REVIEW ARTICLES
Unequal conditions as causes for discontinuation of breastfeeding
Patricia Lima Pereira PeresI; Antônio Olinto PegoraroII
INurse. Professor of the Nursing Department Maternal-Child/Nursing College from the State University of Rio de Janeiro. PhD Student of the Post-graduate Program in Association of Higher Education Bioethics Institutions, Applied Ethics and Public Health, Federal University of Rio de Janeiro/Oswaldo Cruz Foundation/University of the State of Rio de Janeiro/Federal University of Fluminense. Email: patrícia.uerj@hotmail.comABSTRACT: Breastfeeding is a human, social and feminine worldwide practice that spans the centuries. Many studies have been produced to understand the reasons for breastfeeding interruption and the consequent introduction of milk formula. The present study sought to identify, among the causes of breastfeeding interruption described in scientific literature, which are related to unfair and unequal survival conditions in human society. For this, a systematic review was performed within indexed journals extracted from the electronic databases Scientific Electronic Library Online (SCIELO) and Virtual Health Library (VHL) by choosing a time frame of 10 years (2002-2011) and following these descriptors: maternal breastfeeding, breastfeeding and weaning. As a result, 37 articles were selected that described 47 factors for weaning. Of these, 30 are related to social injustice; however, this correlation wasn’t corroborated by some authors that consider these factors just as unfavorable conditions for breastfeeding.
Keywords: Maternal breastfeeding; weaning; justice; social inequality.
INTRODUCTION
Breastfeeding is a practice that spans the centuries, present in all places in which human relations are developed. It is described in the literature as biologically determined and culturally conditioned1, however, its no-practice is old as its practice2,3.
Several studies have been produced in seeking to understand the present reasons for the interruption of breastfeeding and the consequent introduction of milk formula, not only over time, but especially in this century that intensified numerous strategies to promote breastfeeding (BF) and of public policies focused on this issue.
The associated causes are common to the woman's desire to breastfeed, the difficulties in the management of problems related to the physiology of lactation or to ignorance on the part of women about the advantages of BF, leaving covert those related to violation of social rights, from the most basic to the most comprehensive.
By bringing to the debate as a cause of weaning, social conditions that thousands of women and children are exposed, we are dealing with an issue that is present in the daily lives of those who experience breastfeeding and are not perceived as social injustice, but as part of everyday life, distorting the meaning of human rights, in this way:
Poverty, hunger, unemployment, helplessness, or social or economic insecurity, customs and governments who tyrannize are conditions under which people can realize their privations and disadvantages distortedly and even help to develop alternatives or possibilities of change4:14.
Thus, the article aims to present a systematic review about the causes of weaning, highlighting those related to unfair and unequal conditions in society. The interest in this subject arises from reflection about breastfeeding in a bioethical perspective using the framework of justice in Amartya Sen4.
LITERATURE REVIEW
A study performed with 65 professional women and students from a public university in the state of São Paulo, showed that the process of breastfeeding is influenced by the conditions of the domestic environment, work or study and, similarly, the personal relationships present in these environments5.
The need to work to supplement the income6,7, the stress by return causing low milk production and also the unsuitable conditions in the work environment8 have been reasons why formal employment is considered an important cause for weaning, although in this type of bond is that the law of protection of motherhood more advanced, showing that there is still a way to go to strengthen the knowledge on the part of workers and employers about the existing legislation, since the practice was not effective for all, and should be subject to monitoring and mobilization of organized civil society, of trade unions and the Ministry of Labor9-16.
Although motherhood is a practice considered nature, society still expects women to put in the background leaving her forever for later; thus, it is common to observe situations of embarrassment both in the workplace and in school, lack of physical space for the removal of milk or simple emptying of the breast to comfort the woman and not fulfilling the intervals to breastfeed prescribed by law. With respect to interpersonal relationships, these environments are permeated with unequal relationships and the woman is, in most cases, the weakened by the condition after maternity licence still need breaks and spaces for the removal of milk.
The Ministry of Health, through a technical note, set standards for the installation of rooms to support breastfeeding in public or private companies and the inspection of such environments by local health surveillance. The objective is to allow the rooms to the woman who, after maternity license decides to keep the BF, have a suitable breast milk place (milking) and store it safely and with hygiene17. Such technical note appears to unify a practice that was already happening in some both public and private companies, and demystify that such investment is costly for the employer when, on the contrary, has brought numerous benefits, as presented in the document:
Companies also benefit from lower employee absenteeism, considering breastfed children get less sick; secondly, to give greater comfort and value the needs of its employees, the employer may have as return greater adherence to employment and, therefore, stay of skilled personnel; this certainly leads to a more positive perception of the image of the company to employees and society17.
There is no obligation to support room and no law or financial incentive was intended for its installation, it is an imaginative way to promote BF through social responsibility of whoever uses. However, it is necessary that such initiatives also advance to the school spaces, where there is non-observance of the law of protection to motherhood.
Another study, conducted with 12 mothers guided about BF, in a private maternity, pointed out that the tensions generated in the period of breastfeeding strongly influence the decision to breastfeed, being the main factor for weaning. Breastfeeding must always be seen within a larger context than the mother-baby-family universe. When the focus is not dislocated to this triad and the social, political and economic context of the society in which it operates, we limit ourselves to consider the causes of interruption or even denial of breastfeeding are tied to allegations as weak milk, few milk, dried milk or even disinterest of the woman8.
Among the studies produced over the past decade, the main maternal allegations concerned a non-competence to breastfeed perceived by the woman, characterized by a lactation insufficiency. Studies mention that in societies that promotes breastfeeding, making it a habitual practice, lactational insufficiency is rarely observed, differently of the societies in which women are less exposed to breastfeeding and with a greater degree of industrialization18.
If we seek a little deeper into history, we will see that the origin of this concept of lactational insufficiency or lack of milk is linked not only to popular culture, but to concepts strongly widespread in scientific circles in recent decades. A study that examined the knowledge of health professionals (doctors and nurses) about breastfeeding, demonstrated that among the interviewees, 32.7% answered that it is important to change the breast every 10 minutes from the start of suckling and 28.8% reported that it is necessary to establish regular times to breastfeed the baby19.
The health professional is not free to develop their beliefs and assimilate myths from their worldview, knowledge that were built throughout their education, which highlights the need for ongoing training process so that new concepts based on scientific evidence would be assimilated.
Unsurprisingly women show different physiological conditions of man, women menstruate every month; may have premenstrual syndrome; become pregnant and breastfeed, but these differences can not be obstacles to the exercise of its functions of woman, working or student. When these differences are highlighted, we see injustices being triggered and gender inequality, reigning, generating feelings of guilt by pregnancy, weight for maternity license and the very denial of usufruct of the right to breaks provided by law10.
A study conducted in Campina Grande, Paraíba, followed 104 children during 12 months, in a health family unit, and identified that the causes for weaning reported by mothers, were related to the child in 36.8% and 63.2% were due to maternal conditions; the study also found that the use of pacifiers and bottles showed a strong association with early weaning and discontinuation of exclusive breastfeeding (EBF)20.
Study conducted in Piauí, identified that between social classes C, D and E, which reside in rural zone, the practice of BF has higher rates21.The study performed in Bahia found an association between low socioeconomic status and an increase of 2.3 times in the introduction of complementary foods; among those with very poor conditions, the interruption of BF increases to 2.5 times22; another study, also in Bahia, found an association between lower family income and early interruption of exclusive breastfeeding (EBF)23.
It is interesting to note that in two studies in Bahia, low income was a negative factor for the EBF, and not necessarily for breastfeeding, perhaps due to the absence of necessary conditions to keep this type of feeding that requires free demand and in the first months, stay of the mother with the child. In two systematic reviews published in Campinas and Rio de Janeiro respectively, the researchers concluded that the smaller the socioeconomic status, the greater the vulnerability and with it, the risk for weaning6,24.
It has also been suggested as a cause of weaning the belief that breast milk is only required up to 06 months, despite the global recommendation that it be offered exclusively until six months and complementary up to two years or more9,25. The refusal of the child to the breast was also identified as a cause for weaning in 05 studies26-30, this issue is present in many maternal discourse and should be valued in the management of breastfeeding. There are many causes for the child refusal of the breast, among them we can mention the sensation of discomfort or pain in a certain position, too full breast with difficult catches by the baby; too strong or too weak breast milk flow, baby can not make or keep the handle or the use of pacifiers and bottles generating confusion nozzle.
METHODOLOGY
This bibliographic research, which adopted methodological approach was a systematic review, differs from the traditional review by answer a more precise question31. Some authors suggest32 to obeyed three stages – the definition of the purpose of the review.; the identification of the literature; and the selection of studies after evaluation according to the criteria of inclusion and exclusion proposed for the study.
Thus, given what the literature profess for the performance of the systematic review, we selected the following question: among the causes of interruption of breastfeeding described in the scientific literature, which are related to unfair and unequal living conditions in society? For this, it was conducted survey in journals indexed in the electronic databases Scientific Electronic Library Online (SCIELO) and Virtual Health Library (VHL), by choosing a time frame of 10 years (2002-2011). The chosen descriptors were: social justice + breastfeeding + weaning; social justice + breastfeeding + weaning; social inequity + breastfeeding + weaning; social inequity + breastfeeding + weaning; no articles with the association between terms were found. Thus, we chose to use the descriptors: maternal breastfeeding; breastfeeding and weaning.
166 articles were selected, being excluded those whose titles and abstracts indicate address another issue, that did not cover the causes of interruption of breastfeeding; jobs that did not contain the full text; in another language and that used secondary data, as in the case of revisions. We decided to review only national articles due to the proposed issue being more related to the Brazilian reality. The analysis was limited to 37 articles that met the inclusion criteria, being therefore, the worked sample.
RESULTS AND DISCUSSION
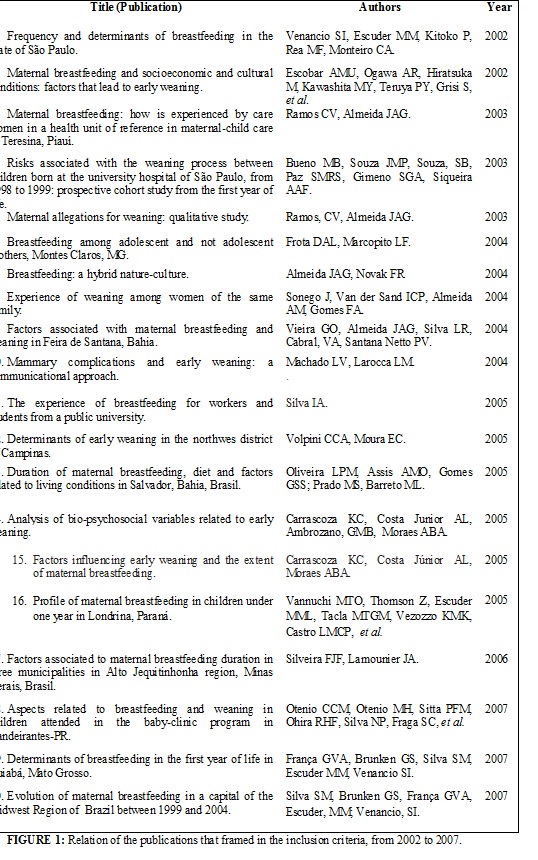
The scientific production examined in the period from 2002 to 2007 is related in Figure 1.
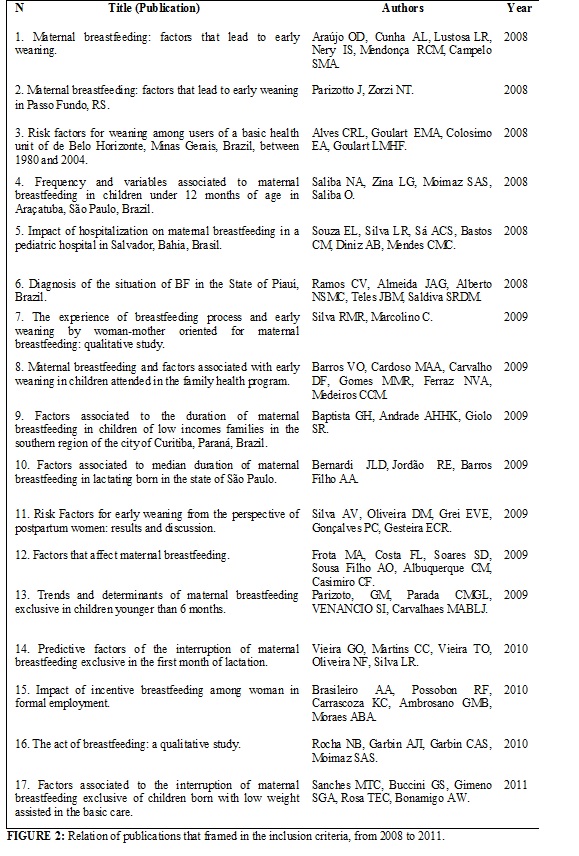
It is noted that, in the period 2002-2007, there was a predominance of publications in 2005 (6 articles) followed by 2004 (5 articles). The scientific production from 2008 to 2011 is exposed in Figure 2, highlighting the prevalence of 2009 (7 articles) and 2008 (6 articles).
The BF is an issue that has been investigated in different regions of Brazil and the causes of weaning, in particular, has been a matter of concern both in quantitative as in qualitative research. Of the 37 articles analyzed, 20 were conducted in the Southeast, of these, one was published in the Northeast; 10 studies were performed in the Northeast, with publication in the Southeast (6) Midwest (1) and three in the region; the five studies in the South, had the following publication distribution: Northeast (1) South (1) and Southeast (3). No study has been found in the Northern Region in the searched database, referring to the period time frame, although there are studies that indicate the situation of the BF in this Region.
Thus, it can be seen that the prevalence in the scientific literature about the topic of breastfeeding and weaning is of the Southeast Region followed by Northeast. In 12 of the studies the qualitative approach was used; in 24 the quantitative approach; and one study used the method qualiquantitative.
Altogether, 47 factors were identified for not breast-feeding or interruption of breastfeeding that can classify into seven groups, according to the referenced texts1-3,5-16,18-30,33, namely: external cause (6); question related to the mother (18); physiological cause/organic (5); causes related to the child (5); unfair/unequal conditions in society (26); culture (9); practices that difficult the feeding (14), as shown in Figure 3.
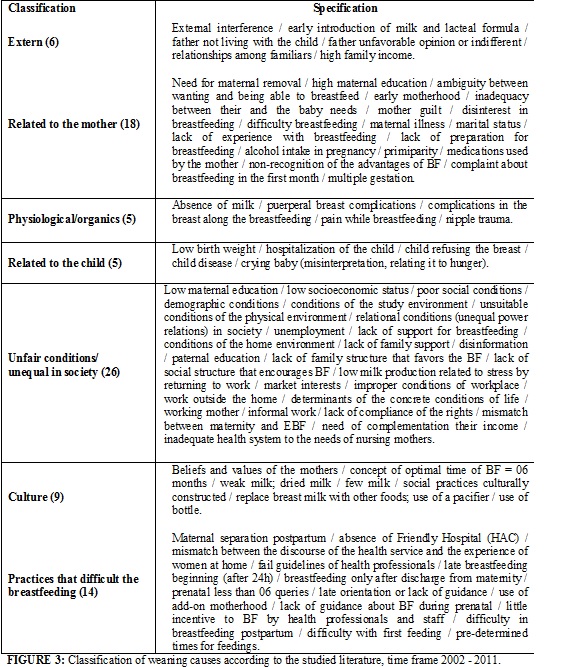
Among the factors discriminated in the seven groups, the study concluded that of 37 articles analyzed, 30 had as causes, factors clearly related to unfair and unequal conditions of survival: low maternal education (5); low maternal socioeconomic status (5); unequal power relations in the study and work environment (2); inappropriate physical environment to the condition of nurse in school and work (2); inadequate health care system to the needs of nursing (3); paternal education (3); maternal employment (including informal employment and unemployment) (14); external influence/influence of grandmothers (3); misinformation (1); milk formulas (3), pacifiers (12) and bottle (4) are products regulated by specific federal legislation and seeks repress abusive marketing mainly focused on nurse and health professionals. Such factors are explored by referenced studies1-3,5-16,18-30,33.
The ambiguity between wanting and being able to breastfeed presented in an article points to the denial of a woman's right to exercise a capacity (capability) their and of the child in obtaining the necessary food for their development, provided in the main documents of child protection.
Clearly unjust and unequal conditions4, presented in the results of the studies reviewed, are treated in most articles as unfavorable conditions for breastfeeding, without, however, discussing that these are social arrangements that need to be combated and reported. Only three articles did make this correlation, citing the lack of social structure conducive to breastfeeding (10); determinants of the actual concrete conditions of lived reality (12); masked market interests of scientific knowledge disguised of devices for health33, in a reference to the weaning of exceptionality; weaning socioculturally constructed, highlighting that the woman needs support not only from family and health professionals, but also, government support, which requires the formulation of laws that ensure conditions for the exercise of this practice.
However, more than formulate new laws exist the need to create mechanisms to ensure the inviolability of rights already conquered, similarly, to generate conditions for unfairly included, do not become excluded, but also included34:25.
Although in the analyzed articles the discussions about these social determinants have been superficial or non-existent, some authors suggest the search for new standards to support health actions in order to contemplate social and political constraints. It can not deny that there is a promotion law and extensive protection of the specific point of view of maternity and in particular, breastfeeding, which contemplates the assistance to pregnancy, childbirth and puerperium; worker protection, to the student through maternity license and convict, providing a safe place during the of breastfeeding period; the presence of milk dispensary and breastfeeding room at daycare is another existing law, but that is also not fulfilled in its entirety.
Going through the entire law, we can see that it did not achieve the realization of these rights equitably in different strata of society, between social groups with higher income and higher education work the demands made act pressure force and are in most met, either the public, whether in the private, which shows that inequality is classes.
Laws abound, is missing its effectiveness through public social protection policies; that adds the misinformation that is a limiting element of decision-making capacity and choices compromising the autonomy and providing that the subjects remain sidelined of necessary achievement to improve the quality of life for the woman and the child. It is in this context that we understand that bioethics has an important contribution to offer through issues such as autonomy/freedom; human rights fact applications; emancipation/citizenship.
The ethics and bioethics that permeate social relations should be evoked when faced with situations where rights are violated. Women and children need to have guaranteed their rights to a dignified existence, this assumes that the fundamental right to life and, therefore, the right to food, freedom and the bond are protected.
CONCLUSION
Unequal conditions in the society, pointed out in the study, can not be treated as the background, but as determinants of not-breastfeeding and weaning to be combated. These conditions that point to the understanding that the BF is not a health practice, but a human female and social practices and should be protected as a human right.
Another important issue that we can extract of the texts is that low education, low income, asymmetrical power relations in the workplace or school, inadequate health care needs of nursing mothers and babies, indiscriminate marketing of milk formula are injustices in society that generate deprivation in the form of unfair exclusion or inclusion, but there are legal frameworks to address them. Give light to the category social injustice, as a causal factor for breast-feeding and weaning, unlike considering just as unfavorable conditions, perhaps is nowadays the biggest challenge for the promotion, protection and support to BF.
Thus, unveiling the real dimension that this category has about women and children can lead us to think public policy and social strategies for solving them within the intersectoral and greater social participation. It is necessary, therefore, that other landmarks are incorporated into the debate, being bioethics an important reference for understanding breastfeeding as human, social and feminine practice.
REFERENCES
1. Almeida JAG. Amamentação: um híbrido natureza-cultura. Rio de Janeiro: FIOCRUZ; 1999.
2. Ichisato SMT, Shimo AKK. Revisitando o desmame precoce através da história. Rev Latino-Am Enfermagem. 2002;10:578-85.
3. Monteiro JCD, Nakano AMS, Gomes FA. O aleitamento materno enquanto uma prática construída: reflexões acerca da evolução histórica da amamentação e desmame precoce no Brasil. Invest Educ Enferm. 2011;29: 315-21.
4. Sen A. Desigualdade reexaminada. São Paulo: Companhia das Letras; 2012.
5. Silva IA. A vivência de amamentar para trabalhadoras e estudantes de uma universidade pública. Rev Bras Enferm 2005; 58:641-56.
6. Faleiros FTV, Trezza EMC, Carandina L. Aleitamento materno: fatores de influência na sua decisão e duração. Rev Nutr [online]. 2006; 19: 623-30.
7. Frota MA, Costa FL, Soares SD, Sousa Filho AO, Albuquerque CM, Casimiro CF. Fatores que interferem no aleitamento materno. Rev RENE. 2009;10(3): 61-7.
8. Carrascoza KC, Costa Junior AL, Ambrozano GMB, Moraes ABA. Análise de variáveis biopsicossociais relacionadas ao desmame precoce. Paidéia (Ribeirão Preto) [online]. 2005; 15 (30): 93-104.
9. Silva RMR, Marcolino C. A vivência do processo de amamentação e desmame precoce por mulheres-mãe orientadas para o aleitamento materno: estudo qualitativo. Online braz j nurs. (Online) 2009; [citado em 12 jan 2014] 8. Available at: http://www.objnursing.uff.br/index.php/nursing/article/view/j.1676-4285.2009.2019/460.
10. Ramos CR, Almeida JAG. Alegações maternas para o desmame: estudo qualitativo. J Pediatr (Rio de Janeiro). 2003;79: 385-90.
11. Venancio SI, Escuder MM, Kitoko P, Rea MF, Monteiro CA. Frequency and determinants of breastfeeding in the State of São Paulo. Rev Saude Publica. 2002; 36: 313-8.
12. Vieira GO, Almeida JAG, Silva LR, Cabral VA, Santana Netto PV. Fatores associados ao aleitamento materno e desmame em Feira de Santana, Bahia. Rev bras saúde matern infant. 2004; 4: 143-50.
13. Frota DAL, Marcopito LF. Amamentaçäo entre mães adolescentes e näo-adolescentes, Montes Claros, MG. Rev Saude Publica. 2004; 38: 85-92.
14. Parizotto J; Zorzi NT. Aleitamento materno: fatores que levam ao desmame precoce no município de Passo Fundo, RS. O Mundo da Saúde. 2008; 32:466-74.
15. Baptista GH, Andrade AHKG, Giolo SR. Fatores associados à duração do aleitamento materno em crianças de famílias de baixa renda da região sul da cidade de Curitiba, Paraná, Brasil. Cad Saúde Pública [online]. 2009; 25: 596-04.
16. Rocha NB, Garbin AJI, Garbin CAS, Moimaz SAS. O ato de amamentar: um estudo qualitativo. Physis (Rio de Janeiro). 2010; 20: 1293-305.
17. Agência Nacional de Vigilância Sanitária (Br). Nota técnica conjunta nº 01/2010 ANVISA e Ministério da Saúde. Assunto: Sala de apoio à amamentação em empresas. Brasilia (DF): ANVISA; 2010.
18. WHO. Alimentação infantil: bases fisiológicas. Traduzido por IBFAM-BRASIL e Instituto de Saúde. São Paulo: WHO; 1997.
19. Arantes CIS, Montrone AVG, Milioni DB. Concepções e conhecimento sobre amamentação de profissionais da atenção básica à saúde. Rev Eletr Enf [Internet]. 2008; [citado em 12 jan 2014] 10:933-44. Available at: http://www.fen.ufg.br/revista/v10/n4/v10n4a06.htm.
20. Barros VO, Cardoso MAA, Carvalho, DF, Gomes MMR, Ferraz, NVA, Medeiros CCM. Aleitamento materno e fatores associados ao desmame precoce em crianças atendidas no programa de saúde da família. Nutrire Rev Soc Bras Aliment Nutr. 2009; 34: 101-14.
21. Ramos CV, Almeida JAG, Alberto NSMC, Teles JBM, Saldiva, SRDM. Diagnóstico da situação do aleitamento materno no Estado do Piauí, Brasil. Cad Saúde Pública [online]. 2008; 24:1753-62.
22. Oliveira LPM, Assis AMO, Gomes GSS, Silva MSP, Barreto ML. Duração do aleitamento materno, regime alimentar e fatores associados segundo condições de vida em Salvador, Bahia, Brasil. Cad Saúde Pública [online]. 2005; 21: 1519-30.
23. Souza EL, Silva LR, Sá ACS, Bastos CM, Diniz AB, Mendes CMC. Impacto da internação na prática do aleitamento materno em hospital pediátrico de Salvador, Bahia, Brasil. Cad Saude Publica; 2008; 24: 1062-70.
24. Rivemales MC, Azevedo ACC, Bastos PL. Revisão sistemática da produção científica da enfermagem sobre o desmame precoce. Rev enferm UERJ. 2010; 18:132-7.
25. Alves CRL, Goulart EMC, Colosimo EA, Goulart LMHF. Fatores de risco para o desmame entre usuárias de uma unidade básica de saúde de Belo Horizonte, Minas Gerais, Brasil, entre 1980 e 2004. Cad Saúde Pública. 2008; 24: 1355-67.
26. Escobar AMU, Ogawa AR, Hiratsuka M, Kawashita MY, Teruya PY, Grisi S, et al. Aleitamento materno e condições socioeconômico-culturais: fatores que levam ao desmame precoce. Rev Bras Saude Mater Infant [online]. 2002; 2(3) 253-61.
27. Volpini CCA, Moura EC. Determinantes do desmame precoce no distrito noroeste de Campinas. Rev nutr. 2005; 18: 311-9.
28. Otenio CCM, Otenio MH, Sitta PFM, Ohira RHF, Silva NP, Fraga SC, et al. Aspectos associados à amamentação e desmame em crianças atendidas no programa bebê-clínica em Bandeirantes-PR. Salusvita; 2007;26(2): 45-53.
29. Frota MA, Costa FL, Soares SD, Sousa Filho AO, Albuquerque CM, Casimiro CF. Fatores que interferem no aleitamento materno. Rev RENE. 2009:10(3): 61-7.
30. Araújo OD, Cunha AL, Lustosa LR, Nery IS, Mendonça RCM, Campelo SMA. Aleitamento materno: fatores que levam ao desmame precoce. Rev Bras Enferm. 2008; 61: 488-92.
31. De-La-Torre-Ugarte-Guanilo MC, Takahashi RF, Bertolozzi MR. Revisão sistemática: noções gerais. Rev esc enferm. USP. 2011; 45: 1260-6.
32. Sampaio RF, Mancini, MC. Estudos de revisão sistemática: um guia para síntese criteriosa da evidência científica. Rev Bras Fisioterapia. 2007; 11(1): 83-9.
33. Almeida JAG,Novak FR. Amamentação: um híbrido natureza-cultura. J Pediatr (Rio de Janeiro) 2004; 80 (5): S119-S20
34. Bobbio N. A era dos direitos. Rio de Janeiro: Elsevier; 2004.