore, despite a score far below the average expected for a PHC service on the affiliation degree in Macaé, Rio de Janeiro, Brazil, the interviewees acknowledge both the health unit and the professional who provided the service on the day he/she went to the unit. That intervention model is still centered on the disease and not on the ill person.
CONCLUSION
This article reports on the guidance degree from an FHU in Macaé, Rio de Janeiro, Brazil, as for users' access to those services upon first level care in the municipal health system, by means of the use of the primary care evaluation instrument PCATool-Brazil.
Data analysis of first contact attribute on the access component evinced high users' dissatisfaction about health services, on the basis of the poor organization of the units as providers of integral end-to-end care to population.
Restriction on the preferential use of FHU as a gateway is regarded as one of the major access hindrances, from the operational model to the assistance type, as it is centered on clinical complaints rather than on family approach.
Results do little to the understanding of PHC dimensions and differ from an effective primary care service, which must show high responsive capacity to prevailing problems among the population within its territory.
On account of their strategic relevance responding to health problems of the population with hypertension, the FHU in Macaé, Rio de Janeiro, Brazil are able to reorganize their work process and become a major locus for the development of professional actions anchored on end-to-end integrality, territorialization, liability, bond, and responsibility principles.
From that perspective, nurses acting at the FHS can help decrease inequity and improve indicators within circumscribed area. The impact generated by a care model limiting universal access impoverishes the bond with both services and professionals, as a result.
The low results found on the evaluation of the core attribute upon first contact access showed the need for relevant adjustments to invert the prevailing logics on work processes in health services at FHC centered on the biomedical model.
Despite the high utilization of those services, investments in professional education prove to be a priority. They can be a qualification and improvement strategy on health care within the municipality. The improvement of both access and operation of the health system by means of ensuring universal, integral, end-to-end, and network-like access turns out to be a continuing challenge.
REFERENCES
1.Lima MADS, Ramos DD, Rosa RB, Nauderer TM, Davis R. Acesso e acolhimento em unidades de saúde na visão dos usuários. Acta paul. enferm. 2007; 20(1):12-17.
2.Sanchez RM, Ciconelli RM. Conceitos de acesso à saúde. Rev. Panam. Salud Pública. 2012; 31(3): 260–8.
3.Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Política Nacional de Atenção Básica. Brasília (DF); EMS;2006.
4.Novaes HMD. Pesquisa em, sobre e para os serviços de saúde: panorama internacional e questões para pesquisa em saúde no Brasil. Cad. Saúde Pública (Online), 2004;20(Supe2):5147-57.
5.Donabedian A. Explorations in quality assessment and monitoring. Ann Arbor, (USA) Health Administration Press; 1980.
6.Hartz ZMA, Organizador. Avaliações em saúde: dos modelos conceituais à prática de análise da implantação de programas. Rio de Janeiro: FIOCRUZ; 1997.
7.Stein AT. Health service evaluation requires the use of validated instruments. Rev. Epidemiol. Serv Saúde. 2013; 22(1):179-81.
8.Ministério da Saúde (Br). Avaliação da atenção básica em saúde: caminhos da institucionalização. Brasília (DF): EMS ; 2005.
9.Ministério da Saúde (Br). Secretaria de atenção em saúde. Manual do instrumento de avaliação da atenção primária à saúde: primary care assessment tool pcatool – Brasil. Brasília (DF): Departamento de Atenção Básica; 2010.
10.Cesar MC, Campos GWS, Montebelo MIL, Sarmento G. Avaliação da atenção primária no município de Piracicaba, São Paulo, Brasil. Rev. Saúde em Debate. 2014; 38 ( esp):296-306.
11.Ministério da Saúde (Br). Secretaria de atenção à saúde. Hipertensão arterial sistêmica para o sistema único de saúde. – Brasília (DF): EMS; 2006.
12.Rabetti AC, Freitas SFT. Avaliação das ações em hipertensão arterial sistêmica na atenção básica. Rev. saúde pública (Online). 2011; 45(2):258-68.
13.Souza MLB. Modelo orgânico de avaliação participativa: construção e aplicação na estratégia saúde da família [tese de doutorado]. Rio de Janeiro: Universidade Federal do Rio de Janeiro; 2011.
14.Lima EFA, Sousa AI, Silva MM, Souza IEO, Leite FMC. Avaliação da atenção primária na percepção dos usuários e profissionais de saúde: uma revisão integrativa. Rev. enferm. UFPE on line. 2014; 8(supl. 2):3758-66.
15.Fava SMCL, Silva PCS, Machado JP, Lima J, Vieira LLV, Veiga EV. Associações entre pressão arterial, circunferências braquial e abdominal de pessoas com hipertensão arterial. Rev. enferm. UERJ, 2016; 24(2):e14500.
16.Araújo JL, Paz EPA, Moreira TMM. Hermenêutica e o cuidado de saúde na hipertensão arterial realizado por enfermeiros na Estratégia Saúde da Família. Esc. Anna Nery Rev. Enferm. 2010; 14(3): 560-66.
17.Ministério da Saúde (Br). Ministério da Educação. Portaria Interministerial nº 421, de 3 de março de 2010. Institui o Programa de Educação pelo Trabalho para a Saúde (PET Saúde) e dá outras providências. Diário Oficial da União, 05 de março de 2010; seção I, pág 52.
18.Souza LF; Chaves SCL. Política Nacional de Saúde Bucal: acessibilidade e utilização de serviços odontológicos especializados em um município de médio porte na Bahia. Rev. baiana de Saúde Pública. 2010; 34(2):371-87.
19.Coca Al, Gripp DB, Schinestzki ECV, Gianlupi K, Liberali R, Coutinho VF. Consumo alimentar e sua influência no controle da hipertensão arterial de adultos e idosos de ambos os sexos em uma unidade básica de saúde em Dourados – MS. RBCEH: 2010;7(2) 244-57.
20.Dourado CS, Macêdo-Costa KN, Oliveira JS, Leadebal OD, Silva GR. Adesão ao tratamento de idosos com hipertensão em uma unidade básica de saúde de João Pessoa, Estado da Paraíba. Acta Scientiarum Health Sciences. 2011; 33(1):9-17.
21.Reis RS, Coimbra LC, Silva AAM, Santos AM, Alves MTSSB, Lamy ZC et al. Acesso e utilização dos serviços na Estratégia Saúde da Família na perspectiva de gestores, profissionais e usuários. Ciênc. saúde coletiva (Online). 2013; 18(11):3321-31.
22.Fausto MCR, Giovanella L, Mendonça MHM, Seidi H e Gagno J. A posição da estratégia saúde da família na rede de atenção à saúde na perspectiva das equipes e usuários participantes do PMAQ-AB. Rev. Saúde em Debate. 2014; 38( esp):13-33.
23.Mota RRA, David HMSL. Programa Nacional de Melhoria do Acesso e da Qualidade da Atenção Básica: questões a problematizar Rev. enferm. UERJ. 2015; 23(1):122-7.
24.Pires MRGM, Gottems LDB, Cupertino TV, Leite LS, Vale RL, Castro MA et al. A utilização dos serviços de atenção básica e de urgência no SUS de Belo Horizonte: problema de saúde, procedimentos e escolha dos serviços. Rev. Saúde Soc. 2013; 22(1):211-22.
25.Silva SRA, Amorim RCA, Almeida AM. Percepção de feirantes hipertensos sobre o adoecer crônico. Rev. enferm. UERJ. 2015; 23(6):761-6.
26.Ferreira VD, Oliveira JM, Maia MAC, Santos JS, Andrade RD, Machado GAB. Avaliação dos atributos da atenção primária à saúde em um município mineiro. Esc. Anna Nery Rev. Enferm. 2016;20(4): e20160104.
27.Lima EFA, Sousa AI, Leite FMC, Lima RCD, Nascimento MH, Primo CC. Avaliação da Estratégia Saúde da Família na perspectiva dos profissionais de saúde. Esc. Anna Nery Rev. Enferm. 2016;20(2):275-80.