RESEARCH ARTICLES
Nursing Consultation of the Diabetic Patient Using Protocol Staged Diabetes Management
Jéssica Sâmia Silva TôrresI; Ionara Holanda de MouraII; Layla Gonçalves do Nascimento MacêdoIII; Ana Roberta Vilarouca da SilvaIV; Paulo César de AlmeidaV
INurse. Scholarship by the Primary Health Care Program in the municipality of Patos, Piauí, Brazil. E-mail: samia_520@hotmail.comABSTRACT: This study aimed to analyze the nursing consultation to the implementation of the Protocol Staged Diabetes Management in two family health units from the city of Picos, PI. Descriptive and cross sectional study, conducted with 80 patients of both genders enrolled in the Family Health Strategy of the Ministry of Health of Brazil. Data collection occurred through a questionnaire applied in the period of March-April 2011. The results revealed an increase in abdominal circumference in 67.4% of respondents, while 36.3% had blood pressure consistent with hypertension stage I. In addition, 85% made use of antidiabetes medication. It was observed that 58.7% said that had fruit consumption and 55% said that had consumption of vegetables daily. It is concluded that the use of the protocol during nursing consultations enabled characterization of the sample and serve to standardize the service in order to establish a human and holistic care.
Keywords: Protocols; diabetes mellitus; hypertension; nursing care.
INTRODUCTION
Diabetes Mellitus (DM), considered one of the major public health problems, is in ascendancy with regard to alarming rates of people affected by disability and premature mortality, as well as the costs involved in its control and treatment of its complications. Among Latin America's urban population, the prevalence of diabetes is between 4 and 8% and is higher in countries or areas with a low or medium socioeconomic status1.2.
In this way, the multidisciplinary team, besides providing the patient all the information about his disease, they need to be together for a period of time, in order to help him in making decisions of numerous situations lived with diabetes3. In addition, the complexity of diabetes treatment in daily life, requires the health team being qualified for assistance, where nursing seeks to contemplate an integrated approach to all body systems, plus find a humanized care4.5.
To this end, it is necessary to establish protocols that contribute to guarantee a better service, ensuring individually care, standardization of records and decreased costs.
Given this, this study aimed to analyze the nursing consultation with the application of the Protocol Staged Diabetes Management (PSDM) in two family health units from the city of Picos-PI.
LITERATURE REVIEW
Several protocols have been used throughout the world with the purpose to systematically monitor the diabetic patient to prevent chronic complications during the evolution of DM. The first protocol, called the Diabetes Control and Complication Trial Research (DCCT) conducted in the United States of America with DM1 patients, demonstrated a reduction of complications arising from diabetes. After this protocol, there were already diabetic care protocols implemented in several countries, such as Chile, the United Kingdom, Argentina and Brazil, where also besides several protocols implemented the PSDM was also used6.
The PSDM is a protocol of systematized care for he diabetic patient, developed by the International Diabetes Center (IDC), Minneapolis-USA, in 1989, containing a text book and two quick guides for the multidisciplinary team assit the diabetic patient with specific criteria for the establishment of therapy and follow-up, with a view to improve the metabolic control of the diabetic patient and empower the team to clinic practice6.
The guide includes three therapeutic steps. The nutritional step, constituting food guidance and implementation of a program of physical activity to help patients reach their metabolic goals. The step called oral agents, about the use of oral anti-diabetes. Finally, the insulin step, concerning the rapid acting insulin administration, intermediate and long3.
The therapeutic steps indicate which is the type of treatment selected for the patient. For each therapeutic step, the patient cycles through three stages of treatment, as: the initial phase, phase of adjustment and maintenance phase, since that the diabetic patient is a continuous disease that starts with the diagnosis and evolves into the adjustment phase until the objectives are achieved. At that point, the therapy is maintained. Thus, the diabetic patient care is defined through the therapeutic steps that indicate the expected progress3.
The PSDM, as already mentioned, has already been used in several countries, being quite accepted by the population. In Brazil, the lack of professional autonomy and training of nurses in diabetes education are factors that hinder the use of this kind of protocols3.
METHODOLOGY
This is a descriptive and cross sectional research, held in two family health units of the municipality of Picos-PI. The population was composed of 213 patients with diabetes, where the sample calculated in accordance with formula for finite population was of 80 participants. The following inclusion criteria were used: to be registered in the family health strategy, have diagnosis of DM type 2 (DM2) and participate in all stages of the research.
The data were collected from March to April 2011, by using a semi-structured form, covering the following topics: age, gender, family background, life habits, current symptoms listed by the patient, current treatment of DM2, difficulties found, medication use, among others.
Initially, participants answered to the interview where personal data and clinical information were collected. Then, a measuring weight, height, waist circumference and blood pressure (BP) was performed. The weight data were obtained with individuals barefoot and with light clothes, using a portable analog scale with ability to record 120 Kg. The height was measured with the use of tape measure, with precision of 0.5 cm, fixed in a smooth wall. The height measurements were taken with barefoot participants, with feet together and in parallel, in the standing position and looking forward, with the support of a ruler placed on the heads of the individuals, to ensure measurement accuracy in the measuring tape. From the two values, the body mass index (BMI) was calculated, whose interpretation was based on the recommendations of the Ministry of Health7. The waist circumference was measured in lesser curvature located between the ribs and iliac crest, with flexible and inelastic measuring tape without compressing tissues, being the interpretation based on Ministry of Health8.
In PA measurement aneroid sphygmomanometers were used, measured by INMETRO, immediately before its use and with wide rubber cuff closer to 40% of the circumference of the arm. As recommended, the cuff was placed 2 cm to 3 cm before the antecubital fossa. The diaphragm was free of clothes, the palm of the hand facing up and the right arm was preferred in order to unify the readings9.
It is important to note that three measures of blood pressure were measured, discarding the first and considering the mean arterial pressure obtained in the last two.
Regular physical activity is considered the recommendations of the Ministry of Health7, walking about 5 min to 10 min in flat terrain, increasing weekly until reaching 30 min to 60 min daily, 5 to 7 days a week. The shoes should be comfortable, avoiding blisters and calluses; the intensity of physical activity should be increased gradually, aiming to achieve moderate intensity (60% and 80% of maximum heart rate). In relation to smoking and alcoholism, the self-reference of the participants was considered.
Data analysis took place with the help of the software SPSS version 17.0. The study was submitted to the Ethics Committee in Research of the Federal University of Piauí and approved with the CAAE: 0392.0.045.000-10, being followed all the recommendations of work involving human beings. All the participants signed an informed consent.
RESULTS AND DISCUSSION
Of 80 (100%) of participants, 61.3% were female, between 51 to 70 years old (47.5%) and of brown color (42.5 percent), with an average age of 65.06 years old.
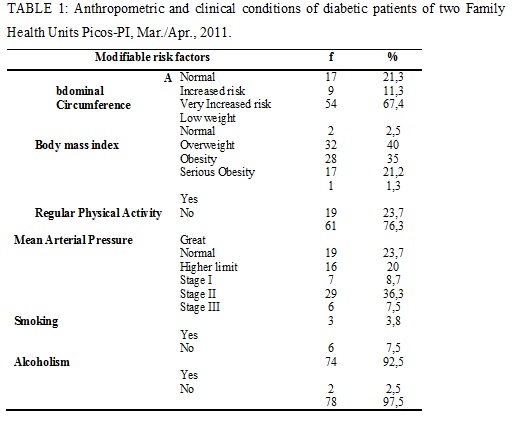
When analyzing the variable waist circumference, it is observed that 54 (67.4%) presented increased risk for cardiovascular diseases, 40% were with normal BMI and 76.3% reported not practising regular physical activity. In addition, 29 (36.3%) had abnormal values compatible with hypertension stage I and most of the respondents reported not being smokers -74 (92.5%) and not use any type of alcoholic beverage – 78 (97.5%) as shown in Table 1.
Considering the waist circumference, a high prevalence of individuals with increased risk for cardiovascular disease was observed, where 40.9% of men and 62.3% of women owned CA values above the limit considered normal. Another study of Fortaleza-CE found that obesity was present in 42 individuals (32.3%), while abdominal obesity appeared in 110 of the samples (84.6%)10. In relation to BMI, the study showed that most of the respondents was with normal BMI, which differs from the study done in 2010, where 55% of respondents had overweight11. A common difficulty found to the DM control refers to the maintenance or reduction of body weight which is related to inappropriate eating habits and the life style12.
Most of the samples - 61 (76.3%) did not practice any kind of physical activity in their daily lives. Population based cross sectional study with 12,402 adult and 6,624 elderly samples of 23 Brazilian States, have identified that in relation to the practice of physical activity among individuals who reported having DM, 82.6% (CI 95% 79.0-86.1) of adults and 88.2% (CI 95% 86.3-90.1) of the elderly were considered insufficiently actives13.
As for the blood pressure values, 29 (36.3%) had abnormal levels compatible with hypertension stage I, upper value to the ones found in other work with diabetics, where 19.5% had associated and uncontrolled hypertension and diabetes, and 15.5% had some complications, such as cerebrovascular accident14.
Another risk factor emphasized, is the practice of smoking. In this study it was clear that participants have low frequency of this practice, since 74 (92.5%) declared not to be smokers, unlike the results of previous studies15.16, in which there was a greater prevalence of smoking (14.3% and 19.4%, respectively). In relation to the practice of alcoholism, the participants had a low prevalence of intakes, because only 2.5% reported the use of some type of alcoholic beverage, different results of research carried out in 2013, which had positive response to alcoholism in 25% of patients with diabetic foot and 11.1% in patients with retinopathy diabetes17.
In relation to variable diagnostic time, 75% found the DM for less than 10 years. Besides, 62.5% used as criteria for diagnosing the fasting glucose test and most of them joined the mainly medicated treatment (85%), with emphasis on the use of glibenclamide 5 mg and metformin 830 mg. Most of them emphasized the classic symptoms of DM (polyuria, polyphagia, polydipsia and loss of weight) and most have or had at least one individual for the first degree of kinship diagnosed with SAH (45%) or with DM (43.7%) as shown in Table 2.
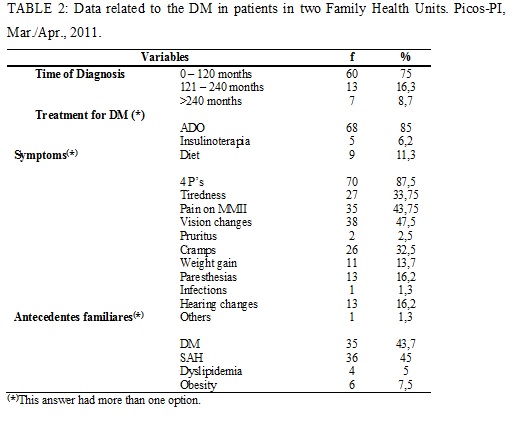
A similar study showed that 67.5% used antihypertensives, which inhibitors of angiotensin-converting enzyme (ACE) and inhibitors of angiotensin receptor blockers (ARBS) represented 84%18. In another research conducted in Rio de Janeiro, 49.4% of the sample had family history for cardiovasculares diseases19.
Thus, being diabetes a preventable pathology, the nurse has an important role, implementing preventive measures and promoting integral care for the patient with diabetes. That is why it is important for the use of the PSDM6, a multidisciplinary team, with the aim of intensifying the strategies for obtaining a good metabolic control; to promote training courses in education in diabetes20.21; to develop intervention research with diabetic patients, promoting the modification of habits and lifestyle, as well as to allow understanding the factors that interfere with and/or easy to achieve metabolic control and establish a permanent communication way between the professionals of the health institutions and patients, mainly at the stage of initiation and/or adjustment of therapy in diabetes.
CONCLUSION
The DM is considered one of the chronic diseases of high cost, both for the health of the patient as to public health, especially in the case of chronic complications that he carries and which can be avoided with a simple change in the habits of life of the population.
Studies that enable the diagnosis, as well as the monitoring and the risk factors become necessary within this population, to support prevention of complications.
It is concluded that the use of the Protocol during the nursing consultation enabled to characterize the sample and will serve as a standardization of the service in order to establish a human and holistic assistance.
In this context, it is observed the importance of nurses that act continuously on the day of patients and are inserted into all levels of assistance, earned their workspace within the health teams dealing with patients with chronic diseases. This professional can act together to a patient with diabetes and his family, with the possibility of an educative work, expanding the consciousness of this clients in recognizing chronic complications arising from this disease.
The results obtained in this research, as well as our experience with patients with diabetes, strengthen our conviction that there is a need for guidance and continuous monitoring for diabetic patients, even those who are in metabolic control.
It is suggested, therefore, that this type of study is carried out in other FHU, to broaden the sampling universe, in order to be fundamental a diabetic care protocol aiming at standardization of customer service, seeking a humanized and holistic care, a health education and a decrease of complications that diabetes offers this community, in order to reduce public spending and increase the quality of life of people, starting with the training of nurses in the use of the Protocol.
REFERENCES
1. López-Jaramillo P, Sánchez RA, Diaz M, Cobos L, Bryce A, Parra-Carrillo JZ, Lizcano F. Consenso latino-americano de hipertensão em pacientes com diabetes tipo 2 e síndrome metabólica. Arq Bras Endocrinol Metab. 2014; 58: 205-25.
2. Freitas RWJF, Araújo MFM, Marinho NBP, Damasceno MMC, Caetano JA, Galvão MTG. Fatores relacionados ao diagnóstico de enfermagem autocontrole ineficaz da saúde entre diabéticos. Acta Paul Enferm. 2011; 24: 365-72.
3. Zanetti ML, Otero LM, Peres DS, Santos MA, Guimarães FPM, Freitas MCF. Evolução do tratamento de pacientes diabéticos utilizando o protocolo staged diabetes management. Acta Paul Enferm 2007; 20: 338-44.
4. Teixeira CRS, Becker TAC, Citro R, Zanetti ML, Landim CAP. Validation of nursing interventions in people with diabetes mellitus. Rev esc enferm USP. 2011; 45: 173-9.
5. Mascarenhas NB, Pereira A, Silva RS, Silva MG. Systematization of Nursing Assistance to patients with Diabetes Mellitus and Chronic Renal Insufficiency. Rev Bras Enferm. 2011; 64: 203-8.
6. Miyar LO. Implementação e avaliação de atendimento ao paciente diabético utilizando o Protocolo Staged Diabetes Management. f. [tese de doutorado] Ribeirão Preto (SP): Universidade de São Paulo; 2005.
7. Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Estratégias para o cuidado da pessoa com doença crônica: hipertensão arterial sistêmica /Ministério da Saúde, Secretaria de Atenção à Saúde, Departamento de Atenção Básica. – Brasília: Ministério da Saúde, 2013.
8. Sociedade Brasileira de Hipertensão. VI Diretrizes Brasileiras de Hipertensão. Rio de Janeiro: SBH; 2010.
9. Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Estratégias para o cuidado da pessoa com doença crônica:diabetes mellitus. Brasília (DF): Ministério da Saúde; 2013.
10. Machado SP, Rodrigues DGC, Viana KDAL, Sampaio HAC. Correlation between body mass index and anthropometric indexes of abdominal obesity in patients with type 2 diabetes mellitus. Rev Bras Promoç Saúde. 2012; 25: 512-20.
11. Vilarinho RMF, Lisboa MTL. Diabetes mellitus: fatores de risco em trabalhadores de enfermagem. Acta Paul Enferm. 2010; 23 (4): 557-61.
12. Oliveira VA, Santos MA, Andrade NHS, Teixeira CRS, Rodrigues FFL, Zanetti ML. Body perception among women with diabetes mellitus and obesity. Rev enferm UERJ. 2014; 22:251-7.
13. Seus TLC, Siqueira FV, Silveira DS, Tomasi E, Thumé E, Silva SM, Dilelio A. Self-reported of diabetes and physical activity in Brazil. Rev Bras Ativ Fis e Saúde. 2012; 17: 520-31.
14. Silva DB, Tereza Alves de Souza, Célia Maria dos Santos, Mércia Marques Jucá, Thereza Maria Magalhães Moreira, Mirna Albuquerque Frota. The association between hypertension and diabetes in a Family Health Center. Rev Bras Promoç Saúde. 2011; 24:16-23.
15. Rodrigues DF, Brito GEG, Sousa NM, Rufino TMS, Carvalho TD. Prevalência de Fatores de Risco e Complicações do Diabetes Mellitus Tipo 2 em Usuários de uma Unidade de Saúde da Família. Rev Bras de Ciência da Saúde. 2011; 15: 277-86.
16. Ribeiro AG, Cotta RMM, Ribeiro SRM. A Promoção da Saúde e a Prevenção Integrada dos Fatores de Risco para Doenças Cardiovasculares. Ciência & Saúde Coletiva. 2012; 17:7-17.
17. Przysiezny A, Rodrigues KF, Santiago LH, Silva MCV. Características sociodemográficas de pacientes com diabetes mellitus portadores de pé diabético e ou retinopatia diabética atendidos em 16 unidades de Estratégia de Saúde da Família de Blumenau. Arq Catarin Med. 2013; 42(1): 76-84.
18. Comar JF, Matsuzaki RC, Teixeira CJ, Bazotte RB. Perfil de pacientes diabéticos tipo 2 usuários de insulina disponibilizada pela Secretaria Municipal de Saúde de Maringá, PR, Brasil. Arq. Ciênc. Saúde UNIPAR. 2011; 15: 243-246.
19. Martins LN, Souza LS, Silva CF, Machado RS, Silva CEF, Vilagra MM, Carvalho CVA. Prevalência dos Fatores de Risco Cardiovascular em Adultos Admitidos na Unidade de Dor Torácica em Vassouras, RJ. Rev Bras Cardiol. 2011; 24: 299-307.
20. Luna NSA, Baeza MR, Castell EC, Santos FC, David HL, Castillo MMA. Intervención educativa: implementación de la agencia de autocuidado y adherencia terapéutica desde la perspectiva del paciente diabético. Rev. enferm UERJ. 2013; 21: 289-94.
21. Diógenes MAR, Souza AKP, Cavalcante IP, Lopes LCO, Rebello MMCB. Insulinoterapia: conhecimento e práticas utilizadas por portadores de diabetes mellitus tipo 2. Rev enferm UERJ. 2012; 20: 746-51