RESEARCH ARTICLES
Public health policies for breast cancer control in Brazil
Carla Andréia Vilanova MarquesI ; Elisabeth Níglio de FigueiredoII; Maria Gaby Rivero de GutiérrezIII
INurse. Master and PhD student at the Graduate Nursing Program, Federal University of Sao Paulo. Brazil. E-mail: cvilanova@inca.gov.br.
IINurse. Associate Professor at the Paulista School of Nursing, Federal University of Sao Paulo. Brazil. E-mail: elisabeth.niglio@unifesp.br.
IIINurse. Tenured Professor at the Paulista School of Nursing, Federal University of Sao Paulo. Brazil.
E-mail: gaby.gutierrez@unifesp.br
IVAcknowledgements to the National Council of Science and Technology for providing productivity in research grant level 1B and Higher Education Personnel Training Coordination by the granting of the master's scholarship.
DOI: http://dx.doi.org/10.12957/reuerj.2015.13632
ABSTRACT: This study described public healthcare measures for breast cancer control in Brazil. A narrative review of official government websites was performed, with no time restriction, and analyzed against current health policies in place in Brazil. As a result, 48 publications were detected, revealing that cancer treatment has been considered in public health circles since 1984, but not until 1996 was a specific program started for this disease. In 2004, the measures, resources, target public and screening and early detection indicators were defined, but computerized monitoring of these practices started two years after implementation. In conclusion, the documentation reviewed showed that public health interventions for breast cancer control have increased considerably since 1998, and that more policies have been directed to screening and early detection since 2004.
Keywords: Breast neoplasms; primary health care; mass screening; public health policy.
INTRODUCTION
Cancer has been recognized as a public health problem in Brazil since 19191, however, from 1975, with the creation of the information system was observed that mortality among the cancers in women, which breasts already showed high prevalence and mortality in the country2. These epidemiological profile data, among other factors, may have contributed to its inclusion on the agenda of public policies in health, in the year, 19843.
However, despite being formulated proposals for the control of breast cancer, there was an increase in mortality from this cancer from 2003 to 2007, in the South and Southeast, highlighting São Paulo (12%), Rio de Janeiro (6%) and Minas Gerais (22%), attributed by the authors to the variation of access to health services and quality of registration data4.
It is known that this disease, most of the time, grows slowly and may be diagnosed in the initial phase by the use of isolated or combined methods of mammography (MMG), clinical breast exam (CBE) and the encouragement of Self Breast Examination (SBE) aiming at body care5,6. The decrease of sequels, best therapeutic responses, as well as increasing the cure rate has been observed in systematic screening programs, thus endorsing the formulation of public health actions5-7. Despite these findings, studies in the Brazilian population reveal that the diagnosis still occurs in advanced stage and survival is low4,8.
Knowing and analyzing the intervention strategies in any health policy or program enables one to identify the factors that interfere with its implementation and can contribute to developing measures that stop, accelerate or modify9. It is noted that the Brazilian public health proposals for the control of breast cancer have been described in various documents and articles10-23, making it difficult to understand the links between them. This study aims to describe which were to public health actions to control breast cancer in Brazil, determined over time.
METHODOLOGY
This is a narrative review24 on proposed public healthcare interventions for the control of breast cancer in Brazil. It should be noted that the review does not presuppose narrative exhaustive search on the object of research, yet allows for description and understand the choices made.
With the focus of the study being meeting public health interventions for breast cancer, in 2009 and 2013, all pages of the website of the National Cancer Institute were consulted (http://www2.inca.gov.br/wps/wcm/connect/inca/portal/hom) and the Ministry of Health (MH), the Health Portal (http://pthertalsaude.health.gov.br/portalsaude/busca), the Publisher's page (http://dtr2001.saude.gov.br/editora/produtos/livros/genero/livros.htm#p) the collection of publications and texts of the Virtual Health Library (http://bvsms.saude.gov.br/metaiah/search.php#).
The search was conducted without restriction of year, using the words cancer and women's health. Inclusion criteria were publications in Portuguese, Spanish or English addressing actions for the control of breast cancer. It also used a reverse search24 to check those references that met the inclusion criteria. Of the 48 publications included there were Ordinances, laws, official notes, programs and health policies. These were described strategies, goals and organs responsible for the proposal. In chronologically sorting the findings, the date of disclosure was considered and the results were presented as follows: before 1998, 1998-2003 (control program institution of breast cancer) and after 2004 (definition of strategic actions). Data analysis was carried out in the light of current health policies in the country.
RESULTS
Proposed actions before 1998
From the disclosure of therapeutic discoveries for some types of cancerthe interest of the medical category increased, contributing to reorder the priorities in public health, before pointing only to infectious and contagious diseases1.
The inclusion of neoplasms in the national public agenda occurred when its etiology has been considered possibly contagious and preventable. Thus, cancer was inserted into the list of diseases of the National Department of Public Health, created in 1919 to control infectious diseases contagious and to analyze the causes of death1.
Another landmark date of 1941 and refers to the establishment of the National Cancer Service (NCS) to guide and coordinate the oncology actions of public and private services. The NCS was also tasked to develop research, epidemiological control and health education to the population and professionals1. It is observed that until then, prioritized actions were not specific to breast cancer.
However, from 1984 through the Women's Health Comprehensive Care Program (WHCCP), coordinated by MH3, this scenario changed with the expansion of interventions beyond the gravid period, including breast cancer. Also in this decade, the Oncology Program proposed to regain control of Neoplasms by professional training and educational activity1.
In the late 80s, there was a new logic of financing and operation of the Brazilian healthcare system with the implementation of the Unified Health System (SUS)25, and the National Cancer Institute (NCI) became the Assistant MH assuming NCS assignments1.
With regard for oncological therapy, the Technical Ordinance (TO) Nº 170/93, repealed by Nº 3535/99, standardized the accreditation of hospitals that perform highly complex procedures.
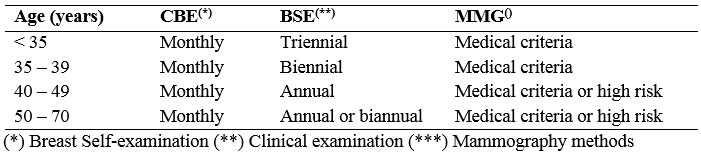
In order to reduce mortality and breast cancer effects in 1996, NCI coordinated the pilot program for breast and cervical cancer screening entitled Viva Woman Program11. Previously, the actions were carried out in isolation and disorganized, hindering access. The breast cancer screening actions recommended by MH, followed recommendations of the Pan-American Health Organization for Latin America and Caribbean12 with minor modifications.
TABLE 1: Actions recommended by the INCA for screening of breast cancer in Brazil, according to the recommendations of OPS for Latin America and the Caribbean before 1998.
Actions proposed from 1998 to 2003
In 1998, with the Viva Woman Program, opportunistic screening actions of breast and cervical cancer were deployed. Therefore, in 2000 were trained in breast radiology, 960-trained professionals and 432 municipal managers. In addition, it was observed that the provision of resources for the control of cervical cancer was higher than the breast and, this lacked specifications for the priority actions, target audience, form of operation, parameters to estimate the coverage of actions and equipment, as well as monitoring indicators and/or evaluation. In 2001, educational materials were prepared for the training of these professionals to perform the CBE, and purchased 50 mammographers (MMG) and 50 processors11. Later this year, the NCI guided the protocols for the treatment of this cancer13 and Law Nº 10.223 made it mandatory health insurance the cost of breast reconstructive plastic surgery.
TO n° 1.101 of 2002 proposed assistance coverage parameters in SUS: internationally recognized social assistance parameters; attendance statistics users of SUS and the national implications, by specialties, the past three years; services offered, including diagnostic and therapeutic, based on studies and opinions of technicians and assistance parameters of various institutions of the country. For programming, the diagnostic arsenal of equipment parameters were built that indicated a mammography unit for each 240.000 inhabitants and an ultrasound device for every 25.000. In contrast, official data published in 2006, on the number of mammographies demonstrated the capacity from 50% to coverage of women over 50 years old and concentration of 47,26% of the country's Southeast Region14. From 1998 have been published several ordinances to standardize the cancer care in the SUS.
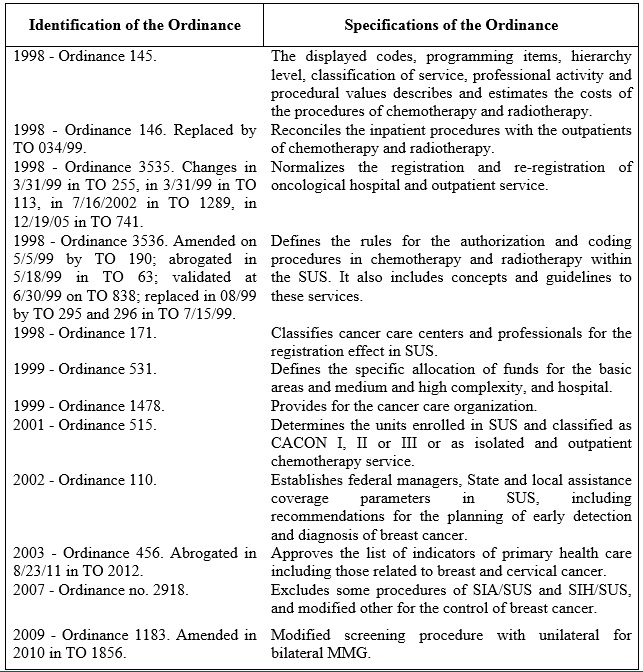
FIGURE 1: Technical Ordinances that direct public actions for the control of breast cancer - 1998-2011.
Proposed actions after 2004
In 2004, the National Policy of Comprehensive Care in Women's Health was launched and coordinated by the MH, in which it was agreed to reduce morbidity and mortality from preventable causes including breast cancer3. The proposed strategies have guided the Organization of reference and counter-reference network for diagnosis and treatment of this tumor. The female mortality rate for breast cancer and breast reconstruction have become indicators of interventions3.
Now in the consensus of Breast Cancer Control15, of all the guidelines the actions prioritized assistance for detection and health promotion. They have determined whether the criteria for cytological and histopathological diagnosis, the use of diagnostic technology (MMG, breast ultrasound and biopsy), the types of treatment (surgery, radiotherapy, hormone therapy and palliative care) and activities of the multidisciplinary team. The age and the high risk became indicative criteria for the screening and the frequency of the examinations.
INSERIR AQUI - Figura 2
These recommendations were based on international studies, due to the absence of national data15. Since then, in addition to the female mortality rate for this cancer, the mammography was constituted as an indicator15. In 2005, the TO in 2439, the National Policy of Oncology Care was presented and objectives for the control of cancer re-established, involving addition of high complexity assistance, medium complexity and primary care16.
On the Action Plan for the Control of Cervical and Breast Cancers, 2005-2007, the role of the primary care team was considered a tactic to reduce the incidence and mortality of these tumors10. In addition, seeking to articulate assistance network formation and improve the features, was proposed in 2006, the pilot project of Mammography quality assurance17. In March this year, the implementation of the National Policy of Primary Care appointed basic healthcare units (BHU) as the preferred contact for users18.
Thus, aiming to overcome the SUS consolidation difficulties, managers of the three spheres developed the Pact for Health consists of three dimensions: for life, in defense of the SUS and management19. The pact for life focused on six health problems, including breast cancer19.
Strategically, to enhance adherence to the agreed actions, a determined BHU team focused on attracting the target women; the implementation of the women's agenda; the referral of patients with result of MMG or CBE suspects or altered; educational activities; active search for defaulting, the suspicious reports and who have never performed the CBE or MMG, as well as the guidance and monitoring of women with low-risk and regular CBE20.
Although previous documents orient what would be the target audience for screening of breast cancer, item III of Law 11.664 of 29/4/2008 which ensured in the country performing mammography for all women after 40 years age, created a divergence from government proposals already established (Figure 2).
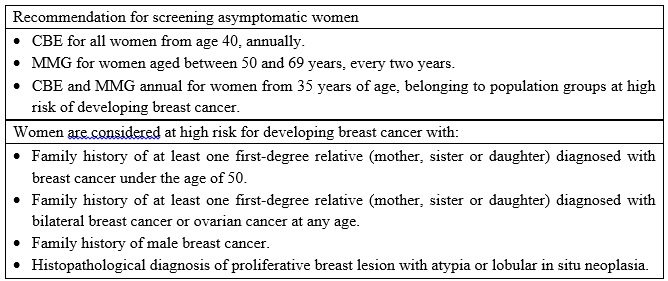
FIGURE 2: Consensus of breast cancer control, National Cancer Institute. Rio de Janeiro, Brazil 2004.
In order to know the organization and results of systematic and opportunistic screening programs in several countries in 2009 there was a meeting at the NCI21, resulting in the institution, in the city of Curitiba, the first screening pilot program titled Woman of Curitiba Program22. In this project, which is still under monitoring, it is expected to identify the difficulties and facilities in the operationalization of the convocation, director of MMG, diagnostic confirmation and referral to treatment.
Supported by TO nº 779, began in June 2009 the implementation of SISMAMA information system in BHU and MMG services, generating the implementation of that survey data from 2010. In addition, based on international and national studies, we estimated the need for specific actions to control this neoplasm23.
In March 2011, there were three goals reaffirmed for the control of breast cancer: early diagnosis guarantee of palpable lesions; MMG offer of screening to the target audience; and qualification of the health care network. These proposals were presented in the action axis strengthening of the National Breast Cancer Control Program, Cancer National Plan for Strengthening Prevention Network, Diagnosis and Treatment of Cancer. Since the TO nº 558 of 24/03/2011 presented the Technical Advisory Committee to monitor the policy of prevention, diagnosis and treatment of cervical and breast cancers. This plan resulted in the publication, in March 2012, TO Nº 531, which established the National Program for Quality Mammography, after positive results presented in 2008, four locations that have implemented and monitored the project started in 2006.
DISCUSSION
The survey conducted shows an increase of publications from the year 1998, showing the inclusion of the control of breast cancer on the agenda of public health policies in Brazil. Note also that before 1998 were public services like the National Department of public health1, the NCS1, MH3and the NCI1 who worked for the control of neoplasms and the inclusion of specific actions for breast cancer. The main interventions guided on Standardization of tertiary care31, job training, health education1and running a pilot project for screening without normative specifications11. Reflection on the time gap between creating and embedding knowledge in health can justify part of the findings, since the first international and national reports of oncological surgery occurred between 1840 and 1900, the radiotherapy between 1904 and 1919 and the use of chemotherapy, in the 50s, when production occurred in scale of these drugs by the pharmaceutical industry1.
As for the Brazilian health system, before 1988, it assumed the Bismarckian model, with contributions from employees, employers and government in public cases systems for professional categories. A small portion of the population had employment, resulting in restricted coverage and access to health services. Public interventions were minimal and there was an important act of philanthropic institutions25. During this period, urbanization, aging population and advances in health care have contributed to the decline of infectious contagious diseases and the increased prevalence of chronic degenerative25, including breast cancer. Under social politician, provisional Governments and strong military interference, limited social participation in policy decisions, generating internal conflicts, lack of provision of resources and discontinuity of the public health actions1,25. Social dissatisfaction mobilized several sectors, including health, which proposed with the SUS, the reorganization and expansion of assistance, with a focus on basic care25.
That way, the findings before 1998, probably arising from the consolidation process influences the knowledge in Oncology and the characteristics of the current healthcare system.
In 1998, following the point against gradual deployment of SUS, the reasonable economic and social stability of Brazil, as well as the consolidation of knowledge and advances in Oncology, possibly were boosters of public health actions in this area1,25.
In the process of implementation of the Viva Woman Program, it was observed that the investments and the provision of services for the control of cervical cancer were higher and faster than the breast11. The lack of specification of the target audience, the diagnostic criteria and Foundation for the control of breast cancer may have a causal relationship with the scarce resource allocation at the beginning of the program. Still in the period of 1998 to 2003, it was observed that 10 Ordinances were prepared with an emphasis on cancer care organization, three levels of health care in the SUS, being mostly directed towards therapy. Only TO Nº 1101 of 2002, established MMG and USG breast coverage parameters. From the 10 ordinances, two have been repealed, three replaced, five changed and validated, which may result in fragmentation and discontinuity of the proposals. In this period, there was a breakthrough of the actions still focused on therapeutic actions13, however, standardized and carried out by public bodies12, unlike the previous phase, where the role of the State was fragile.
In order to complement, from 2004, with the launch by MH of the consensus document15, the regulatory gaps indicated above have been resolved. Since this period, several important documents and specific to this type of tumor,10,14-24 were produced. As for SISMAMA data for the early detection and tracking of this neoplasia, have been produced, because the system is still in deployment in the Country14. According to the NCI, the vast territorial extension and the high number of target individuals makes it impossible, at the time, the stock offering systematic tracking15,20-22, although its benefits be recognized since 19635.
It must be considered that the actions proposed in the consensus15,20 for this cancer, are part of a health policy of a developing nation. The Brazilian SUS was promulgated in 1990 and continues to be structured until today25. This health system aims to universal coverage, funding and managing subsidized by the balls Federal, State and Municipal government and spaces for social participation for the control and setting priorities in the public agenda25. Even so, the healthcare sector has received few resources and their regulation mechanisms are being incorporated, which favors the discontinuity of the actions in public health25.
The nexus of national public actions for the control of breast cancer that were presented in this study, however, we did not consult theses, dissertations and monographs, and may have left out some data in addition to information in the temporal analysis. However, this review identified, over the years, objectives, actions and focus of interventions toward the problem.
CONCLUSION
The documents analyzed for the period before 1998 emphasize the creation of entities of cancer services management, training in this area and the expansion of tertiary healthcare.
The production of documents from 1998 to 2003 has grown considerably, probably influenced by the restructuring of the healthcare system. Therapeutic interventions were still the most common in this scenario; however, note that the targeted primary care are gaining prominence.
After 2004, it should be noted that breast cancer won space on the political agenda and to proposals for improvements and expansion of the network continue to structure at different levels of health care, with a focus on early detection and tracking of this interlocutory appeal.
It should be considered that this trajectory is shaped according to the social, political and economic characteristics and health problems of developing countries, in addition to extensive territorial size and limited resources. Still, it is expected that the compilation of knowledge about the public health actions to control the Brazilian breast cancer encourages its review and support the decision making of the managers.
REFERENCE
1.Teixeira LA, Fonseca CM. De doença desconhecida a problema de saúde pública: o INCA e o controle do câncer no Brasil. Rio de Janeiro; Ministério da Saúde. 2007.
2.Wünsh VF, Moncau JE. Mortalidade por câncer no Brasil 1980-1995: padrões regionais e tendências temporais. Rev Assoc Bras. 2002; 48(3): 250-7.
3.Ministério da Saúde (Br). Política nacional de atenção integral à saúde da mulher: princípios e diretrizes. Brasília (DF): Editora MS; 2004.
4.Zapponi ALB, Melo ECP. Distribuição da mortalidade por câncer de mama e de colo de útero segundo regiões Brasileiras. Rev enferm UERJ. 2010; 18:628-31.
5.World Health Organization. International Agency for Research on Cancer (IARC). Breast Cancer Screening. Lyon (Fr): WHO; 2002.
6.Organización Mundial de la Salud. Programas nacionales de control del cáncer: políticas y pautas para la gestión. Ginebra (Swi): OPS; 2004.
7.Coleman MP, Quaresma M, Berrino F, Lutz JM, De Angelis R, Capocaccia R, et al. Concord working group: cancer survival in five continents: a worldwide population-based study. Lancet Oncol. 2008; 9(8):730-56.
8.Liedke PE, Finkelstein DM, Szmonifka J, Barrios CH, Chavarri-Guerra Y, Bines J, Vasconcelos C, Simon SD, Goss PE. Outcomes of breast cancer in Brazil related to health care coverage: a retrospective cohort study. Cancer Epidemiol Biomarkers Prev. 2014;23(1):126-33.
9.Mendes JMR, Garcia MLT, Oliveira EFDA, Fernandes RMC. Gestão na saúde: da reforma sanitária às ameaças de desmonte do SUS. Texto contexto – enferm. 2011; 10:331-44.
10.Ministério da Saúde (Br). Plano de ação para o controle dos cânceres do colo do útero e da mama 2005 -2007. Brasília (DF): MS; 2005.
11.Instituto Nacional de Câncer (Br). Viva Mulher: câncer de colo de útero, informações técnico gerencial de ações desenvolvidas. Rio de Janeiro; INCA; 2002.
12.Lopes ER, Abreu E, Gadelha MIP. Detecção do câncer de mama: atualização e recomendações. Rev Bras Cancerol. 1993; 39(1):21-26.
13.Instituto Nacional de Câncer (Br). Câncer de mama: condutas do INCA/MS. Rev Bras Cancerol 2001; 47(1): 9-19.
14.Instituto Nacional de Câncer (Br). A situação do câncer no Brasil. Brasília (DF): Editora MS; 2006.
15.Instituto Nacional de Câncer (Br). Controle do câncer de mama: documento de consenso. Rio de Janeiro: INCA; 2004.
16.Portaria n°2439/GM de 8/12/2005: institui a política nacional de atenção oncologia. Brasília (DF) [periódico na internet] [citado 30 mar 2013]. Disponível em: http://www.saude.pr.gov.br/arquivos/File/retrol/registrocancer/Portaria2439GM_MS.pdf
17.Instituto Nacional de Câncer (Br). Mamografia: da prática ao controle. Rio de Janeiro; INCA. 2007.
18.Portaria nº 648/GM de 28/03/2006: aprova a Política Nacional de Atenção Básica. Brasília (DF) [periódico na internet] [citado 26 ago 2014] Disponível em: http://dtr2001.saude.gov.br/sas/PORTARIAS/Port2006/GM/GM-648.htm.
19.Ministério da Saúde (Br). Painel de Indicadores do SUS 2006. Brasília (DF): MS; 2006.
20.Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Controle dos cânceres do colo do útero e da mama. Brasília (DF): Editora MS; 2006.
21.Instituto Nacional de Câncer (Br). Coordenação Geral de Ações Estratégicas. Encontro internacional sobre rastreamento do câncer de mama: resumo das apresentações. Rio de Janeiro: INCA; 2009.
22.Instituto Nacional de Câncer (Br). Rastreamento organizado do câncer de mama: a experiência de Curitiba e a parceria com o Instituto Nacional do Câncer. Rio de Janeiro: INCA; 2011.
23.Instituto Nacional de Câncer (Br). Parâmetros para o rastreamento do câncer de mama: recomendações para gestores estaduais e municipais. Rio de Janeiro: INCA; 2009.
24.Rother ET. Revisão sistemática X revisão narrativa.Acta Paul. Enferm. [online]. 2007; vol.20, n.2, pp. v-vi.
25.Paim J, Travasso C, Bahia CA, Macinko J. O sistema de saúde Brasileiro: história, avanços e
desafios. The Lancet – Saúde no Brasil. 2011 maio; 11-31.