RESEARCH ARTICLES
Individual and clinical characteristics of clients with chronic kidney disease on renal replacement therapy
Brunno Lessa Saldanha XavierI; Iraci dos SantosII; Renato Francisco AlmeidaIII; Araci Carmen ClosIV; Monique Tavares dos SantosV
INurse, PhD student in Nursing from the State University of Rio de Janeiro, Assistant Professor of the Graduate Nursing Program at the Federal Fluminense University, Rio das Ostras, Rio de Janeiro, Brazil, Email: brunnoprof@yahoo.com.br.ABSTRACT: This paper aims at identifying individual and clinical characteristics of people with Chronic Kidney Disease (CKD) on hemodialysis, awaiting kidney transplant. Descriptive and quantitative methods held at Rio de Janeiro-Brazil, with 48 clients, from October to November, 2013, applying structured interview during nursing consultation. Data were treated with standard descriptive statistics. Results show 58.3% are female; 62. 5% are black; 58.3% have primary education levels, and 67% have family income of 1-2 minimum wages. Average age was 49 years old; 71% were dependent on hemodialysis for longer than two years; and 66.7% take it as their only treatment option. Hypertension and major comorbidity affect 85.4% of the subjects investigated. Conclusions show that there are worrying socio demographic and clinical conditions, suggesting preventive interventions to minimize morbidity and to promote quality of life through nursing guidance for self-care of clients with CKD.
Keywords: Nursing; self-care; chronic kidney disease; hemodialysis.
INTRODUCTION
Chronic kidney disease (CKD) represents an object of great importance and concern in the field of public health, due to its high morbidity and mortality.
In recent decades, specific hygiene measures such as the control and eradication of major epidemics, sanitation, the advancement of antibiotic therapy and chemotherapy resulted in a sharp reduction in mortality from infectious and parasitic diseases, contributing to the increase in life expectancy and an aging population. Simultaneously, chronic degenerative diseases have assumed a prominent position in the healthcare scenario in general, seen changes in life habits, in particular, the progressive increase in industrialization and urbanization1.
In this aspect, surpasses that the incidence of CKD is progressively increasing in the population, constituting a concerning public health problem in Brazil. According to the last census in 2011, there are 91,314 clients in dialysis treatment in Brazil. In the year of 2000, there were 42,695 people undergoing this type of treatment. Therefore, the total number of people in renal replacement therapy more than doubled in 11 years. In addition, among more than 90,000 individuals in dialytic therapy currently in the country, approximately 90% are dependent on hemodialysis2.
This pathology, in conjunction with the inevitability of a rigorous treatment, breaks out a succession of situations for the client, compromising the physical and psychological aspects, and reverberates in personal, family and social spheres3. Regarding the aspect of living with this individual, there is an urgent need for nursing interventions, prioritizing more innovative alternatives to the limitations caused by the disease and the treatment, being necessary to relearn to live the life that they have with the essential human dignity.
Stressing that the challenge configured in the caring for the individual with CKD undergoing renal replacement therapy (RRT), is also characterized by care to the complexity of their normally present clinical and emotional condition.t. This alerts for an urgent need for construction and appropriation of new knowledge, aiming to guide alternate paths, based on the care needs of the person relating to the promotion of the their welfare3.
In view of these facts about the characteristics of CKD and modalities of renal replacement, inclusive, whereas the human needs and of guidance for self-care for clients affected by this, presents the research problem: what are the individual characteristics and conditions for people affected by chronic kidney disease, and hemodialysis therapy, awaiting a kidney transplant?
This study aims to identify the individual and clinical characteristics of people with chronic kidney disease on dialysis and awaiting a kidney transplant.
LITERATURE REVIEW
CKD is the progressive and irreversible loss of renal capacity to maintain its normal functions, causing systemic signs and symptoms. Its cause is mainly due to the progression of diseases such as diabetes mellitus, hypertension, and glomerulonephritis, or also repeated urinary tract infections4.
Together with the progressive decline of the glomerular filtration rate (GFR) detected in CKD, it is observed that the deterioration of regulatory, excretory and endocrine functions of the kidney, thus compromising all other organs and body systems4,5.
The first symptoms of CKD may take years to emerge, and this fact may be decisive for the characteristics of the clinical course of the disease5. However, with early diagnosis of the disease in conjunction with the introduction of specific interventions and care, one can slow its progression thus avoiding some of its feared complications3,5.
The renal function replacement treatment modalities, called renal replacement therapies, include hemodialysis, peritoneal dialysis and kidney transplant3. All these alternatives employ advanced technologies, involving monitoring by health professionals with mandatory frequency and high costs6.
In addition to the RRT, conservative treatment is mentioned consisting mainly on dietary control, blood pressure and underlying diseases, and even in the continuous use of medication. It outweighs that such treatment modality is anchored in an attempt to halt the progression of the disease, aiming mainly to delay the need for submission to a form of therapy in order to greatly reduce the suffering of the clients6.
METHODOLOGY
To develop this research, it was decided to carry out an analytical-descriptive investigation, with a quantitative approach, characterizing an epidemiological study of people with CKD.
The research was performed in the hemodialysis unit of a general hospital in large, private, and located in a central area of the city of Campos Goytacazes-Rio de Janeiro-Brazil. In this unit, in addition to the dialysis treatment offered in the peritoneal dialysis and hemodialysis modalities, there is the care / outpatient monitoring of patients in treatment and/or being tested for CKD. It outweighs the presence of a multidisciplinary team of nurses, nutritionist, psychologist and social worker.
The study subjects were 48 clients with a definitive CKD diagnosis, duly registered in regular hemodialysis programs and waiting for the call for a kidney transplant, from their registration on the waiting list to receive a kidney.
For the sample selection, was, initially, a survey of all those regularly seen in the service at the dialysis hospital, based on the analysis of medical records, seeking to meet a priori to the following criteria: duration of hemodialysis equal to or less than eight years and with an active registration on the waiting list for a transplant.
The following inclusion criteria have been established: to have CKD of any etiology and in a regular hemodialysis regimen, in addition to wanting to receive the kidney transplant; be capable of cognition / understanding preserved; both sexes and over 18 years of age; and own a phone or email contact for possible communication about the research and be able to sign the Informed Consent Form (ICF).
Exclusion criteria were less than 18 years of age, clients who refused to sign the Informed Consent Form (ICF) and/or who had some type of cognitive deficit, because this factor prevents the interpersonal communication and the application of the data production form.
Among the 156 clients who were registered and being treated in the study field, only 48 fulfilled the criteria proposed for the composition of the sample.
The data production was carried out by the researchers, through the nursing consultation, in the months of October and November 2013, directly with individuals with CKD in RRT, during the hemodialysis sessions that happen three times a week. The choice of approach with the client, is at the time they are connected to the hemodialysis machine, this is justified because it is a period in which, generally they are at idle for an average of four hours. It is, therefore, a unique opportunity to fill this time with some activity.
The data collection took place from the application of a structured form, prepared for project implementation of the doctoral thesis in nursing through clinical trial, aiming at the identification of the socio-demographic characteristics and clinical users with CKD in the health system.
The form used in the data production considered the following variables, related to socio-demographic characteristics: gender, color/ethnicity declared, age, place of birth, residence, type of residence, level of education, profession/occupation, state of the union, family circle, family income, religious belief; and those related to clinical characteristics, i.e. , associated with living with the disease: discovery time and knowledge about the disease and the cause(s), comorbidities, medical treatment recommended, time of hemodialysis and living with treatment, history of kidney transplant, knowledge about CKD treatment modalities and the care needed for coexistence.
The data obtained were organized, grouped and tabulated. A simple descriptive statistics was applied, calculating the absolute frequency and percentage. This data is presented in simple tables, and in one of them, there is a relationship between the study variables.
It is noteworthy that the application form, taken with an average duration of 20 minutes for each participant it occurred after the client's signature on the consent form, in accordance with Resolution No. 466/2012, concerning research with humans. As well, have been complied with the principles of autonomy, beneficence, non-maleficence, justice and equity, and the study submitted to the evaluation of the Research Ethics Committee at the University of the State of Rio de Janeiro, obtaining approval by the opinion no. 407.889 /2013.
RESULTS AND DISCUSSION
This session begins by describing the individual characteristics of the study subjects. Of the total of 48 clients with CKD undergoing regular hemodialysis treatment, selected to compose the study in this research scenario, it is noted that the most, 28 (58.3%) were female, and 20 (41.7 %) were male.
In spite of the chronic kidney disease reach, without distinction, men and women, the division of the sample in terms of gender, in this research, draws attention to counterbalance the several studies7,8 already carried out on the same subject, which, generally, display in their majority a male clientele.
The average age of the sample was 49 years, with a range between 20 and 68 years, with predominance of 50% in the age group between 51 to 68 years. It outweighs that 8 (16.7%) respondents were aged between 20 and 38 years, and 6 (75%) of these were women, all married and/or divorced and without occupation and/or remunerated activity. It was also found that 16 (33.3%) clients aged between 40 and 50 years.
The predominance of the respondents in the age group above 51 years corroborates with the study that showed a greater number of individuals with more advanced age on hemodialysis treatment, due to the high prevalence, in this clientele, of diseases such as hypertension and type 2 diabetes mellitus9.
It was noticed that the majority, 30 (62.5%) individuals, were ethnically self-declared as black. It is also emphasized that 19 (39.6 %) participants didn't even complete elementary school and 28 (58.3%) were, at the time, single and/or without a steady companion.
Regarding the people's state of union, this research revealed the predominance of unmarried individuals and/or without a steady companion. Thus, it also says that, generally, a solid family support associated with a healthy relationship with a partner and/or friends, favors the coping with the disease and its treatment, minimizing losses and frustrations imposed by the new routine10 and coexistence with the CKD and in RRT.
It was found that the majority of the 48 interviewees, corresponding to 26 (54.2%) clients, was composed of Catholics, while 10 (21%) individuals were evangelical. The family income level of one to two minimum wages was predominantly informed by 32 (67%) clients. It is noteworthy that 8 (16.7%) participants chose not to disclose their income.
In this research, it was found that only 3 (6.2%) respondents had, at the time, some occupation and/or remunerated activity, while the majority, 30 (62.5%), was retired and/or a pensioner, and 15 (31.3%) were unemployed and/or without fixed income. On this last point, it should be noted that of this total, 12 (80%) were women, less than 51 years of age.
The fact that few clients exercised a profession and / or remunerated activity, corroborates with findings of previous studies9,11. As for the females, they are unemployed and/or without fixed income, it should be noted that these are less than 51 years of age, therefore, are productive. This observation suggests an exclusion character of this type in the labor market.
Work for citizens is an important trace of their existence, allowing their professional self-realization, as well as financial autonomy for the support of the family institution, especially for adults. Therefore, it outweighs that CKD and its treatment do not characterize direct and absolute impediment to work. However, it causes some significant limitations for people, often resulting in undesirable gaps and/or early retirements12.
The clients that have ties with work are generally more independent and have greater self-esteem and self-actualization, and thus show greater satisfaction with living and support from friends and family. On the other hand, those who are not able to establish and/or maintain ties with work, tend experience feeling of frustration, powerlessness and dependence, favoring a hopeless state of dissatisfaction with the time and support they receive from people close to them12,13.
Among all the aspects previously seen so far, it is noteworthy that the majority of respondents had low level of schooling, still revealing the fact that the total sample, only two individuals, male, were able to complete higher education. As we live in a capitalist society, with an increasingly competitive labor market, low education makes it difficult for this clientele to even enter and / or stay in the labor market.
Even in terms of the correlation between the level of knowledge of the respondents and the degree of schooling, it is important to highlight the lowest degree of schooling of 21 subjects among the 32 who reported ignoring other RRT possibilities in addition to hemodialysis. On this aspect, it reflects about the preponderance of social and cultural metrics, to which the citizen fulfils conditions to achieve and assimilate knowledge and additional information for their survival process.
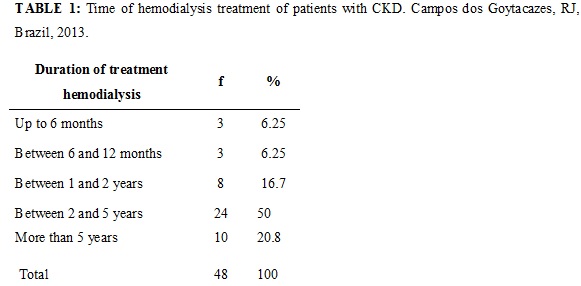
It highlights the dependence of hemodialysis prevalent up to five years in this study, as shown in Table 1. It outweighs some studies showing that the more time spent in dialysis, the more resignation to the disease is perceived14. However, parallel to this, there are studies that have found that the longer one stays on hemodialysis, the greater will be the range of strategies developed by clients to deal with the disease and its treatment14,15.
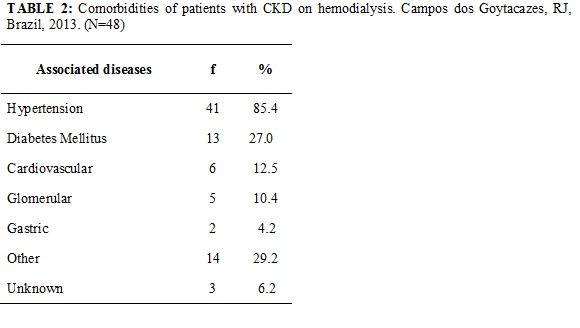
It should be noted that the results obtained on comorbidities /associated diseases reinforce information2 and research11,16 already disclosed about the theme, where it was found that hypertension and diabetes appeared leading the list of pathologies associated with CKD, according to Table 2.
The majority of respondents attributed their illness to hypertension and/or diabetes It is known that these two diseases, especially when they are not controlled, are considered, in actuality, the greatest villains in terms of the onset and progression of CKD. These diseases, when not treated and controlled appropriately, in different ways trigger, a slow progressive degeneration process of the organs and targets tissues, including the kidneys. Thus, with the passage of time, the development of irreversible loss of partial and / or total function of the organ arises from an inexorable event17.
Also with respect the conception of subjects about what might have caused the disease, it was found that some participants made analogies and / or conclusions with anemia (three interviewees), with habits such as too much sun exposure (2 respondents) and work several consecutive days at nighttime. There was no one who didn't relate to the question of their CKD.
There is evidence that anemia is one of the complications of the disease and not its cause4. Triggered mainly by the decrease of erythropoietin, the disorder is characterized by fatigue, cooling of cognitive function, depression and shortness of breath, among other symptoms. Approximately 75% of clients with CKD and almost all children develop anemia4.
Although rare, there are records of cases of serious diseases brought on by heat, even in populations with a low risk (in good physical shape, who already live in regions where the climate is hot, or that work in places with high temperatures). Caused by heat, the injury is configured in an event that can be moderate to severe, characterized by impairment to an organ (e.g. liver, kidney, intestines) and usually, but not always, with a body temperature above 40° C18.
Still, of all the participants who said that they know the different ways to treat the disease, the majority did not mention kidney transplant. On this aspect, it is important to stress the fact that the imagination of clients with CKD, often, the transplant is seen as cure and/or final resolution of the problem, and not as a modality/option to deal with the disease6.
Something to consider, is the fact that customers have reported that were caught by surprise when they initiated a RRT. CKD is often diagnosed at an advanced stageby not displaying significant symptoms in its early stages4. This has forced clients to initiate an RRT, almost always the hemodialysis11, suddenly, without proper time and condition to meet and choose the treatment modality that seem the more convenient and / or appropriate for them.
Regarding the duration of hemodialysis, as already shown in Table 1, it is noted that half of the 48 study participants were already machine-dependent for between two and five years. It is also clear that 10 (20.8%) of the total number of clients have depended on dialysis for a period longer than five years.
It was observed in this study, the average time between the discovery of the disease and the onset of dialysis therapy of the client, highlighting that the majority of respondents, 32 clients (66.7%) started hemodialysis treatment within six months after the discovery of CKD, as shown in Table 3.
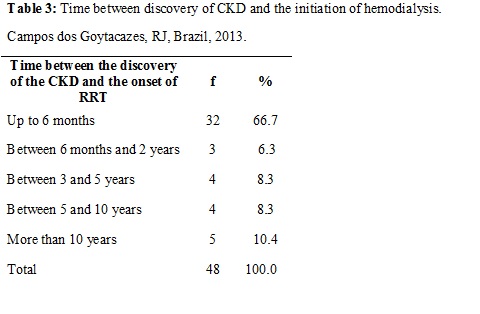
According to this aspect, it drew attention to the fact that 24 (75%) respondents, of all 32 who began to dialyze 32 during the first six months after the discovery of the CKD, they began early during the first 60 days.
Analyzing information about the comorbidities associated with the table of CKD, referred to by the respondents, there was hypertension raging almost the entire sample Research 41 (85.4%), followed by Diabetes Mellitus - 13 (27%). In the meantime, it should be noted that 11 (23%) clients revealed association of both pathologies. The associated diseases, in this study are described in Table 2.
Regarding the responses of other clients classified as in Table 3; there are three who show association with thyroid disorders cases, three with retinopathy, two cases of Human Immunodeficiency Virus (HIV) and one with Hepatitis C.
There was the perception of each client concerned about the relation x disease, i.e., their conception of the triggering factor for CKD in their body. Thus, it was found that 29 (60.5%) attributed the onset of their renal pathology to hypertension and/or diabetes.
Regarding the level of knowledge of the subjects on the options / possibilities of treatment of CKD, it is observed that 32 (66.7%) reported not knowing all the available treatment modalities.
By correlating the knowledge on RRT with the level of education, it outweighs that 21 (43.7%) respondents with elementary school reported no knowledge of another RRT beyond hemodialysis. Compared with the individuals with high school, this rate drops to 11 (22.9%).
IT outweighs that 16 (33.3 %) clients said they knew all replacement therapies in renal function, although none of them have correctly mentioned all the possibilities for treatment Apart from hemodialysis, they made mention only peritoneal dialysis. Among all respondents, only 4 (8.3%) participants described the transplant as a treatment option, however, they did not mention all dialysis modalities offered to deal with CKD.
A limitation of the study relates to the fact that it is an excerpt from a doctoral thesis in progress, whose aim is to characterize the study subjects. Therefore, the correlation between clinical variables and the results on the self-care behavior of clients living with CKD, which are evident, will be the subject of a future study.
CONCLUSION
The results concerning the socio-demographic and clinical characterization of customers with CKD on dialysis, and waiting for kidney transplantation, revealed, a priori, that the disease in question has been ruining, so indistinct, men and women, in the age range increasingly low, that is, a phase of life in which the citizen is considered active and productive. This evidence warns that the chronic degenerative disorders, such as the CKD, is manifested in the general population of ever more early.
It is also highlighted poor education and lack of employment relationship and / or remunerated activity of the majority of the subjects investigated. Because it is undeniable that CKD and its treatment, especially hemodialysis, lead to individual limitations in the spectrum of daily and / or routine activities. Nevertheless, this should not constitute a direct impediment to the development of various activities, including remunerated work, whereas the inability to work is a risk factor for mental health of the individual, especially when it involves physical limitations and / or discrimination.
About the low level of schooling, detected in the majority of the clients, was correlated to the unawareness of the available ways to treat CKD.
The study revealed that the majority of the respondents began hemodialysis within six months after diagnosing CKD, i.e. a short time between the discovery of the disease and the beginning of this treatment.
However, this is an alert to the fact that a citizen with more schooling tends to gather better conditions to absorb new information and decide, in a conscientious, on what they feel is best for them.
Thus, it was concluded there among customers of this research troubling socio-demographic and clinical conditions, suggesting interventions / preventive actions to minimize morbidity aspects related to enabling improvements in their quality of life.
Therefore, it outweighs the importance of investing in health promotion and consequent orientation to self-care nursing, particularly in socioeconomically disadvantaged groups. One should also considered the need to facilitate people's access to basic health services, in addition to promoting the training of professionals in the health care network to hypertension, diabetes and CKD so they can be identified early on and properly treated in its early stages.
REFERENCES
1. Xavier BLS. Expectativas do cliente em hemodiálise sobre o transplante renal: pesquisar sociopoético em enfermagem [dissertação de mestrado]. Rio de Janeiro: Universidade do Estado do Rio de Janeiro; 2006.
2. Sociedade Brasileira de Nefrologia. Censo 2011 [texto na internet]. São Paulo: SBN; 2011. [citado em 02 fev 2014]. Available at: URL:http://www.sbn.org.br.
3. Rocha RPF, Santos I dos. Necessidades de autocuidado entre clientes com doença renal crônica: revisão integrativa de literatura. Rev pesq cuid fundamental online. 2009; 1: 423-33.
4. Riella MC. Princípios de nefrologia e distúrbios hidroeletrolíticos. 5ª ed. Rio de Janeiro: Guanabara Koogan; 2010.
5. Canhestro MR, Oliveira EA, Soares CMB, Marciano RC, Assunção DC, Gazzinelli A. Conhecimento de pacientes e familiares sobre a doença renal crônica e seu tratamento conservador. Rev Min Enferm. 2010; 14: 335-44.
6. Xavier BLS, Santos I dos. Expectativas do cliente em hemodiálise sobre o transplante renal: estudo sociopoético. Rev Pesq Cuid fundam. Online. 2010; 2: 1441-9.
7. Santos PR. Relação do sexo e da idade com nível de qualidade de vida em renais crônicos hemodialisados. Rev Assoc Med Bras. [periódico na Internet] 2006 [citado em 29 abr 2014] 52: 356-9. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-42302006000500026&lng=pt. http://dx.doi.org/10.1590/S0104-42302006000500026.
8. Cassine AV, Malagutti W, Rodrigues FSM, Deus RB, Barnabe AS, Francisco L, et al. Avaliação dos principais fatores etiológicos em indivíduos portadores de insuficiência renal crônica em hemodiálise. ConScientiae Saúde. 2010; 9: 462-8.
9. Lopes GB, Martins MTS, Matos CM, Amorim JL, Leite EB, Miranda EA et al . Comparações de medidas de qualidade de vida entre mulheres e homens em hemodiálise. Rev Assoc Med Bras. [periódico na Internet]. 2007 [citado em 29 abr 2014 ]; 53: 506-9. Available at: http://www.scielo.br/scielo.php?script=sci_arttext&pid=S0104-42302007000600017&lng=pt. http://dx.doi.org/10.1590/S0104-42302007000600017
10. Cordeiro JABL, Brasil VV, Silva AMTC, Oliveira LMAC, Zatta LT, Silva ACCM. Qualidade de vida e tratamento hemodialítico: avaliação do portador de insuficiência renal crônica. Rev Eletr Enferm. 2009 [citado em 31 mar 2014] 11: 35-41. Available at: http://www.fen.ufg.br/revista/v11/n3/v11n3a22htm.
11. Ribeiro RCHM, Ferrari RRCHM, Bertolin DC, Canova JCM, Lidimara CEQ. O perfil sociodemográfico e as principais complicações intradialíticas entre pacientes com insuficiência renal crônica em hemodiálise. Arq Ciênc Saúde 2009; 16: 175-80.
12. Santos I dos, Rocha RPF, Berardinelli LMM. Necessidades de orientação de enfermagem para o autocuidado de clientes em terapia de hemodiálise. Rev Bras Enferm 2011; 64 : 335-42.
13. Pacheco GS; Santos I dos. Cuidar de cliente em tratamento conservador para doença renal crônica: apropriação da teoria de Orem. Rev enferm UERJ. 2005; [citado em 07 mar 2014] 13: 257-62. Available at: www.facenf.uerj.br/revenfermuerj.html.
14. Frazão CMFQ, Ramos VP, Lira ALBC. Qualidade de vida de pacientes submetidos à hemodiálise. Rev enferm UERJ. 2011; 19 577-82.
15. Molina CGE, Fierro JGP, Robledo JL, Carrasco RO, Mendoza JAM, Rodrígues VMV. Calidad de vida y depresión en pacientes con insuficiencia renal crónica terminal en hemodiálisis. Med Int Mex. 2009; 25: 443-9.
16. Patat CL. Análise da qualidade de vida de usuários em hemodiálise. Enfermería Global. 2012; 27: 66-76.
17. Mason J, Khunti K, Stone M, Farooqi A, Carr S. Educational interventions in kidney disease care: a systematic review of randomized trials. Am J of Kidney Dis. 2008; 51: 933-51.
18. Carter R, Cheuvront SN, Sawka MN. Doenças provocadas pelo calor. Gatorade Sports Science Institute (GSSI) traduzido e adaptado do original em inglês SSE. 2007[citado em 17 jan. 2014] 19: 102. Available at: http://www.gssi.com.br/publicacoes/sse/pdf/gatoradesse51.pdf>.