ORIGINAL RESEARCH
Knowledge and practice of breast self-examination among night-shift public school students
Lorena Campos MendesI; Thaís Cristina EliasII; Sueli Riul da SilvaIII
I
Nurse. Master of Health Care from the Federal University of Triângulo
Mineiro, Uberaba, Minas Gerais, Brazil. E-mail. E-mail:
lorena_camposmendes@hotmail.com
II
Nurse. Master of Health Care from the Federal University of Triângulo
Mineiro, Uberaba, Minas Gerais, Brazil. E-mail: thaiscelias2@hotmail.com
III
Nurse. PhD in Fundamental Nursing. Professor, Graduate Program, Federal
University of Triângulo Mineiro, Minas Gerais, Brazil. E-mail: sueliriul@terra.com.br
IV
We would like to thank the following funding organization for this study:
Coordination for the Improvement of Higher Education Personnel – social
demand
DOI: http://dx.doi.org/10.12957/reuerj.2017.13746
ABSTRACT
Objective: to ascertain the effectiveness of educational activities relating to breast self-palpation (BSP) conducted with students. Method: this quasi-experimental study of night shift upper secondary students, young adults and teachers at a public school was approved by the Research Ethics Committee of the Triângulo Mineiro Federal University (Protocol 2585). Application of an instrument to ascertain prior knowledge on the subject was followed by an educational activity on BSP. Later the instrument was reapplied and the responses compared with those from the previous application. Results: 540 students participated in the study. The question with the highest proportional increase in score (44.1%) asked who should perform BSP and the question that aroused most attention (for the high error rate) related to the usefulness of BSP. Statistical tests showed increased knowledge. Conclusion: the educational activity had a major effect on this population's knowledge, and positive educational impact, making that knowledge more homogeneous.
Keywords: Breast self-examination; health education; nursing; women's health.
INTRODUCTION
In Brazil, cancer (CA) has gained the spotlight and with it, space in political and technical agendas at all government levels. According to the World Health Organization (WHO), in 2012, an estimated 20 million cases of CA were expected, and 8 million people died from neoplasms, with the greatest incidence occurring in low and middle income countries1 . Thus, CA is currently considered a public health problem, as the Brazilian Mortality Information System (SIM) registers that it represents the second leading cause of death by disease in Brazil2.
Breast CA is probably the most feared malignant neoplasm by women because of its psychological impact, as it involves aspects related to the perception of feminine sexuality and self image2. Even though breast CA can present good prognosis when detected and treated early, mortality rates in Brazil remain high, as the disease continues to be diagnosed mostly at advanced stages1.
In light of the above, health professionals still have much to do in the field of health promotion and breast CA prevention among the population 3. It is important to create strategies and programs to reduce the number of breast CA cases, using educational activities to awaken the interest of women in self-care, primary prevention through lifestyle changes, and carrying out breast CA screening tests.
To create such strategies, it is necessary to determine the knowledge and practices of women regarding the breast self-exam (BSE). The aim of the present studyIV was to verify the effectiveness of health education activities about BSE conducted with students attending night high school, youth and adult education (EJA), and teaching training to contribute to the reduction of morbimortality rates due to breast CA.
LITERATURE REVIEW
According to data from the National Cancer Institute of Brazil (INCA), breast cancer is the most common neoplasm among women. In 2012, 1.67 million new cases of this neoplasm were expected worldwide, representing 25% of all types of CA diagnosed in women. In 2015, the Brazilian Ministry of Health (MS) estimated 57,960 new cases of primary breast CA in the 2016-2017 biennium, with an estimated risk of 56.20 cases per 100,000 women. It is worth mentioning that this estimate increased in comparison with 2014, a year in which 57,120 new cases were expected and the estimated risk was of 56.09 cases per 100,000 women1,4.
In this context, a study conducted with gynecological CA patients at a teaching hospital in the state of Minas Gerais, Brazil, in 2009 corroborates this data, in which 45% of the population undergoing chemotherapy presented breast CA5. Another study in 2011 found breast CA to be the main cause of death due to neoplasms in a population of women residing in the municipality of Juiz de Fora, Minas Gerais. Moreover, the trend analysis showed a growth in mortality by breast cancer throughout the years6.
To control the morbimortality rate of this disease, early breast CA screening strategies must be implemented. Such strategies must include education activities with women and health professionals, teaching them how to recognize the signs and symptoms that characterize the disease and facilitating access to health services7.
Educational activities are highly important, as many women, due to their values and culture, are not familiar with CA prevention and early detection measures2. It is important that health professionals encourage women to conduct BSE as often as they feel like it, with no specific technical recommendation, emphasizing casual discovery of minor breast changes and then immediately seeking out health services for diagnostic clarification4,7.
Education activities in nursing team practices have been increasingly discussed, as nurses stand out as the main actors in the care process via health education, fostering the development of actions that qualify patient care and care provision, and providing greater autonomy to individuals over their own health8,9.
Although screening tests for breast CA are widely disseminated by the media and health professionals, studies have shown that knowledge about the neoplasm is not complete and homogenous10,11. BSE promotes self-care, providing women with greater self-awareness. Thus, as professionals responsible for patient care and who adopt the principle of implementing care and educational practices to motivate and qualify individuals, nursing teams play an important role in fostering self-care 12.
Additionally, studies have shown increases in knowledge about the theme following educational activities with groups11, corroborating the importance and need to conduct more education activities that enable the exchange of knowledge between professionals and listeners.
Despite the importance of health education activities in nursing practice, there are few studies that measure the effectiveness of self-care and educational activities in reaching the proposed objectives.
METHODOLOGY
This was a quasi-experimental before-and-after study extracted from a Master's dissertation. Research was conducted in 2014 with all the students aged 18 years old or older attending night high school, EJA, or teacher training at all state high schools in the municipality of Uberaba, Minas Gerais, Brazil. Participants had to be enrolled in the regular and in-person modality, and agree to participate in the study by signing informed consent forms.
Currently, the municipality has 23 public night schools, however, 20 schools met the inclusion criteria. Thus, 540 students regularly enrolled in high school, EJA, or teacher training participated in the study by answering the questionnaire.
For data collection, the study subjects were located, identified, and approached at the cited education facilities. The procedures were conducted ensuring privacy and respect, in a woman-only environment to allow participants more freedom. The questionnaires were answered individually, ensuring anonymity.
A self-administered instrument was developed by the researchers of this study, structured with open- and closed-ended questions, informed by the literature and research in the area. The instrument was submitted to analysis by three experts PhD in nursing with knowledge in the research area to ensure face and content validity.
Initially, the instrument was given to subjects with the goal of verifying their previous knowledge on the topic of study. Then, in the same location, the educational activity about BSE was developed. Following the intervention, the instrument was given once more to the subjects to measure the knowledge acquired and compare it with their previous knowledge.
The educational activities lasted an average of 45 minutes and were based on dialogue and exchange of knowledge between the researcher and participants. Didactic resources were used to give a talk about BSE, and understanding was facilitated through the use of audiovisual resources, such as a banner.
Data were compiled using a Microsoft Excel® database. Inconsistencies were detected using double entry verification. Statistical analysis was conducted with the help of the Statistical Package for the Social Sciences (SPSS) version 20.
The quantitative variables were analyzed using central tendency and variability measures (mean, standard deviation, median and range). Qualitative variables were analyzed by obtaining simple frequency distribution and contingency tables for bivariate analysis.
A paired t-test was applied to questionnaire scores before and after the educational activity to assess the effectiveness of the intervention, and Cohen's D test was used to assess effect size and the intervention's educational potential. McNemar's test was employed to assess questionnaire items relative to BSE, measuring whether knowledge increased after the intervention in each item. Significance level was set at α=0.05. The results were organized in bivariate tables and discussed in relation to the literature specific to the area.
The study protocol was submitted to and approved by the Research Ethics Committee (CEP) of the Federal University of Triângulo Mineiro (UFTM), under protocol CEP/UFTM: 2585. Ethical aspects were based on Resolution no. 196/96 about research involving human beings, because the protocol was approved before the new legislation about ethics in research with human beings.
RESULTS AND DISCUSSION
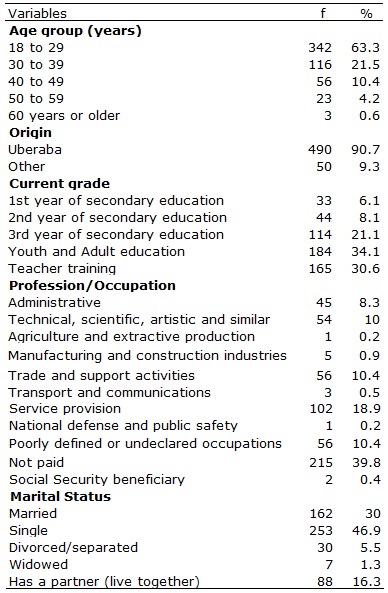
Of the 540 women who participated in the study, mean age was 27.97 years, with a median of 24 years, standard deviation of 10.25 years, ranging between 18 and 65 years. Most (63.3%) were between the ages of 18 and 29 years. Table 1 presents the sociodemographic profile of the participants.
TABLE 1:
Sociodemographic profile of night high school students. Uberaba, Minas
Gerais, Brazil, 2014
The professional categories were divided according to the Brazilian Classification of Occupations (CBO) of the 1991 census13, with the additional options of unpaid work and Social Security (INSS) beneficiaries. Of the women who participated in the study, 215 (39.8%) conducted unpaid activities, given that a great portion of the population were students who did not work, followed by service provision, 102 (18.9%), such as domestic employees, manicurists/hair dressers, caregivers, and cooks. The most prevalent marital status at the time of the study was single, with 253 (46.9%).
Being familiar with the sociodemographic profile of the population is important, as their knowledge can vary according to age, occupation, and marital status, influencing the direction of educational activities. In this context, and according to sociodemographic data, a study conducted in the same municipality and with a comparable population in 2009 found similar data, indicating that the studied population profile had not varied much over the years11.
These findings corroborate the authors' statement about the importance of learning about the sociodemographic profile of people who can benefit from screening programs, as these characteristics are associated with level of access to information. This is especially true in terms of education level, which was not the case of the present study, as the participants were at similar education levels. Lower-income classes tend to have less access to health services, which can result in less access to information about breast CA14.
Among the information channels used, the most cited were the internet (68.0%) and television (66.3%). Other less cited media and that were not present on the instrument were: health professionals and units (1.7%), mobile phones (1.3%), schools and lectures (0.6%), and books (0.4%).
In a study conducted in 2012 with nursing students in the municipality of Montes Claros, Minas Gerais, the internet and television were also among the most commonly used sources of information15. It is important to be familiar with the information channels most used by the population because of the need to expand dissemination and access to information related to health education, enhancing knowledge and search for self-care.
The media has an important role to play in publicizing information to the population, standing out as one of the main sources of information used; thus, health professionals and the media must work together to teach BSE techniques and the adequate frequency of the exam, encouraging self-care.
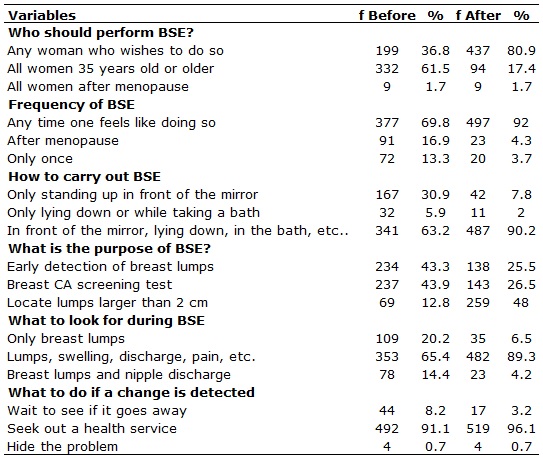
Regarding the answers given by participants, none of the participants scored 100% wrong or right answers, either before or after the intervention. However, there was a considerable increase in the proportion of right answers after the educational activity, as shown in Table 2.
TABLE 2:
Distribution of public night high school students by answers about BSE.
Uberaba, Minas Gerais, Brazil, 2014.
Even though assessment of the knowledge gained about the topic was conducted in a one-off manner, immediately after the educational activity, the intervention was effective in transmitting information to the population. Such gain in knowledge is likely to remain in the long-run, as shown by a study conducted in 2011, which found that before the educational intervention about breast CA, only 6.7% of the women in the study presented adequate knowledge on the theme; but six months after the activity, 93.3% presented adequate knowledge16.
During the educational activities, most questions about BSE were about the difference between benign and malignant lumps, the correct age to initiate BSE, the difference between BSE and mammograms, risk and protection factors, and the main signs and symptoms of breast CA.
Regarding the questionnaire, the item with the greatest proportional increase in right answers, 44.1%, was "who should conduct BSE?" It is believed that this result is due to lack of knowledge before the intervention about the difference between BSE and mammograms.
Another issue worthy of attention is the purpose of BSE, for even though the activity emphasized its true function, self-awareness, many women still believed BSE to be a breast CA screening test or that it could be used in the early detection of breast lumps.
In this context, and corroborating this data, a study conducted in 2013 in a waiting room in an outpatient clinic in the municipality of Uberaba, Minas Gerais, Brazil, found that a considerable part of the participants lacked knowledge about the purpose of BSE, with 52.5% of the participants reporting that BSE allows for the early detection of lumps and 31.5% for breast CA screening test.17.
These data are cause for concern, because the misguided idea of BSE as a screening test or used in the early detection of breast lumps can hinder the use of actual breast CA screening strategies and delay the search for health services. It is important to emphasize once more the importance of health education aimed at providing the population with orientation about the real meaning of BSE and about breast CA screening methods, such as the clinical breast examination (CBE) and mammograms, as recommended by the Ministry of Health.
When asked about their knowledge about BSE, 425 (78.7%) women reported being familiar with it and knowing what it was about. However, the data in table 2 indicates that such knowledge was not complete and homogenous.
Even with the changes in INCA guidelines regarding breast CA screening actions and how to instruct women about breast self-care practices, women's participation in this process is still essential and highly important. The current recommended strategy is to provide information about normal breast changes throughout the menstrual cycle and the main signs and symptoms of breast CA, encouraging women to seek out medical clarification in case of any sign of change, and to conduct BSE with no specified method or frequency4,7,18.
Special mention goes to the finding that 246 (45.5%) of the women reported never having conducted a BSE. This issue is reflected in the fact that breast CA is the malignant tumor that most causes death among women. Not conducting BSE may be explained by lack of women's perception about its importance to help detect changes and the need for specialized medical appointments on a yearly basis, associated with early screening methods3.
Regarding knowledge about BSE before and after the educational intervention, there was an increase in knowledge in the studied population. McNemar's analysis demonstrated a difference before and after the intervention, as the data were statistically significant, thus demonstrating its effectiveness, as shown in table 3.
TABLE 3:
Distribution of public night high school students according to the number
of hits and errors related to APM. Uberaba / MG, 2014.
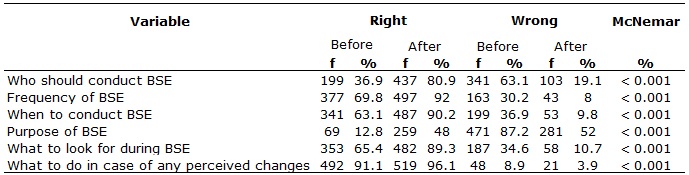
Even though the statistical tests showed that the activity was effective, the percentage of incorrect answers to some questions after the activity was still significant, especially in response to "who should conduct the BSE (19.1%)" and "what is the purpose of BSE (52.0%)". These data reinforce the importance of both group and individual educational activities to expand access to information by women, especially those who belong to vulnerable groups or who for any reason present limited education, as observed among some women during the present study.
Thus, educational activities with the aim of increasing knowledge about self-care are important, both at the individual and collective level. They can contribute to transform the reality of the population and community participation in the process19.
Cohen's D value, or effect size, demonstrated that the activity was relevant in terms of knowledge about BSE20. According to Cohen's D for BSE scores, 1.62, the intervention presented large effect size, indicating a positive educational difference, and reinforcing the importance of educational activities to convey information and impact the population's level of knowledge.
CONCLUSION
The results of the present study demonstrate the need to transmit information about the theme, which is of utmost importance for various populations, and presents itself as an essential tool in nursing care. The educational activities showed the extent of missing information among the participants. From this perspective, it can be inferred that the data indicate the need to create strategies and programs that aim to reduce the number of breast CA cases, awakening the interest of women in self-care, primary prevention through lifestyle changes, and in conducting BSE.
The meetings conducted for this study consisted only of women. This detail was essential so that women could feel more comfortable exposing their doubts and even giving personal examples or those of friends and family.
The educational activity had a positive educational impact as it increased the knowledge about the theme and, in general, the coordinators, teachers and most of the students were interested in more similar educational activities to exchange experiences and receive information about the theme.
Limitations of this study include the administration of the post-intervention questionnaire immediately after the intervention, and not after a period long enough to verify the effectiveness of the activity in changing the participants' behavior, given the limited time available for its execution. This gap in knowledge can serve as a basis for further research in the area.
REFERENCES
1.Ministério da Saúde (Br). Instituto Nacional de Câncer. Estimativa 2016: incidência de câncer no Brasil. Rio de Janeiro: INCA; 2015.
2.Ministério da Saúde (Br). Instituto Nacional de Câncer. Ações de enfermagem para o controle do câncer: uma proposta de integração ensino-serviço. 3ª ed. Rio de Janeiro: INCA; 2008.
3.Portela JRS, Tirado BV. Cáncer de mama: ¿Es posible prevenirlo? Rev Cienc Med. 2011; 15(1): 14-28.
4.Ministério da Saúde (Br). Instituto Nacional de Câncer. Estimativa 2014: incidência de câncer no Brasil. Rio de Janeiro: INCA; 2014.
5.Soares EM, Silva SR. Perfil de pacientes com câncer ginecológico em tratamento quimioterápico. Rev Bras Enferm. 2010; 63(4): 517-22.
6.Rodrigues AD, Bustamante-Teixeira MT. Mortalidade por câncer de mama e câncer de colo do útero em município de porte médio da Região Sudeste do Brasil, 1980-2006. Cad Saúde Pública. 2011; 27(2): 241-8.
7.Ministério da Saúde (Br). Cadernos de atenção básica: controle dos cânceres do colo do útero e da mama. Brasília (DF): Ministério da Saúde; 2013.
8.Ceolin R, Rosa L, Potrich T, Zanatta EA. Educação em saúde como ferramenta para uma atenção integral à saúde da mulher: uma reflexão teórica. Rev Enferm Frederico Westphalen. 2009; 4 e 5(4 e 5):127-37.
9.Sousa LB, Torres CA, Pinheiro PNC, Pinheiro AKB. Práticas de educação em saúde no Brasil: a atuação da Enfermagem. Rev enferm UERJ. 2010; 18(1): 55-60.
10.Silva SR, Lício FC, Borges LV, Mendes LC, Vicente NG, Gomes NS. Atividades educativas na área da saúde da mulher: um relato de experiência. REAS. 2012; 1(1): 106-12.
11.Valente CA, Andrade V, Soares MBO, Silva SR. Women's knowledge about the papanicolaou exam. Rev esc enferm USP. 2009; 43(esp2): 1193-8.
12.Silva IJ, Oliveira MFV, Silva SED, Polaro SHI, Radünz V, Santos EKA et al. Care, self-care and caring for yourself: a paradigmatic understanding thought for nursing care. Rev esc enferm USP. 2009; 43(3): 697-703.
13.Instituto Brasileiro de Geografia e Estatística. Códigos de Ocupações. Rio de Janeiro:IBGE;[citado em: 10/05/2016],1991. Disponível em: http://concla.ibge.gov.br/estrutura/ocupacao-estrutura
14.Freitas CRP, Terra KL, Mercês NNA. Conhecimentos dos acadêmicos sobre prevenção do câncer de mama. Rev Gaúcha Enferm. 2011; 32(4): 682-7.
15.Gomes LMX, Alves MC, Santos TB, Andrade-Barbosa TL, Leite MTS. Conhecimento e prática do autoexame das mamas por acadêmicas de enfermagem. Rev Cubana Enferm. 2012; 28 (4): 465-73.
16.Montañez SP, Alemán IR, Capdesuñer AS, Palácios MC. Modificación de conocimientos sobre cáncer de mama en trabajadoras con factores de riesgo de la enfermedad. Medisan. 2011; 15(1): 92-8.
17.Mendes LC, Silveira CF, Silva SR. Conhecimento de mulheres a respeito do exame de Papanicolaou e do Autoexame das mamas. REAS. 2013; 2(3): 4-17.
18.Thornton H, Pillarisetti RR. 'Breast awareness' and 'breast self-examination' are not the same. What do these terms mean? Why are they confused? What can we do? Eur J Cancer. 2008; 44(15): 2118-21.
19.Oliveira AM, Pozer MZ, Silva TA, Parreira BDM, Silva SR. Extension activities aimed at the prevention and treatment of gynecological and breast cancer: an experience report. Rev esc enferm USP. 2012; 46(1): 240-5.
20.Cohen J. Statistical power analysis for the behavioral sciences. 2ª ed. Hillsdale (NJ): Lawrence Erbaum; 1988.