ORIGINAL RESEARCH
Stress assement among hospital nurses
Neireana Florencio VieiraI; Denismar Alves NogueiraII; Fábio de Souza TerraIII
I
Nurse. Master, Federal University of Alfenas. Minas Gerais. Brazil. E-mail: nfvieira30@gmail.com
II
Zootechnist. PhD. Professor, Federal University of Alfenas. Minas Gerais
Brazil. E-mail: denisnog@gmail.com
III
Nurse. PhD. Adjunct Professor, Federal University of Alfenas. Minas Gerais
Brazil. E-mail:
fabio.terra@unifal-mg.edu.br
DOI: http://dx.doi.org/10.12957/reuerj.2017.14053
ABSTRACT
Objective: to evaluate the stress among nurses working in public and private hospitals. Method: descriptive, analytical, transversal and quantitative research, with 100 nurses from four hospitals in a city in the south of Minas Gerais, Brazil. For data collection, a questionnaire containing socio-demographic variables and the Bianchi Stress scale were used. The Chi-square test of Person or Fisher's Exact were conducted, determining Cronbach's Alpha and odds ratio for independent variables associated with stress. Research protocol approved by Research Ethics Committee, CAAE: 27795814.7.0000.5142. Results: a mean level of stress was found among nurses, highlighting a high level in three areas of the scale: activities related to unit functioning, personnel administration and coordination of unit activities. Conclusion: stress is present among nurses, especially in functions related to the administrative activities of the unit that express their functioning.
Keywords: Nursing; worker's health; psychological stress; hospitals.
INTRODUCTION
The work of nurses in the hospital environment demands skills, technical competence and emotional control over the practice. This environment presents situations of risk and exposure to a continuous wear, with possible losses of the satisfactory conditions of life1.
Nurses working in hospitals provide assistance to patients and their relatives who experience conflicting aspects such as birth and death. Nursing is portrayed as a stressful profession due to the responsibility towards the lives of people and the close interaction with suffering. It is a profession that requires dedication in the performance of duties and brings a high probability of occurrence of psychological exhaustion 2.
The onset of occupational stress in hospitals may become more evident in the case of high workloads and night shifts that cause extreme fatigue, loss of concentration, decreased professional performance and physical and emotional exhaustion3.
It is noteworthy that nurses carry out many activities related to a high degree of difficulty and accountability which when associated with the fast pace, excessive working hours, and work in shifts can result in occupational stress related to psychosocial factors conditioned to the presence of environmental stressors4.
Based on these considerations, this study is relevant due to the possibility of deepening about the discussion on stress and hospital nurses and offering subsidies for hospital institutions to address the main stressors of the hospital environment in an attempt to minimize the health problems of workers.
The objective of this work was to assess the stress among nurses in public and private hospitals.
LITERATURE REVIEW
Occupational stress is defined as a type of stress associated with excessive tension in professional activities. This concept can be seen from the transactional perspective, where there is an interaction between individuals and stressful situations, where stress is determined by the workers' perceptions of demands in the work environment and by their abilities to cope with them5-7.
Health and performance of hospital nurses can be influenced by the demands of the work combined with insufficient resources to cope with them. These resources refer to the interactions of workers with the environment, and the work content and organizational conditions8.
Nurses who work with people under distressing situations, often experience stress because the problems are not always solved immediately and easily 9.
Several factors can be considered as stressors in nursing work. Among the main factors are the activities of direct patient care, human relations, workload, compliance with norms and protocols, professional autonomy, relationship between degree of requirements and level of skills for the development of activities, high responsibility and processes of institutional organization7,10.
It is observed that nursing workers face a quantitative overload, evidenced by the responsibility to provide care for many patients, and also qualitative overload, in the sense of the complexity of human relationships, for example, in the nurse/client, nurse/professional, nurse/family interactions11.
Organizational, technical and technological innovations associated with the progressive and significant increase of occupational stress have required constant adaptation, greater awareness and great ability to face evolutions and manage stress11. Thus, stress in nurses can have some consequences such as decreased productivity in work activities and appearance of diseases when stress exceeds the limits of the individuals 12.
METHODOLOGY
This is a descriptive, analytical, cross-sectional and quantitative study carried out in four hospitals (public and private) in a city in the south of Minas Gerais.
The hospital institutions analyzed in the study were identified by letters A through D, where the public institution A was composed of 52 nurses; and the private institutions B, C and D had 33, 32 and 13 nurses, respectively.
The study population consists of all 130 nurses working in these hospitals. The following exclusion criteria were adopted: nurses working for less than six months as nurses in the hospital sector; nurses who were on vacation; nurses who were on sick leave or pregnancy/maternity leave. After applying the exclusion criteria, the sample was reduced to 100 nurses, of whom 40 were from hospital A, 23 from hospital B, 25 from hospital C and 12 from hospital D.
Data collection was conducted in May 2014 with aid of a questionnaire covering 24 sociodemographic variables, life habits, academic training and work activity. This instrument was submitted to a refinement process through evaluation of five research judges who work on this theme and was later submitted to a pilot test with hospital nurses from a private hospital in another surrounding municipality.
The Bianchi Stress Scale, created and validated in Brazil in 2009, was also used to assess stress in hospital nurses in the basic performance of their activities13.
The Bianchi Stress Scale is a self-administered instrument containing 51 items in a Likert type scale ranging from 1 to 7 where 1 corresponds to little exhausting; 4 to medium; and 7 to highly exhausting. The value 0 was reserved for cases when nurses did not perform the activity addressed. This scale is divided into six domains: (A) Relationship with other units; (B) Proper functioning of the unit; (C) Personnel administration; (D) Patient care; (E) Coordination of activities of the unit; and (F) Working conditions. All domains related to the activities performed by nurses and/or working conditions13.
The assessment of stress followed the classification: low stress level (equal to or below 3.0); medium stress level (between 3.1 to 5.9); and high stress level (equal to or above 6.0)13.
The researcher approached nurses in their work environment and gave them an envelope containing the two instruments (questionnaire and scale) and two copies of the Informed Consent form. The completion of the instruments was performed by the participants themselves, using the self-filling technique.
After collection of data, these were grouped in a spreadsheet by double typing and tabulated in the Statistical Package for Social Science (SPSS), version 17.0. The Chi-square test of Pearson or Fisher's Exact test were used for bivariate analysis of the independent variables with the measure of stress, adopting a level of significance of 5%. After this step, the odds ratio of the independent variables was used with the stress measure for possible risk associations.
Subsequently, a logistic regression model was used for multiple analysis of the independent variables with stress. The method of selection of variables was Backward Stepwise and the odds ratio was also used, with significance level of 5%. In order to evaluate the internal reliability of the scale, internal consistency was tested using the Cronbach's Alpha coefficient.
The research was grounded on the ethical precepts of Resolution 466/12 of the National Health Council and the project was evaluated by the Research Ethics Committee of the Federal University of Alfenas (Unifal-MG) and approved under Opinion nº 566,949. The research institutions authorized the development of the research and the participants were asked to provide a written agreement through the Informed Consent term, with guarantee of anonymity and of the right to withdraw from the study at any stage.
RESULTS AND DISCUSSION
We found that the nurses surveyed were predominantly female - 86%, in the age group between 30 and 39 years - 49%, married/with partner - 59%, had no children - 54%, had a monthly family income between 3,501 to 7,000 Brazilian reais - 49%, were Catholics - 73%, practiced physical activities - 63%, were non-smokers - 96%, did not consume alcoholic beverages - 58%, had no chronic diseases - 90%, and did not make continuous use of medicines, 67%. Regarding the professional training, the majority had graduated 4 to 6 years ago - 42%, and had postgraduate degrees - 80%. Concerning the variables of professional performance, there was a predominance of nurses with up to 3 years of experience as a hospital nurse - 44%, with a workload of 44 hours per week - 43%, did not have another employment bond - 77%, and performed the functions of direct care and supervision - 46%.
The predominance of the female sex coincides with other investigations that found a highest frequency of women in the nursing profession 14,15. In addition to living with the dynamics of the work organization, these nurses also manage their personal lives. This situation of multiple activities can generate stress because they work outside the family home, but are concerned with domestic care and with children 16.
Similar data to this study, regarding age, marital status, number of children and family income were found in other studies13,17. In this context, it should be noted that younger professionals present lower levels of stress when compared to those older than 40 years, which is associated with natural aging, a condition that decreases tolerance to high workloads18.
Among the participants, most were married and had 1 to 3 children. The condition of being married and having children can be stressful when compared to peers who are not married or have no children. This can be explained by greater responsibility/concern with family issues18 .
With regard to religious belief, all participants had some kind of religion. It is therefore necessary to emphasize that when people turn to religion to deal with stress, religious-spiritual coping takes place, improving people's physical and mental health19.
In relation to the practice of physical exercises, it was noticed that the majority of the participants practiced physical activity. It should be noted that regular physical exercise is positively associated with mental and social health20.
In this study, young nurses reported having no chronic disease. There is a notable association between older age and presence of chronic diseases. This requires considering the increased effects of professional burnout on vulnerability to illness, including stress21.
When analyzing the time working as hospital nurses and the time elapsed after graduation, nurses with less time elapsed after academic training and of performance in the hospital setting had a predominance of medium stress. Novice nurses are considered to experience higher stress levels because recent graduation implies greater the stress at work22. Also, nurses with more time of professional performance had mostly medium stress, meaning that nursing work is stressful.
The high percentage of women in the present study and the most frequent workload of 44 hours per week are outstanding because besides the long working hours of these professionals, they take on housework and responsibilities with children. Moreover they have to deal with human lives, suffering and death23.
In the present study, 23% of the participants had another employment bond and 49% had a monthly income ranging from 3501 to 7000 Brazilian reais. It can be inferred, therefore, that the satisfaction about the income of these workers can be a factor of the option for a single employment bond and, consequently, the absence of association of this variable with stress.
However, wage is a relevant factor in the manifestation of stress. Although some nurses had a high salary, this factor may be associated with the recognition they expect for the work they perform16,24.
There was in the present study a higher frequency of nurses who work in the function of provision of care and supervision. The level of stress in the functions performed by them is directly related to the type of work performed and the level of exposure to their stressors25,26. Therefore, it can be inferred that the role assumed by nurses associated with stress is related to the activities inherent to the position they occupy.
With regard to significant life events, 43% of the nurses listed some, especially the loss/death of a loved person, the birth of a child/grandchild and the diagnosis of an illness in a loved person. In turn, 61% of the nurses reported a significant event in their career in the last year, particularly the gain of further responsibility/function, lack of professional recognition and conflicts with peers.
It is noted that the variable significant event in life had a significant association with stress. There are striking events that permeate the lives of people and require some responses to overcome the moments of instability. Thus, these events are part of the person's individual life cycle and can trigger stress27.
The event accumulation of responsibilities/functions stood out among the significant events in the career. It can be inferred that such work overload is often related to the fact that nurses take on the responsibility of many activities, many of which are out of their competence and expose them to stressful situations28.
The Bianchi Stress Scale showed an internal Cronbach's alpha coefficient value of 0.95 in the general score and all domains of this scale presented values above 0.74. Thus, the internal consistency of the domains and the general consistency can be considered acceptable for the items evaluated and correlated to each other, indicating homogeneity.
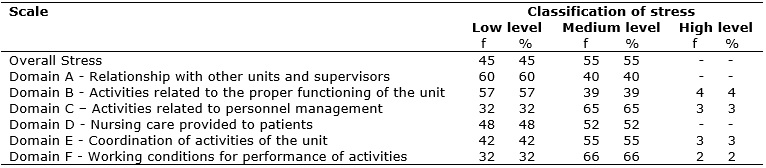
With regard to the classification of stress, 55% of the participants presented medium stress level, followed by 45% with low level. It is important to highlight that there were no participants with high level of stress, according to Table 1.
TABLE 1:
Percentage distribution of hospital nurses according to the general stress
classification and for each domain of the Bianchi Stress Scale.
Poços de Caldas-MG, 2014.
Regarding the stress of hospital nurses, it is noteworthy that some studies on the assessment of this construct in these professionals have also found an medium level of stress among the evaluated participants16,17.
The scale is divided into 6 domains. In the classification of stress in each of the domains, it is notable that of all domains, the B (activities related to the proper functioning of the unit) was the one that presented the highest frequency of nurses with high level of stress. The domains C (activities related to personnel management) and E (coordination of activities of the unit) also presented nurses with high level of stress.
In relation to the medium level of stress, the domains C, D (nursing care provided to patients), E and F (working conditions for performance of activities) had medium stress. However, the domain F stood out with 66 (66%) of the participants. These results are similar to other studies that also showed a medium level of stress in the F and C domains14-30 .
Considering the low stress level, the Domain A (relationship with other units and supervisors) predominated with 60% of the participants, followed by Domain B with 57%. In other surveys, domains A and B were also the ones with the highest number of nurses with low level of stress15,16.
Regarding the most frequent stressors (items), based on the score 7 (highly exhausting) found in each domain of the scale, the most important stressors in Domain A were relationship with maintenance staff (12%) and relationship with the pharmacy (7%).
We can say that interpersonal relationships represent a stressing agent because of the lack of adaptation among people and poor communication. It is up to nurses to mediate and promote communication with other professionals and with hospital sectors, as well as develop behaviors to reduce the pressure over the staff and ensure compliance with the institution's standards28-30.
In Domain B, it was noticed that the most frequent stressors wererequest for revision and repair of equipment and control of equipment, with 17% and 10%, respectively.
Managerial activities linked to care activities stand out because they are fundamental for the proper functioning of the unit. Thus, it is necessary to promote a work environment allied to the strategies of changes such as ergonomic adequacy, physical space, and control of materials and equipment as fundamental in the work organization29.
In Domain C, the stressors that stood out werecontrol of the nursing team (22%) and supervision of team activities (15%). These most frequent stressors found in Domain C were also the items that caused greatest exhaustion among nurses evaluated in other studies14,30.
It is important to reflect that the management of personnel is related to the management of nursing care. Thus, the pressures imposed by the work environment, with demand of higher productivity and complexity of tasks, are some factors that can influence the management of personnel, and they consequently are a cause of stress9.
Regarding Domain D, 20% of the reports of nurses were associated with the stressor facing the death of patients and 15% were associated with assisting relatives of critical patients.
Some studies have also shown that, among the most frequent stressors of the D domain were the items were facing the death of patients and assisting relatives of critical patients13,14.
As the death of patients is constant in hospitals, it is assumed that nurses accept this event as natural; however, it can be said that the human being is not prepared to live and accept loss13.
In Domain E, we observed that the most prominent stressor wascontrolling the quality of care 20%, followed by the stressor coordinating activities of the unit 18%.
Other investigations have also shown these same stressors of Domain E as highly stressful among nurses14,31.
A proper reflection here is when nurses interact with a team that is under their supervision, they are responsible for the care provided and they assume many activities in the practice and broad responsibilities that lead to stress situations21.
And finally, in Domain F, it was possible to observe that 27% of the reports were related to the stressorperforming tasks with minimum available time and 17% with the level of noise in the unit.
In some studies, these stressors were also found in Domain F as the items that caused greatest wear among the evaluated nurses15,31.
We can infer that the short time that nurses have to carry out the activities is associated with some elements known to be threatening to the occupational environment, such as small number of nursing professionals, excess of activities to be performed, the fact of assuming several sectors, and concomitant activities and difficulties in delimiting the different roles of nurses and nursing technicians1.
We identified in this study that none of the analyzed variables showed a significant association with stress. They had the following levels of significance: sex (p = 0.451), age (p = 0.887), marital status (p = 0.526), number of children (p = 0.493), monthly family income (P = 0.237), type of residence (p = 0.787), religious belief (p = 0.603), municipality of residence (p = 0.727) practice of physical exercise (p = 0.053), smoking (p = 1,000), frequency of alcoholic drinking (p = 0.968), chronic diseases (p = 0.505), continuous use of medication (p = 0.358), significant career events (p = 0,313), time elapsed after graduation (p = 0.788), postgraduate degree (p = 0.615), time working as hospital nurse (p = 0.397), (p = 0.915), time working in the institution (p = 0.756), working time in the institution (p = 0.756), working hours in the institution (p = 0.282), period working in the institution (p = 0.925), other employment bonds (p = 0.867) and function associated with stress measure (p = 0.185)..
Among the variables analyzed, it was observed that the variable significant event in life had a significant association with stress (p = 0.030). Thus among the participants who experienced these events, the odds ratio for the medium stress was of 2.470. See Table 2.
TABLE 2:
Bivariate analysis of factors associated with stress according to the
variables studied. Poços de Caldas-MG, 2014. (N = 100).
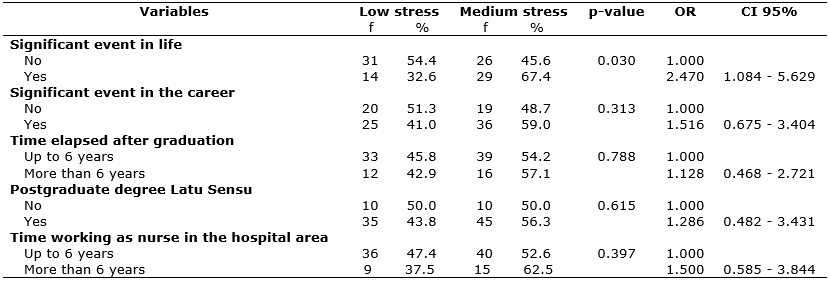
(*)
Application of the Chi-Square Test of Pearson
OR = Odds ratio (CI) CI = Confidence Interval
In the present study, the significant events in the life of the participants in the study were loss (death) of a loved person and birth of a child/grandchild (23.3%).
Events that permeate the lives of people require individual responses to regain the lost balance. Therefore, the feelings of pleasure and suffering are basically determined by the dynamics established between the life history of the workers and the work organization24,32.
Death is an event that is never expected for oneself or for beloved people. Death is, therefore, characterized as a distant possibility, and, in this light, people remain confident toward the future and the fulfillment of dreams. A simple premonition of the proximity with death instills in the human being a feeling of agony32.
, Only two variables that obtained significant associations were elected in the logistic regression analysis, which resulted in an adjusted final model. The variables were practice of physical exercises and significant event in life. Therefore, the logistic regression results showed that the positive practice of physical exercise decreases by 2.95-fold the individual's chance of developing stress (p = 0.020) and the presence of a significant event in life increased by 3-fold the chance of the person to develop stress (p = 0.012), as shown in Table 3.
TABLE 3:
Estimation of the parameters of the logistic regression model of the
independent variables with the stress measure. Poços de Caldas-MG, 2014. (N
= 100).

OR: odds ratio;
(*): P < 0.05.
(**)
Calculation of OR: parameter less than 1, the value 1 was divided by 0.339,
resulting in 2.95.
Practice of physical exercise showed a significant correlation with the ability to work. Thus, workers who practice any sort of physical exercise presented a lower percentage of low ability to work when compared to those who did not practice it (p = 0.02), thus interfering with their level of stress33.
CONCLUSION
Stress is present among the evaluated nurses, especially in functions related to the administrative activities of the unit, which express their functioning. There are risk factors that are present in the work environment, associated with the work components and that are linked to the organization and the environment, and can contribute to the development of stress.
The cross-sectional design of the study and the sample size may have been a limiting factor to the generalization of the findings. However, the study met the proposed objectives, demonstrating the reality of the hospitals of the mentioned municipality. The data can help hospital institutions to reflect on the stress experienced by nurses and on the implementation of strategies associated with the health of workers and the coping with stress.
REFERENCES
1.Teixeira RC, Mantovani MF. Nurses with chronic diseases: relationships with illness, prevention and the work process. Rev. Esc. Enferm. USP. 2009; 43(2): 415-21.
2.Bianchi ERF. Hospital nurses and stress. Rev. Esc. Enferm. USP. 2000; 34(4): 390-94.
3.Miranda EJP, Stancato K. Risks to the health of the nursing team in intensive care units: a proposal of integral health approach. Rev. bras. Tue. intensive. 2008; 20(1): 68-76.
4.Rocha MCP, Martino MMF. Stress and quality of sleep of nurses in the different hospital shifts. Rev. Esc. Enferm. USP. 2010; 44(2): 280-6.
5.Lipp MEN, Malagris LEN. Emotional stress and its treatment: cognitive-behavioral psychotherapies. Rio de Janeiro: Artmed; 2001.
6.Araujo TM, Aquino E, Menezes G, Santos CO, Aguiar L. Psychosocial aspects of work and psychic disorders among nursing workers. Rev. saúde pública (Online). 2003; 37(4): 424-33.
7.Costa JRA, Lima JV, Almeida PC. Stress in the work of nurses. Rev. Esc. Enferm. USP. 2003; 37(3): 63-71.
8.Oliveira EB, Souza NVM. Stress and technological innovation in a cardiology intensive care unit: hard technology. Rev. enferm. UERJ. 2012; 20(4): 457-62.
9.Domingos NAM, Miyazaki MCOS, Valério NI, Pucci FF. Stress of employees of a hospital school. HB scientist. 1996; 3(1): 15-8.
10.Schmidt DRC, Dantas RAS, Marziale MHP, Laus AM. Occupational stress among nursing professionals in the surgical ward. Text & context enferm. 2009; 18(2): 330-7.
11.Montanholi LL, Tavares DMS, Oliveira GR. Stress: risk factors in the work of hospital nurses. Rev. bras. enferm. (Online) 2006; 59(5): 661-5.
12.Pafaro RC, Martino MMF. Study of stress among nurses with a double shift in a pediatric oncology hospital in Campinas. Rev. Esc. Enferm. USP. 2004; 38(2): 152-60.
13.Bianchi ERF. Bianchi stress scale. Rev. Esc. Enferm. USP. 2009; 43: 1055-62.
14. Inoue KC, Versa GLGS, Murassaki ACY, Melo WA, Matsuda LM. Occupational stress in intensive care nurses who provide direct care to critical patients. Rev. bras. enferm. (Online) 2013; 66(5): 722-9.
15. Guido LA, Linch GFC, Pitthan LO, Umann J. Stress, coping and health status among hospital nurses. Rev. Esc. Enferm. USP. 2011; 45(6): 1434-9.
16.Guerrer FJL, Bianchi ERF. Characterization of stress in nurses of intensive care units. Rev. Esc. Enferm. USP. 2008; 42(2): 355-62.
17.Versa GLGS, Murassaki ACY, Inoue KC, Melo WA, Faller JW, Matsuda LM. Occupational stress: evaluation of intensive care nurses who work at night shifts. Rev. gaúch. enferm. 2012; 33(2): 78-85.
18.Murassaki ACY, Versa GLGS, Inoue KC, Melo WA, Matsuda LM. Stress in intensive care nurses and the condition of being head/non-head of household. Ciên. take care Cheers. 2011; 10(4): 755-62.
19.Panzini GP, Bandeira DR. Religious/spiritual coping. Rev. psiquiatr. clinic 2007; 34(1): 126-35.
20.Oliveira E, Rolim MA. Factors influencing nurses to use physical activity in the care of psychiatric patients. Rev. Esc. Enferm. USP. 2003; 37(3): 97-105.
21.Porto AR, Rodrigues SS, Joner LR, Noguez PT, Thofhrn MB, Pai DD. Health self-assessment and chronic diseases among nurses from Pelotas/RS. Rev. enferm. Enferm. 2013; 15(3): 763-71.
22.Lima GF, Bianchi, ERF. Stress among hospital nurses and the relationship with sociodemographic variables. REME rev. min. Enferm. 2010; 14(2): 210-8.
23.Souza NVDO, Cunha LS, Pires AS, Gonçalves FGA, Ribeiro LV, Silva SSLF. Socioeconomic and health profile of nursing workers from the polyclinic Piquet Carneiro. REME rev. min. enferm. 2012; 16(2): 232-40.
24.Seleghim MR, Mombelli MA, Oliveira MLF, Waidman MAD, Marcon SS. Stress symptoms in nursing workers of an emergency unit. Rev. gaúch. enferm. 2012; 33(3): 165-73.
25.Zagonel I P S. Transitional human care in the nursing trajectory. Rev Latinoam enferm. (Online) 1999; 7(3): 25-32.
26. Kestenberg, CCF, Felipe, ICV, Rossone, FO, Delphim, LM, Teotonio, MC. The stress of the nursing worker: a study in different units of a university hospital. Rev enferm. UERJ. 2015; 23(1): 45-51.
27.Martins LMM, Bonzatti, JAG, Vieira, CSCA, Parra, SHB, Silva, YB. Stressful agents at work and suggestion to soften them: opinions of postgraduate nurses. Rev. Esc. Enferm. USP. 2000; 34(1): 52-8.
28.Pereira CA, Miranda LCS, Steps JPO. Occupational stress of the nursing team in the private sector. Rev. pesqui. cuid. fundam. (Online) 2009; 1(2): 196-202.
29.Beleza CMF, Gouveia MTO, Robazzi MLCC, Torres CRD, Azevedo GAV. Occupational risks and health problems perceived by nursing workers in a hospital unit. Cienc. enferm.2013; 19(3): 73-82.
30.Monte PF, Lima FET, Neves FMO, Studart RMB, Dantas RT. Stress of professional nurses who work in intensive care units. Acta paul enferm. 2013; 26(5): 421-7.
31. Martins JTM, Robazzi, MLC, Robroff, MCC. Pleasure and suffering in the team work of nursing: a reflection in the light of dejouriana psychodynamics, Rev. Esc. Enferm. USP. 2010; 44(4): 1107-11.
32. Santos EM, Sales, CA. Mourning relatives: existential phenomenological understanding of their experiences. Text & context enferm. 2011; 20(1): 214-22.
33. Raffone AM, Hennington EA. Evaluation of the functional capacity of nursing workers. Rev. saúde pública (Online). 2005; 39(4): 669-76.