RESEARCH ARTICLES
Nursing in a hematopoietic stem cell transplant unit: profile and self-care
Sandra Hilda SobrinhoI; Vera RadünzII; Luciana Martins da RosaIII
INurse. Master degree in Nursing. Coordinator Nurse of the Bone Marrow Transplantation Unit of the Oncology Research Centre. Health State Secretary of Santa Catarina. Member of the Research Group Caring & Conforting. Florianópolis, Santa Catarina, Brazil. E-mail: sandrahilda@hotmail.com.
IINurse. PhD in Nursing. Professor of the Nursing Department and Post-graduation Program in Nursing of the Federal University of Santa Catarina. Leader of the Research Group Caring & Conforting. Florianópolis, Santa Catarina, Brazil. E-mail: radunz@ccs.ufsc.br.
IIINurse. PhD in Nursing. Professor of the Nursing Department of the Federal University of Santa Catarina. Member of the Research Group Caring & Conforting. Florianópolis, Santa Catarina, Brazil. E-mail: luciana.m.rosa@ufsc.br.
ABSTRACT: This quantitative descriptive study aimed to identify the profile of nursing professionals working in a hematopoietic stem cell transplantation unit, and the strategies used for self-care, drawing theoretically on the assumptions of Radünz with regard to self-care and on World Health Organization, Buss, Heidemann, Verdi and Caponi concepts of health promotion. Data were collected from August to October 2010 by applying a questionnaire of open and closed questions to 18 subjects in Santa Catarina, Brazil. The results highlighted women’s work, working hours in excess of 30 hours weekly and higher education as well as self-care strategies, including being with family and friends, physical exercise, good relationships at work, healthy diet, sleep and rest. The findings indicate the need for institutions to adjust to favor the well-being of personnel at work and for the broader use of the health promotion approach by nursing professionals.
Keywords: Nursing; medical oncology; health promotion; hematopoietic stem cell
INTRODUCTION
Work is an important component in the people´s lives, not only for survive. It enables the social insertion and contributes with the definition of individual´s self-identity1.
The specialized works demand continuous training and acting with ability. The professional exercise of nursing in the hospital area is one of these services presenting diverse demand. In health care of high complexity, in a transplant unit of hematopoietic stem cells (TUHS), nursing care, beyond the requirements of care to cancer clients and their families, it is full of different situations of conflicts and decisions. In addition, there are different demands of a big number of complex procedures and equipment requiring a constant technical-scientific improvement of the team2-4.
In this context, there is the suffering of the oncology client and his Family, demanding a constant control by the nursing professional. For this, it is necessary the professional having knowledge and abilities to deal with their own feelings and to develop action to avoid physical and emotional wearing. Anyway, the professional needs to learn how to care himself to promote health.
In this way, there is the necessity of increasing studies in oncology area, to understand the profile of the nursing professional caring of himself and the other, developing strategies to balance self-care and the care for others, to avoid physical and emotional wearing giving an effective care5-7.
Thus, the objective of this study was to identify the nursing professional profile who works in the TUHS unit in the state of Santa Catarina and the self-care actions that this nursing team performed individually to promote health.
THEORETICAL REFERENCE
For the development and theoretical maintenance of this study, we chose to use the philosophical assumptions and theoretical conceptions of Radünz about self-care, established in his doctoral thesis entitled - A philosophy for nurses: self-care, living with the finitude and the preventability of Burnout. For the author, self-care refers to the promotion of health and it is linked to the process of living and being healthy, i.e., it covers all aspects of person´s life, where the individual takes responsibility for his health by the style of life he chose5.
The author lists strategies that nurses can use to self-care as consultations and periodic examinations, healthy habits, exercise practice, sleep, rest and feeding with frequency and quality, social support, psychological, spiritual and leisure. Noting that the person is the responsible for healthy attitudes and behaviors, and this is an ethical commitment hemselves and others, leading to health promotion5.
For additional support, we associated Radünz5 proposal with concepts of health promotion8-11, summarized here.
In these concepts, health promotion is defined as a process to enable the empowerment of individuals and communities to act actively in search of better quality of life and health11. It is focused on a positive concept and involves the physical, political, social, cultural environment, public policies and conditions that actually promote health development9-11.
Thus, given the above, we understand that seeking to know who are the nurses who work in the TUHS unit favors the planning of the work process, social exchanges and health education.
We believe that dialogue about self-care from data analyzed is a strategy to promote health of professionals and we stressed that the promotion of health in a broader approach favoring some fields of action, such as creating supportive environments and developing skills personal involving greater participation of individuals, thus disregarding the model that discriminates subjects and blames, blaming them for their own health11.
METHODOLOGY
It is a descriptive research, with quantitative approach, performed in an institution specialized in oncology care in Santa Catarina, Brazil.
The study scenario is a care unit of high complexity in oncology, reference in Santa Catarina State, Brazil, acting in TUHS since 1999. The nursing staff of this unit are 27 professionals, 10 nurses and 17 nursing technicians. In this study 18 nursing professionals participated, 10 nurses and 8 nursing technicians.
The study was approved by the Ethic Committee in Research of the institution studied, under opinion set out number 009/2010. Its development followed the established requirements by Resolution number 196/96 of the Health National Council (HNC)12.
The inclusion criteria of the study participants was filling out the identification form and the interest shown by the professionals participating on the research, registered signing the Informed Consent Form (ICF).
Before starting the data collection, there was a meeting with the nursing professionals to present the Project, highlighting the theoretical references by Radünz5 and the concepts about health promotion8-11, as an education strategy. This stage was in August 2010.
For the data collection, each research participant was asked to fill out the individual identification form (questionnaire). This form had closed questions investigating social and work data, as: age, gender, education, workplace, workload and an opened question about the self-care actions performed and considered significant for the health promotion.
The forms were delivered after the project´s presentation. For the professionals who were not in the presentation day, the form was given later, as well as the clarifications needed about the project and the ICF. The The return of the forms was accepted until October, asking them to put the forms in an envelope with the name of the research, in the mural of the nursing center in the unit. The forms were daily collected by the researchers, after the morning and afternoon shift changing from Monday to Friday.
The data presented in this study are quantitative, so they did not need coded identification of the subjects to their anonymity.
The collected data were typed in Microsoft Excel program worksheets and then processed and analyzed by descriptive statistic. The results related to self-care were analyzed according to the theoretical references proposal supporting the study development.
RESULTS AND DISCUSSION
Regarding to gender, the female workforce prevailed, 17 professionals (94%) and 1 (6%) male professional. This finding is similar to other studies shown feminization in the profession, being 94.1% of nursing staff. Nursing is a historically women profession, aimed the human being, family and society care, experiencing health/disease process13,14.
Regarding the working time in the OMT unit, 6 subjects (33.3%) work less than 3 years in the institution, 4 (22.2%) work since 5 years ago and 8 (44.4%) have more than 10 years of work. These results demonstrate that the number of individuals with more working time and stability gained by the time worked at the institution prevails.
The professional experience, the institutional involvement and the stability gained by the time worked, make the professionals to stay in the organization, being even associated to these factors the work proposal the institution offer and the own individual satisfaction15.
As for the double employment, only 5 (28%) of the subjects have other job, while 13 (72%) have exclusive dedication to the study scenario. This result is similar to other study15, showing that 66% of the nursing staff has exclusive dedication to one job and this is a factor enabling the nursing professional a higher involvement with the institution and his job. Different from this reality, another transversal study investigating the health of 502 nursing professionals of a public hospital in Bahia, showed that the double employment was in 53.9% of the studied population, revealing a high demand of workload in nursing16. The double shift at work affects the nursing worker health, having poor time to self-care due to the increase of workload, affecting his quality of life17.
Most of the professionals here investigated, do not have double employment. However, 5 of them (28%) work 24 extra hours a month, 3 (16%) work 36 extra hours, 5 (28%) 60 extra hours and 5 (28%) do not have extra hours. The number of employees in the 24 hour schedule and low salaries justify the high number of extra hours by the nursing staff.
In this way, professionals try to increase these low salaries working extra hours.
On the other hand, public system give the opportunity to do extra hours, because the payment of these extra hours is much less hiring more people according to technical indications, related to care demand.
In a study about nursing working management, it is shown that this situation occur very often due to the need of ensuring the continuous nursing assistance and highlights that the excess of worked hours can cause technical mistakes involving the patient´s security and worker´s health. This same study suggests as a strategy the compensatory day off, highlighting the importance of the worker to enjoy at least one day off a month on Sundays or holidays, so they can be together with their family and friends, strengthening affective and social bonds18.
Many professionals are obligated to increase their workload because of their low salaries in health area, not enough to support them and the family. This problem interfere in the time that the nursing professional takes to self-care and leisure, interfering in some aspects like quality of life, increasing tiredness and consequently, generating physical and emotional stress17,19,20.
Some components add up to the need to double or triple workload and are known as threatening to the nursing work environment. The lack of health professionals, the excess of activities, the lack of autonomy, the professional recognition and the poor salaries worsen then professional situation20.
The nursing care practice demands nonstop 24 hours a day service. Thus, analyzing the results of this study, it is recommended to do breaks every 12 hours shift (period of the shifts adopter by the TUHS here investigated) not exciding that period to preserve professional health and patient´s security, according to legal requirements.
The workload from 30 hours a week is the healthiest indication, enabling the dedication to work, self-caring and the family, promoting health and ensuring the availability of time for technical and scientific improvement. But this workload must be linked to a dignified salary, being something for professionals and health institutions to struggle. The managers should be aware, despite being common the rest period occurring during the week, it is important that professionals enjoy moments of self-caring on Sundays and holidays with family and friends, strengthening the emotional and social bonds, contributing to health care and intellect by creating an environment of humanized care.
Regarding to age, the results show that 1 subject (6%) is 20 to 25 years old, 7 (39%) are 25 to 35 years old, 8 (44%) are 35-45 years old and 2 (11%) are 45-55 years old. Then, the majority, 16 (83%) are 25 to 45 years old. These data are different from another study on the employability of nurses in Brazil, showing that, of 565 nurses, 64.3% were 35-55 years old21.
As for the academic education, 6 subjects (33%) have completed basic education; 2 (11%), completed graduation and 7 (39%), completed post-graduation. In addition, 3 subjects (17%) are attending post-graduation school, of which 2 (11%) are attending Oncology Nursing Course and 1 (6%) Master degree course. These results do not allow us to affirm that nursing professionals of the unit invest in their professional training.
A Brazilian study shows that specialization in graduation nursing appears in 31.2% of the population of the study21, equivalent to the findings in this study. However, in the study scenario there is no policy to encourage training and vocational training. The results represent the interests of professionals in their own professional development.
The nursing staff of the study scenario works with two types of labor contracts, a 40-hour week contract by CLT regime and another 30 hours a week contract by the statutory regime of the State Secretary, 5 subjects (28%) have 40 hours per week contract and 13 (72%) have 30 hours per week contract. The most frequent complaint of professionals who have the contract of 40 hours is to work longer hours and have less pay and less labor advantages, when compared to the same category of professionals hired by the statutory regime.
Different regime work in the same professional category can create conflicts in the workplace. The stressful work done by oncology nurses indicates the need for maximum workload of 30 hours per week. This situation was found in only 1 subject investigated (6%). The other 17 (94%) work more than 30 hours, only in the scenario of the study or in other health institutions.
The managers should be aware that, despite being common the rest period occurs during the week, it is important that professionals enjoy moments of self-caring on Sundays and holidays with family and friends, strengthening the affective and social bonds, contributing to the health care and intellect by creating an environment of humanized care.
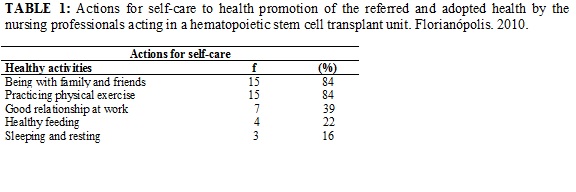
As for the actions of self-caring for health promotion, there were highlighted the needs to be with the family and the practice of physical exercises, adopted by 15 study subjects (84%), as shown in Table 1.
The findings are similar with the study, according to which the nursing staff that cares for cancer patients, uses different activities to promote his own care, including support from being with family and friends and creating a therapeutic environment at work as important strategies to promote health5. See Table 1.
According to the concepts about health promotion supporting this study, health starts to be built for the care that each one dedicated to himself and others, by the ability to make decisions and have control over the circumstances of their lives and the struggle for society to provide conditions that allow having health by all its members8.
The idea of health promotion, rescuing the prospect of linking health and living conditions, highlights the multiple as physical, psychological and social elements linked to achievement of a healthy lifestyle, highlighting the importance of both the development of collective participation and skill individual. Ways of life, work and leisure are health sources contributing to create a healthier society and promoting health means to watch some fields of action as healthy public policy, supportive environments, strengthening community action and the development of skills and attitudes conducive to health11. Health should be seen as a resource for everyday life, not the objective of living, resulting care that each person dispensing herself and others. Therefore, health is a positive concept emphasizing social and personal resources, as well as physical capacities. Developing strategies for health promotion means advocating on multiple political, economic, social, cultural, environmental, behavioral and biological factors8.
Analyzing the social, labor characteristics and actions of self-care, it can be stated that, despite the effort to supplement the salary and maintain shift coverage, the subjects are concerned with maintaining health activities, prioritizing social contact with family and friends and to do exercise, thus searching for leisure time, breaking the routine of nursing, creating moments to self-care.
In nursing, self-care and taking care of another promote growth, improvement and development of the caregiver and who is cared. To develop the praxis of human care there are principles such as self-knowledge and self-care. When the nursing professional makes use of these possibilities, he adopts ethical behavior for life, awakening the responsibility and concern for the living. Healthy lifestyle habits, such as exercising, sleeping, resting and frequent and quality feeding, social, psychological and spiritual support and leisure are healthy attitudes and behaviors that elevate the quality of life and promote health5.
CONCLUSION
With these findings, it is identified that the profile of the participants sows the prevalence of female gender, higher education, the unique professional bond with the study scenario, as well as excess worked hours.
The physical activity and being with family and friends were the most cares cited followed by the good working relationship, care with feeding, sleeping and resting. These findings demonstrate the significance of interpersonal and emotional relationships for the good life, as a practice of care and of life and care for the body to support life and the pursuit of the harmonious balance of organic and mental functions.
On the other hand, the findings showed that the practices of self-care do not cover all aspects of health promotion. Thus, it is necessary for professionals to expand their vision of health promotion, including as critical actors and participants in this process. In this study, the time available for such practice was limited, unable more comprehensive and consolidated results in the individuality of each subject.
The reflective practice on self-care for health promotion helps the construction of new knowledge and contribute to improving the quality of life of nursing staff, enabling the provision of a humanized nursing care.
It is recommended that the study scenario creates internal policy to promote training, capacity building and professional improvement. One way to facilitate these projects is through the design and quantitative adequacy of the nursing professionals, adding an index of technical security to cover situations related to staff turnover and participation in continuing education programs, fitting to technical indications.
Another important practice to encourage health promotion would be encouraging good relationships in the workplace, because it is a prerequisite for collaboration and mutual support encourages understanding, tolerance and spirit of helpfulness among professionals. Thus, labor institutions should permanently exploit this practice.
Considering cancer as a public health problem, it is necessary continued exploitation of the nursing staff to self-care, since working to promote health to self-care and vice versa is an important issue to relevance in the tertiary care of high complexity and in any other practice area of nursing professionals.
REFERENCES
1. Carvalho V. Sobre a identidade profissional na Enfermagem: reconsiderações pontuais em visão filosófica. Rev. bras. enferm [Internet] 2013 [citado em 12 mai 2014]. 66(spe):24-32. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0034-71672013000700003&lng=en.
2.Bonassa EMA, Gato MIR. Enfermagem em terapêutica oncológica. 4ª ed. São Paulo: Atheneu; 2012.
3. Machado MH, Vieira ALS, Oliveira E. Construindo o perfil da enfermagem. Enfermagem em Foco. 2012; 3(3):119-22.
4. Avellar LZ, Iglesias A, Valverde PF. Sofrimento psíquico em trabalhadores de enfermagem de uma unidade de oncologia.Psicol estud. 2007; 12:475-81.
5. Radünz V. Uma filosofia para enfermeiros: o cuidar de si, a convivência com a finitude e a evitabilidade de Burnout. Florianópolis (SC): UFSC; 2001.
6. Santos VEP. O cuidar de si no contexto acadêmico da enfermagem e a segurança do paciente [tese de doutorado]. Florianópolis (SC): Universidade Federal de Santa Catarina; 2009.
7. Silva IJ, Oliveira MFV, Silva SED, Polaro SHI, Radunz V, Santos EKA et al. Cuidado, autocuidado e cuidado de si: uma compreensão paradigmática para o cuidado de enfermagem.Rev Esc Enferm USP. 2009;43:697-703.
8. World Health Organization. The Ottawa charter for health promotion. Ottawa (Ca): WHO; 1986.
9. Buss PM. Promoção da saúde e qualidade de vida. Ciênc. saúde coletiva. 2000; 5:163-77.
10. Heidemann ITSB, Almeida MCP, Boehs AE, Wosny AM, Monticelli M. Promoção à saúde: trajetória histórica de suas concepções. Texto Contexto Enferm. 2006;15:352-8.
11. Verdi M, Caponi S. Reflexões sobre a promoção da saúde numa perspectiva bioética. Texto Contexto Enferm. 2005;14:82-8.
12. Ministério da Saúde (Br). Conselho Nacional de Saúde. Resolução nº 196/96 de 10 de outubro de 1996. Aprova as diretrizes e normas regulamentadoras de pesquisas envolvendo seres humanos. Brasília (DF): CNS; 1996.
13. Lopes MJM, Leal SMC. A feminização persistente na qualificação profissional da enfermagem brasileira. Cadernos Pagu. 2005; 24:105-25.
14. Amorim RC. A questão do gênero no ensinar em enfermagem. Rev enferm UERJ. 2009; 17:64-8.
15. Martins C, Kobayashi RM, Ayoub AC, Leite MMJ. Perfil do enfermeiro e necessidades de desenvolvimento de competência profissional. Texto Contexto Enferm. 2006;15:472-8.
16. Araujo TM, Aquino E, Menezes G, Santos CO, Aguiar L. Aspectos psicossociais do trabalho e distúrbios psíquicos entre trabalhadoras de enfermagem.Rev. Saúde Pública. 2003; 37:424-33.
17. Pafaro RC, De Martino MMF. Estudo do estresse do enfermeiro com dupla jornada de trabalho em um hospital de oncologia pediátrica de Campinas.Rev Esc Enferm USP. 2004; 38:152-60.
18. Freitas GF, Fugulin FMT, Fernandes MFP. A regulação das relações de trabalho e o gerenciamento de recursos humanos em enfermagem.Rev esc enferm USP. 2006; 40:434-38.
19. Harbs TC, Rodrigues ST, Quadros VAS. Estresse da equipe de enfermagem em um centro de urgência e emergência. Boletim Enferm. 2008; 2 (1):41-56.
20. Murofuse NT, Abranches SS, Napoleão AA. Reflexões sobre estresse e Burnout e a relação com a enfermagem. Rev Latino-Am Enferm. 2005;13:255-61.
21. Universidade do Estado do Rio de Janeiro. Empregabilidade e trabalho dos enfermeiros do Brasil. Relatório final. Rio de Janeiro: Instituto de Medicina Social; 2006.