RESEARCH ARTICLES
Social images among women with precursory lesions of cervical cancer: study of social representations
Maria Cristina de Melo Pessanha CarvalhoI; Ana Beatriz Azevedo QueirozII; Maria Aparecida
Vasconcelos MouraIII
ABSTRACT: The qualitative, descriptive study examined social representations among women with precursor lesions of cervical cancer at a public institution, from February to June 2009, and discussed the women’s social images in relation to their cervical abnormalities. The sixty women participating, all with confirmed diagnosis, undergoing treatment and consenting to the study, were divided into a Reproductive-Age Group (RAG) and Non-Reproductive Age Group (NRAG). Analysis by Free Association of Ideas Test, revealed the categories: the uterus for women with PLCC; meanings attributed to PLCC; and social images among women with PLCC. The lesions were represented by severe disease, fear and death. Images among women with cervical change were connected with the participants’ daily experiences, traversing issues from the social and relational environment. The study offers a contribution to gynecological nursing, enabling effective women's care actions to reduce cases of precursor lesions and cervical cancer.
Keywords: women's health; oncologic nursing; social psychology; cervical intraepithelial neoplasia.
INTRODUCTION
The precursor lesions of cervical cancer/LPCCU are distinguished by the presence of modifications of the original epithelium, constituting precancerous lesions that may progress to cervical cancer1,2,3. The identification of these changes is relevant for prevention and early detection of this type of female cancer, becoming an important public health problem; especially in countries with lower socioeconomic status, the high mortality in the female population evidenced in the Brazilian reality4.
With the experiences of caring for women suffering from such lesions a variety of behaviors were observed; some being committed to the treatment, other finds being just a typical woman problem or approaching to death. This diversity enabled to develop a study that highlighted content integrating the knowledge that these women have present with this problem, seeking to understand the social image built about the woman who has LPCCU. In this sense, the image of this woman is understood as an object of social representation, since she is the bearer of these changes has a dimension of affect (psi) and the other social. They take refuge in previous experiences, accumulated knowledge, values and culture that from social relations are processed the exchange of information contributing to organizing actions against the health problem.
Studies1,2,3 about these issues are relevant involving women with uterine cervical changes, since there is an exclusively technical and biologicist approach, not getting effective answers to combat this problem in the health area; it is necessary to consider the value of a social subject as a thinking subject and there paradigms5. In this perspective, the proposed objective was to analyze the social representations of women with LPCCU and discuss the social images of these women in the uterine cervical abnormalities.
THEORETICAL REFERENTIAL
Research grounded in Social Representations Theory (SRT) essential to understand the constructions of ideas that are part of the common sense of the participants.
The female body represented here by the reproductive organ - the uterus - brings with it fundamental values and meanings in female identity, and through it the relationship of femininity, sexuality, gender and social issues are exposed and gain amplitude. This preparation process is influenced by the previous reference systems and values that involve mobilizing effects in conjunction that contribute to form representations of reality experiments6.
When studying this object is essential to understand the subjectivity involving the complexity of the situation for women's health and their quality of life. Psychosocial issues, not just the epidemiology disease, become essential to adjust not only the behavior and procedures, but the actions of health promotion in the reality of those who experience the problem.
The phenomena of social representations research are psychosocial, keeping relations between the subjective and the social universe of individuals who acquire importance in the routine of life7. In this theory, women process the information coming from the scientific universe with circulating in everyday conversations and knowledge from their experiences. This theory applies to studies on the universe of common sense and invests in unveiling the knowledge that guide individuals in the world8.
Then, it arises the opportunity to offer another dimension to the healthcare professional on how to care through strategies to take this client in accordance with their values grounded throughout their lives. As a professional practice of gynecologic nursing delineates a special care to meet the needs and expectations of these women, aiming to treat them and care for them; contemplating their values and representations, since it must exist, beyond the understanding of the physical dimension, an understanding of the social context in which it is the subject of the disease9.
METHODOLOGY
Qualitative and descriptive research, sustained in Social Representations Theory it procedural precursor. The setting was a federal public health institution in Rio de Janeiro, highlighted as reference in Service Cervical Pathology. Data collection took place between February and June 2009 where 60 women participated. Inclusion criteria were women with confirmed LPCCU, being treated at that institution to accept and participate in the research being excluded if they were in the process of confirming the diagnosis.
The participants were divided into two groups belonging: group of reproductive age (RAG) and non-reproductive group (NRAG), with 30 participants each. This sample was made by variety type, with the criteria of homogeneity critical the phase of a woman's life. To ensure anonymity and acronyms number (I1, I2,...) the interviews were assigned according to the order of arrival of the participants, divided by RAG and NRAG.
Ethical issues met the requirements of Resolution 466/12 of the National Health Council, was approved under the No. 02/2008 by the Research Ethics Committee of the School of Nursing Anna Nery/Institute for Health Care São Francisco de Assis of the Federal University of Rio de Janeiro. The participants signed a consent form.
The interviews were individual, starting with the technique of Free Association of Ideas (FAI). This is a technique in which elements emerge after the sentences stimulated for the participant can join the ideas that run through their mind in a clear and spontaneous way10. Inducers terms were: uterus; wound in the uterus; and woman with wound in the uterus, questioned one at a time and separately. For this research purposes the contents present at this early part of the interview were explored and discussed, since the object of this study was focused at this stage.
The technique of thematic content analysis was used that allows uncovering the meanings, knowing the subjectivities that are part of the communications area. The analysis allowed to seek the emergence of relevant senses to the object context. The organization of thematic analysis was oriented in three phases: pre-analysis, material exploration and treatment11.
In the pre-analysis, the data produced was organized by separating the material in both RAG and NRAG groups, to perform the initial reading and promote familiarization of this material. The exploration passed to the analytical treatment of the corpus. Connections of induced words were identified, grouping them and pointing the categories and subcategories. Evocations were grouped and separated by bands which were correlated with each other, either by similarity or contradiction with the problem. Subsequently, the results were presented in tables statements for each inducing word containing the frequency of responses. From the analysis three categories emerged: The uterus for women with LPCCU; The meanings attributed to LPCCU; and social image of women with LPCCU which were analyzed with the theoretical referential.
RESULTS AND DISCUSSION
Participant´s Characterization
Characterization of participants
The age of respondents ranged from 16 to 90 years old and more than half of women in both groups, have education up to elementary school. Over 90% of women in both groups were infected by the Human Papilloma Virus (HPV). The RAG Group made diagnosed with Low-Grade Cervical Intraepithelial Lesion; however, the High-Grade Lesion was very presented in NRAG. The results were organized into topics considering that the subject undergoes a process of reframing their discursive content and contextualizes from the processes of socialization, featuring time lived12.
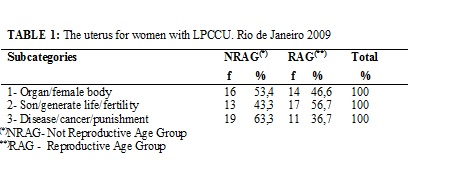
Category 1: The uterus for women with LPCCU
In this category, three subcategories emerged: Organ/female body; Son/generate/fertility and disease/cancer/punishment. The subcategory Organ/female body presented with significant results for the RAG with 14 (46.6%) and NRAG with 16 (53.4%), as shown in Table 1. This result shows that the uterus is a part of objectified the female body to be belonging to women only by their inherent nature to biological function. In the process of objectification, it is showed how the woman rearranges the elements of the representation13. Uterus female organ has emerged as a hegemonic form in both groups, because for years, the woman was restricted to uterus-centrism14.
Here is a testimonial:
Part of woman's body, is the life of a woman. (I44 NRAG)
In this context, the female organ brings the representation assigned to patterns that remain present today as traversing an axis of tradition, one of the constituent elements of social representations7. The social intervenes in various ways by the specific context in which individuals and groups are situated, the communication established by the boards of apprehension provided by codes, values and ideologies linked to social participations9.
For the subcategory Son/generate/fertility, this was mentioned more frequently by the RAG in 17 (56.7%) subjects, showing that this segment anchored the uterus motherhood and reproductive cultural process. In NRAG emerged less frequently, with 13 (43.3%) evocations certainly because the uterus have already completed this considered essential function. The reproductive capacity of women for centuries was the condition of being female, defining motherhood as one true realization of women12. Childbearing function was internalized throughout their lives and formed and built representations since ancient times in sociocultural contexts15.
The LPCCU because it is a condition that affects the uterus, symbol of common sense of reproduction/maternity, influences and is influenced in the representations of these women. Nowadays, this ideas make the woman feel the duty to gestate, which is reinforced by the doctor discourse, reified universe of science, disqualifying them as a social being, if they do not want or cannot be mothers16.
Another testimony:
Uterus is to generate child, it is important because the son comes from it. (I8 NRAG)
The subcategory Disease/Cancer/punishment emerged from the uterus association with experienced health problem. This became more evident in NRAG with 19 (63.3%) evocation, different from RAG, which emerged only in 11 (36.7%). This differentiation, in relation to representations of NRAG, may have been elaborated by no longer be identified as a reproductive being, i.e. the uterus no longer having their social-biological function, it was objectified as a disease keeper (I50 NRAG. The health/disease process should be regarded as a psychosocial phenomenon historically constructed when analyzing the process of being ill12.
To understand the association between uterus and disease in women with LPCCU, the process of becoming ill stops being a casual event and shall be included in the biography of the individual, since each person has a way of living and being ill17. The acceptance of an illness is related to their life history, the nature of the conflict and their social roles17. The social representation is a practical knowledge linking a subject to an object in an attempt to explain something that brings subjetivity9. This connection may have been generated by a sense of sin and punishment, representations that are constructed by feelings of guilt and regret; resulting behaviors sometimes not socially worthy, as treason and abortions.
Only serves to take cancer, bad disease. (I14 RAG)
It is this disease that is punishment for what we did in life. (I52 NRAG)
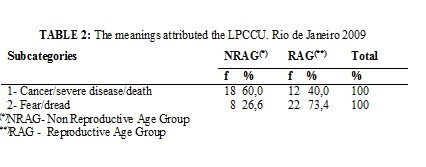
Category 2: The meanings attributed to LPCCU
In this category emerged the subcategories: Cancer/severe disease /death and fear/dread. The first appeared sharply in both groups. However, it was relevant in NRAG with 18 (60%) evocations, reinforcing the anchoring process of LPCCU as a serious disease and may causing death, as shown in Table 2. It is observed that reaffirms the disease/cancer/punishment related to the term inducer uterus. These two subcategories demonstrate that different inducers terms permeate the representation of this thread, that LPCCU causes suffering be considering the cancer itself. It is shown the complexity surrounding the concept of health and illness, life-death by traversing a bio-psycho-social reality18. The disease becomes a threat when it is linked to cancer that has historically been linked to bad experiences, suffering and the possibility of death19. In this idea, the LPPCU opened a range of directions related to disease-suffering-gravity-finiteness dimension of demonstrating affection of social representations.
Here, there are statements:
For me it is death, is the end of it, there's no way. (I19 RAG)
I think it's a very serious disease that has no cure. (I8 NRAG)
The connection of this subcategory with NRAG is justified, perhaps, being a female segment without chance of reproduction, getting sharper the disease process. They incorporate the negative image and diminished social mirror that reflects on women of older age. The RAG experiences the duality between the power of motherhood and the lesion in the uterus, endangering not only their lives but their reproductive condition.
The fear/dread subcategory was different for each group. For NRAG can be understood related with the previous discussion. Women find themselves threatened by this lesion which is represented as a serious disease and can lead to death, therefore, feelings of anxiety and dread may arise. These feelings related to cancer in general and to cervical uterus, are created and perpetuated by the discourse of risk and vulnerability present in LPCCU.
The evidence for this subcategory, with a total of 22 (73.4%) evocations in RAG, brings reflection on values established. Most have some priorities in their lives, like having children, preserve and maintain the bond of marriage and sexuality. They experience the problem as something painful and all these expectations are threatened when they receive a diagnosis they consider dark and devastating20. This fear/dread is implicated in influencing situations in their daily lives, livelihood, with insecurities and uncertainties, according the interviewee exposes:
I'm afraid to not get pregnant, cannot have more children. (I17 RAG)
I'm terrified of my husband leaving me. (I3 RAG)
The diagnosis of LPCCU presented for this segment, different from NRAG, fear of negative feelings that form barriers that impede the treatment of the disease21.
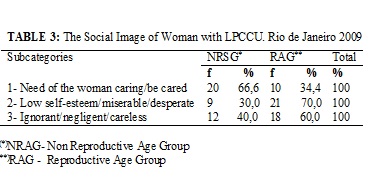
Category 3: Social image of woman with LPCCU
In the case of this category it was possible to divide the subcategories: Need of the woman caring/be cared; Low self-esteem/miserable/desperate and Ignorant/negligent/careless, as shown in Table 3.
Analyzing the subcategory Need of the woman caring/be cared we can see various subjectivities that are instilled on how a woman should act with of LPCCU.
I think women have to seek treatment immediately. (I36 RAG)
The woman has to be careful, go to the doctor. (I41 NRAG)
Woman having LPCCU as a serious illness, may bring serious problems to their health and life, needing care practices. The reified knowledge about health care forecast construction of a representation that contributes to a relevant women´s health meaning16. There is the need to care for and to carry out prescribed treatment to prevent greater diseases. The social representation intervenes in actions enabling the explanation of behavior, guiding behaviors and practices. This defines what is permissible, tolerable or unacceptable in a social context7. When analyzed by group, it was identified this need, most often in NRAG with 20 (66.6%) evocations.
Feeling sick can threat life plans, allowing attitudes relevant to the improvement of health. In care we have the perspective of healing and the ability to interrupt the degenerative process of the disease. It is emphasized that care practices are guided by results of social experiences that produce interpretations, meanings acquired from actions processes in everyday life and have produced imaginary constructions22. In this approach, the social representation is a preparation for the action, remodeling and carried by the elements of the social environment7.
On the other hand, we found that the subcategory Low self-esteem/miserable/desperate showed the greatest relationship with RAG, with 21 (70%) evocations, then the subcategory Ignorant/negligent/careless with 18 (60%).
It is the decrease in woman's ego. Feeling inferior and incapable. (I9 RAG)
These results show that younger women with LPCCU construct meanings of inferiority and incapacity. The context of the representation of the female body is related to synonyms of power in interpersonal relationships, with beauty and social status23.
Regarding the subcategory Ignorant/negligent/careless it can verified the connection that women have made to the source of the problem, reflecting the image of woman with LPCCU; i.e., lack of care and prevention were factors that caused this problem. These references influence the feelings of female devaluation, bringing a connotation of irresponsibility and blame of the woman. It is developed thus the perception of the situation they experience in building a movement that contributes to their self-care24.
Is the woman who does not properly care (I7 RAG)
That's when the woman is ignorant, is slob. (I1 NRAG)
In this topic, content zone changes of social representations with the image of the carrier with LPCCU were accessed. The zone change is composed of elements of the representation that are counter-normative, cognitions or beliefs that are not expressed by the subject under normal production conditions, as they may conflict with moral values or norms of a given group25.
CONCLUSION
The study met the goals from the perspective of a new understanding of women with LPCCU in TRS. The uterus of disabled women with LPCCU; The meanings attributed to LPCCU and social image of woman with LPCCU were the categories of analysis that emerged from the research. It was possible to describe the presence of different meanings given to LPCCU, as well as images of women with uterine cervical changes, explained in their groups. The RAG showed fear facing the possibilities of losses, the strong identification of women with motherhood. On the other hand, the NRAG highlighted the representation of cancer/disease with the possibility of death if not prioritize the care process. It is noteworthy that both meanings conferred to the uterus, the LPCCU and the image of women with cervical changes are linked to the daily experiences of the participants, traversing issues of social and relational environment. This research may contribute to a performance within the gynecological nursing aims to establish immediate and effective self-care that takes into account the LPCCU woman and psychosocial issues that interfere with their image as a woman.
A limitation of the study is partly because it was performed only in a public setting, without investigating the representations of these women in different institutions.
REFERENCES
1. Schiffman M, Castle PE, Jeronimo J, Rodriguez AC, Wacholder S. Human papillomavirus and cervical cancer. Lancet. 2007; 370: 890-907.
2. Bosch FX, You-Lin Q, Castellsagué X. The epidemioly of human papilomavirus infection and its association with cervical cancer. Int J Gynecol and Obstetrics. 2006; 94 (supp. 1): s8-s21.
3. Pandey D, Putteddy S, Rao. Micronucleus assay as a triage tool for borderline cases of cervical dysplasia. Sri Lanka Journal of Obstetrics and Gynaecology. 2011; 33: 104-11
4. Instituto Nacional de Câncer José Alencar Gomes da Silva. Estimativa 2014: incidência de câncer no Brasil. Rio de Janeiro: INCA; 2014.
5. Coelho MS, Silva DMGV, Padilha MIS. Representações sociais do pé diabético para pessoas com diabetes mellitus tipo 2. Rev esc enferm USP. 2009; 43:65-71
6. Secchi K, Camargo, BV, Bertoldo, RB. Percepção da imagem corporal e representações sociais do corpo. Psicologia teoria e pesquisa. 2009; 25:229-36
7. Moscovici S. Representações sociais: investigação em psicologia social. 4ª ed. Petrópolis (RJ):Vozes; 2011.
8. Viana N. Senso comum, representações sociais e representações cotidianas. Bauru(SP): Edusc; 2008.
9. Oliveira AP, Gomes AMT. A estrutura representacional do câncer para os seus portadores: desvelando seus sentidos e dimensões. Rev enferm UERJ. 2008; 16:525-11
10. Oliveira DC. Pontuando ideias sobre o desenvolvimento metodológico das representações sociais nas pesquisas brasileiras. Rev Bras Enferm. 2004; 57:508-11.
11. Bardin L. Análise de conteúdo. Tradução de Luis Antero Reto e Augusto Pinheiro. São
Paulo: Edições 70; 2010.
12. Spink MJP. Psicologia social e saúde: práticas, saberes e sentidos. Petrópolis (RJ): Vozes; 2007.
13. Moscovici S. A psicanálise, sua imagem e seu público. Petrópolis (RJ): Vozes; 2012
14. Queiroz, ABA, Arruda A. Refletindo sobre a saúde reprodutiva e a situação de infertilidade. Cad Saúde Coletiva. 2006; 14: 163-78.
15. Tedeschi LA. Relações de gênero e a história das mulheres camponesas. Educação, Ciência e Cultura. 2009; 14: 45-62
16. Zanin M, Moss AT, Oliveira LA. Representação social da gravidez na percepção de adolescentes gestantes de baixa renda. Unoesc & Ciência – ACHS. 2011;2: 89-98
17. Hisada S. O processo de adoecer. In: Tedesco JJA, Cury AF. Ginecologia psicossomática. São Paulo: Atheneu; 2007. p. 7-9.
18. Alves PC, Minayo MCS. Saúde e doença: um olhar antropológico. Rio de Janeiro: Fiocruz; 2008.
19. Silva SED, Vasconcelos EV, Santana ME, Rodrigues ILA, Mar DF, Carvalho FL. Esse tal Nicolau: representações sociais de mulheres sobre o exame preventivo do câncer cérvico-uterino. Rev esc enferm USP. 2010; 44: 554-60.
20. Insa LL, Mónleon AB, Espallargas AP. El enfermo de cáncer: una aproximación a su representación social. Psicologia e Sociedade. 2010; 22:318-27.
21. Vieira CP, Queiroz MS. Representações sociais sobre o câncer feminino: vivência e atuação profissional. Psiclogia e Sociedade. 2007, 18:63-70.
22 .Alverez REC, Moncada MJA, Arias GG, Rojas TCS, Contreras MVI. Rescatando autocuidado de la salud durante el embrazo, el parto y al recién nacido: representaciones sociales de mujeres de una comunidad nativa en Perú. Texto contexto - enferm. 2007; 16: 680-7.
23. Kenny S, Camargo BV, Bertoldo RB. Percepção da imagem corporal e representações sociais do corpo. Psic: Teor e Pesq. 2009; 25: 229-36
24. Trindade WR, Ferreira MA. Grupo feminino de cuidado: estratégia de pesquisa: cuidado à mulher. Rev Bras Enferm. 2009; 62:374-80.
25. Abric JC. A zona muda das representações sociais. In: Oliveira DC, Campos PHF, organizadores. Representações sociais, uma teoria sem fronteiras. Rio de Janeiro: Museu da República; 2005.p.23-4