RESEARCH ARTICLES
Anxiety level of companions of children in outpatient surgery: contributions of the nursing consultation
Carlos Eduardo Peres SampaioI; Raquel Vianna SilvaII; LianyBonilla da Silveira CominoIII; Regina Aurora Trino RomanoIV
INurse, PhD, Associate Professor, Department of Medical-Surgical Nursing, State University of Rio de Janeiro, Asssistant Professor at the Universidade Veiga Almeida. Research Advisor Rio de Janeiro, Brazil, Email: carlosedusampa@ig.com.br.
IINurse, Graduated in Nursing from the University of Grande Rio. Rio de Janeiro, Brazil, Email: raquel.silva02@yahoo.com.br
IIINurse, Master's in Nursing, Assistant Professor, Department of Public Health Nursing, School of Nursing, State University of Rio de Janeiro. Rio de Janeiro, Brazil, Email: liany@unisys.com.br
IVNurse, Master in Educational Technologies in the Health Sciences. Assistant Professor, Department of Medical-Surgical Nursing, School of Nursing, State University of Rio de Janeiro, Brazil. Email: reginatrino@hotmail.com.
ABSTRACT: It is an analytical and comparative study with a quantitative approach; the general objective of the study is to compare the influences of the nursing consultation in the degree of trait and state anxiety two groups of child companions in a surgical situation. The scenario was the policlinic in the city of Rio de Janeiro. The study occurred in the period of March to August of 2012. The study population was 42 mothers of children who had been undergone pediatric surgery. The subjects were 100% mothers and divided into two groups: one that received nursing pre-operatory orientations (n=21) and the other that didn’t (n=21). The mothers who received the orientations had a lower degree of anxiety.
Keywords: Nursing assistance; companions; children; anxiety.
INTRODUCTION
Ambulatory surgery had its beginnings in the 60s, with numerous advantages in comparison with classical surgery hospital, such as decrease the number of hospitalizations, reduced hospital costs by 25% to 75%; release of hospital beds; reduced anxiety, greater comfort for patients and caregivers; early return home and routine activities, in addition reducing the risk of nosocomial infection1.
The companion, generally, is the person closest to the child: a family member who will provide emotional support and affection, easing the concerns, anxiety and fear. Thus, making the child more confident and emotionally stable. The family companion profile in terms of gender is predominantly formed by mothers and grandmothers, highlighting the importance of the nurse motivating the companion to involve other family members in child care2.
The parents, in their majority, are anxious when their children are submitted to a surgical procedure3 and, at this moment, some factors are responsible for this anxiety and concern with injuries that may occur, fear of pain in the postoperative period, separation from the family, fear of is incapacitated, fear of not waking up from anesthesia and fear of general complications. Thus, parents must be informed and encouraged to actively participate in their children's treatment, contributing positively to their presence and safety. Throughout the perioperative period, parents need to be informed about the state of the child, the progress and the time for the end of the surgery. This attitude is of great importance to soothe and comfort them4.
The surgery, because it is a strange situation for both the child as well as for the companion, contributes to an increase in the level of anxiety of both, the procedure to be performed5.The state of anxiety causes various changes such as dryness of the mouth, sweating, palpitations, vomiting, chills, elevation of blood pressure, respiration and heart rate6.
The relevance of this research is the fact of being able to identify the contributions of the nursing consultation, with respect to the degree of trait and state of anxiety for the companion of the child subjected to the surgical procedure.
Thus, the general objective of the study is to compare the influences of the nursing consultation in the degree of trait and state of anxiety in two groups of child companions in surgical situations.
LITERATURE REVIEW
The nursing consultation in the period before surgery is a very important tool to reduce anxiety both the child and the family have just received the surgical diagnosis. At this time, the nurse explains how the surgery will be performed, which required care with the child before the surgery; you know the medical history of the patient and the family history. Also encourages responsible to express their feelings and fears and, through dialogue, the nurse can identify the level of information from the family about the procedure to be performed, clarifying any doubts to ease fears, anguish, anxiety and insecurity. This evaluation process contributes to the planning of an individualized nursing care of high quality in the trans and post-operative periods7,8.
The main care activities performed by nurses of the outpatient surgery department is receiving the patient in the operating room, conference of the data concerning the identification and preoperative preparation; service requests during their stay in the service; physical and emotional evaluation of the patient in the post anesthesia recovery room; guidelines for conducting the necessary postoperative care for the family member9.
Anxiety is defined as a complex state or psychological condition of the human body, composed of phenomenological properties and physiological that differentiates from emotional states such as stress, threat and fear10.
These events are presented as possible causes of the anxiety state. In addition, anxiety can manifest itself in different ways: as a state or trait. The state of anxiety (A-state) refers to an emotional state or transient condition of the human organism characterized by unpleasant feelings of tension and apprehension consciously perceived, and by an increase in the activity of the autonomic nervous system, generating psychophysiological reactions such as tachycardia, butterflies in the stomach, shiver in spine, among others10.
On the other hand, the trait of anxiety (A-trait) refers to individual differences relatively stable in propensity to anxiety. In general, it would be expected that individuals who have high A-trait showing elevations of A-state, because if the circumstance is perceived as threatening, without object of danger, or is symbolic, nonspecific and advance, the individual responds with a high state of anxiety. However, if the event is perceived as not threatening, the individual reacts with low state of anxiety10.
The people, which differ in A-trait, show or not corresponding differences in the A-state, depending on the degree to which the specific situation is perceived by an individual, in particular, as dangerous or threatening. This is greatly influenced by past experiences of the individual10.
Is understood as the set of transitional anxiety somatic manifestations such as tachycardia, hyperventilation, sweating and psychological manifestations with feelings of apprehension, nervousness, restlessness, and may cause changes in the sleep-wake cycle11.
The concept trait-state is based on the idea of anxiety proposal, where the A-state refers to a passenger emotional state, characterized by subjective feelings of tension, varying in intensity all the time. It is, therefore, an opposite reaction to stress, while the A-trait refers to a relatively stable disposition to respond to stress in this way, with a tendency to perceive the various situations as threatening. Therefore, the A-trait refers to the part of the personality structure of the subject12,13.
METHODOLOGY
This is an analytical and comparative study of quantitative approach to determine the degree of trait and state anxiety accompanying the two groups of children in a surgical situation. The quantitative research allows the measurement of opinions, reactions, habits and attitudes in a universe, by means of a sample that statistically represents them. The main characteristics are: obeys a pre-set plan, with the aim of listing or measure events; uses the theory to develop hypotheses and the variables of the survey; examines the relations between the variables by experimental methods or semi-experimental; usually employs instrumental statistics for data analysis14.
The research was conducted at the outpatient unit (UCAMB) and a pediatric surgery in a University Polyclinic in the city of Rio de Janeiro, from March to August 2012. The UCAMB is a unit of well-equipped surgery with adequate physical and environmental structure, according to current regulations. It has reception rooms, preparation and admission of patients, anesthetic recovery for adults and children, in addition to four surgery rooms and washroom. At the outpatient clinic of pediatric surgery, there are rooms for consultations of a water areas and nursing, in which they are carried out guidelines of nursing directed to the perioperative period, aiming to promote a better care for the patient and the family facing the outpatient anesthesia and surgical procedure.
Data collection occurred through the State-Trait Anxiety Inventory (STAI) of Spielberger, Gorsuch and Lushene, 1970, which has two scales: scale of trait anxiety and state anxiety scale. Each consists of 20 questions and the answers ranged from 1 to 4. The sum of the values in each response ranges from 20 to 80 points and corresponds to the level of anxiety: 20-40 points - low level of anxiety; 41-60 points - average level of anxiety and 60-80 points - High level of anxiety. On the state anxiety scale, 60 scores were reversed, since the content of the statements contained therein were opposite to the statements for the remaining items. They are: 1, 2, 5, 8, 10, 11, 15, 16, 19 and 20 and in the anxiety-trait scale in some items, the scores were also reversed, and they were: 1, 6, 7, 10, 13, 16 and 1913.
The scales are intended to assess anxiety. The state scale requires the participant to describe how you feel now, this time in relation to 20 items presented on a scale of 04 points, among them: no, slightly, fairly and totally. Similarly, the trait scale is also composed of 20 items, but the participant is instructed to respond as it should generally feels, in accordance with a new scale of 04 points: almost never, sometimes, frequently, almost always13.
Given that this is a research involving human beings, the participants were informed about the objectives of the study. Moreover, were informed of the study objectives, ensuring their anonymity as well as total freedom of response, may the subject interrupted data collection at any time, without any damage to you, as required by Resolution 196/96. All interviewees who agreed to participate signed an Informed Consent Form. Inclusion criteria were the companions of children classified as ASA (American Society of Anesthesiology) I and II ASA (American Society of Anesthesiology).
The research project was approved by the Research Ethics Committee of the Pedro Ernesto University Hospital of the State University of Rio de Janeiro, under the opinion No 2920-CEP/HUPE/UERJ.
Data were collected after nursing consultation and the day of surgery, the perioperative period, the group of companions and oriented in the group who were not counseled. The state and trait scale was applied on the day of surgery. The study subjects were composed 100% by mothers and divided into two groups: one composed of companions who received instructions from preoperative (n = 21) nurses and other caregivers who did not receive preoperative guidelines (n = 21).
The quantitative data underwent descriptive statistical treatment and were tabulated and presented in a figure and table.
RESULTS AND DISCUSSION
The collected data refer to the review of the trait and state anxiety of accompanying children who underwent outpatient surgery. Those who received pre-operative nursing guidelines and those not instructed: two groups of caregivers were evaluated. The nursing guidelines were made through a preoperative nursing consultation.
The following trait and state anxiety levels obtained in the two groups studied, with the guidance of nursing and taught without such guidelines are presented.
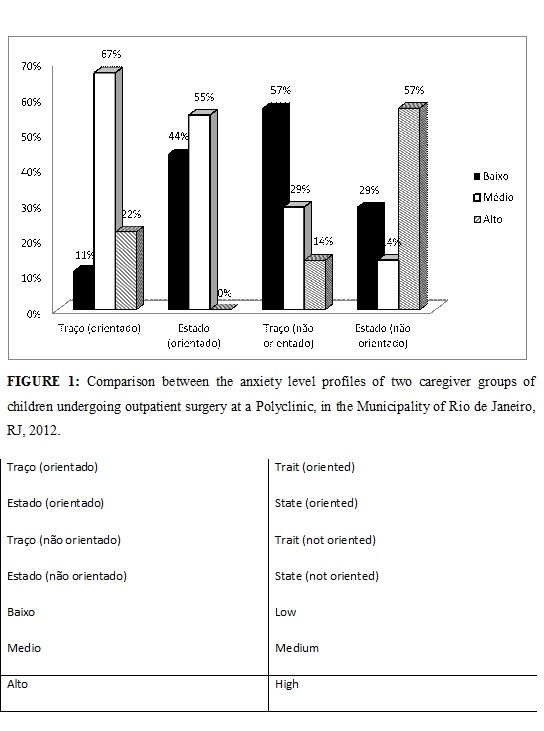
The study subjects were divided into two groups each 21participantes, as previously reported. According to the data presented in Figure 1, the accompanying children who underwent outpatient preoperative nursing, showed a profile more balanced anxiety as trait anxiety was distributed as follows: 02 (11%) with low level, 14 (67%) with an average level and 05 (22%) with a high level of anxiety, but the anxiety showed a low level 09 (44%), 12 medium (55%) and not scoring for the high level of the state anxiety score.
It presents a balance in their anxiety level when comparing the trace of anxiety is the anxiety inherent with state anxiety as a surgical intervention; we observe that high anxiety level was drastically reduced from 22% to 0%. On the other hand, the level due anxiety was reduced from 67% to 55 %, showing that the patients targeted have a lower level of anxiety when comparing trait anxiety with anxiety at the time of tension from the surgery.
Referring to the data of companions who have not passed the nursing consultation, the profile of the level of anxiety, when compared trait and state anxiety, showed an increase of the high levels of anxiety. The anxiety-trait presented the following distribution in their respective levels of anxiety: low 12 (57 %), medium 06 (29 %) and high 03 (14 %); while the anxiety state presented below 06 (29 %), medium 03 (14 %) and high 12 (57%).
We point out that the companions had not driven an increase in the high anxiety levels of 3 (14%) to 12 (57%) and decreased low anxiety levels of 12 (57%) 6 (29%) when compared to trait and state of anxiety. The results show that high levels of state anxiety increased by approximately fourfold when compared trait and state anxiety of non-oriented companions. Thus, it is evident the importance of the nursing orientations to minimize stress levels of the surgical companions.
In a recent study it was demonstrated, a reduction in the anxiety levels of surgical patients who received nursing orientations for preoperative nursing visit, compared with those who received no orientations. Corroborating the importance of nursing in the stabilization and maintenance of anxiety level of surgical patients15.
We can also observe in Figure 1, when compared to the high level of anxiety state of the patients who received preoperative orientations to those who did not receive a reduction in anxiety score from 57% to 0%. These results underscore the importance of childcare and the guidelines of nursing passed during the pre-operative nursing consultation, to minimize the concerns at the time of tension and stress experienced during the surgical time by companions of children undergoing surgery.
The evaluation of emotional and mental performed by nurses shows is becoming increasingly necessary. The identification of emotional problems and mental emerging and/or arising out of hospitalization and illness is of extreme value, since it provides, along with the physical examination, directing the nursing care15.
Both the emotional and mental condition evaluations, the professional should focus their attention on attitudes and the testimony of the patient/family. Therefore, during the data collection attention is directed at the same time, for the behavior of the patient / family, the way of living and the problems and symptoms presented by him and thus get a diagnostic evaluation. Should let the patient / family free to talk about their fears, suffering, and illness, among others. Observe and listen to the patient is essential because it allows them to speak, being available for dialogue.
Before beginning the evaluation, it should be explained to the patient / family their goal and make them aware that this is a way to help in their recovery. Through observation of behavior, symptoms and testimony, the nurse can assess the level of anxiety of the patient / family.
Studies show that the greater the degree of understanding of the patient/family with regard to the information given by the nurse in the pre-operative period, the lower will be the level of anxiety in relation to the surgical procedure, and thus, the better will be their recovery. Therefore, the contact and the information of professional nurses contribute to decrease the uncertainty of the patient/family and provide peace of mind and well-being to them16.
The patient / family is surprised when the illness and need for hospitalization feels unprotected and anxious due to the new conditions experienced.
As the surgeries are scheduled, there is a reasonable period of time for the completion of the pre-surgical suitable, for the range of minimizing the level of anxiety, the surgical stress and eventual postoperative sequels5.
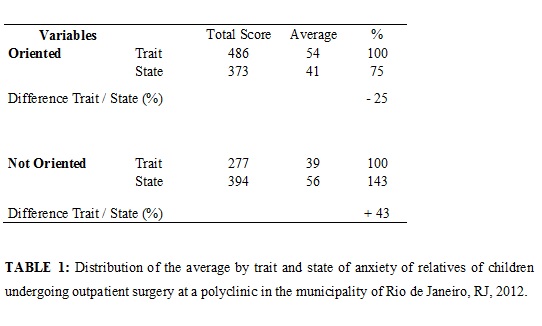
According to the results obtained, the non-oriented companions showed a mean anxiety trait = 39, while anxiety state = 56, i.e. an increase of 43% in the level of anxiety. Oriented companions had an average trait = 54 and average state anxiety = 41, i.e., there was a 25% reduction in anxiety level of these companions, according to Table 1. Therefore, by means of these data, it can be seen that the companions who received orientations on perioperative nursing consultation proved to be less anxious when compared the rates of trait and state anxiety of non-oriented companions. Thus, it is clear the importance of nursing consultation in emotional stability of patients, reducing the level of anxiety of surgical patients.
The nursing consultation aims to guide on the surgical procedure to be performed, the preparation for the surgery, the recovery, and the postoperative care. It enables the reduction of tension, stimulates the self-care, the rehabilitation in the postoperative period and acceptance of treatment. It is a time where the nurse interacts with the patient and family, seeking to solve problems identified by stimulating a humanized care, which contributes to reassure the patient at the time of surgery17.
In accordance with the Cofen Resolution no. 159/93, the nursing consultation is private nurse and through it, you can identify situations of health/disease, schedule and execute measures that contribute to promotion, protection, prevention, recovery and rehabilitation of the individual and family. It is composed by the following steps: nursing history (interview); physical examination, nursing diagnosis, prescription and implementation of nursing care and nursing developments.
The step of the interview is more than a dialog; it requires the professional nurse the ability to listen and understand, to exploit the data that the patient/family brings to demonstrate interest and knowledge, to be receptive. It is necessary to establish a communication favorable for getting good information to inquiries made. It is the first and best opportunity that the patient/family has to expose their feelings; realizing the health condition and circumstances.
As the interview progressed, relationship that is more interpersonal is strengthened, providing fruitful space clearing doubts, covering treatment, routine health facility and establishing joint goals regarding the planning of nursing care.
CONCLUSION
As can be seen, the companions who were told during nursing consultation showed a decrease in anxiety levels, while the group that did not receive perioperative nursing orientations revealed a marked increase in the level of anxiety. With this, it becomes evident the importance of the implementation of the nursing consultation pre-operative to reduce the anxiety of these companions, aiming to provide information to minimize their fears, worries, anxieties and insecurity generated by the surgical procedure, in addition to get important data that should guide the nursing care to be provided.
This study contributes to the nursing staff, in order to emphasize the importance of the nursing consultation pre-surgery, in which the nurse provides guidelines and, through dialog, identifies the level of understanding of the family on the surgery and their level of anxiety. In this way, it is possible to minimize the number of postoperative complications and the suspensions of surgeries, through the implementation of measures such as consultations and visits to nursing pre-operative.
Some of the limitations of this study should be considered which might hinder its generalization of the results, such as the limited number of subjects and the possibility of the socio-cultural variable that may influence the study.
REFERENCES
1. Flório MCS, Galvão CM. Implantação de um serviço de cirurgia ambulatorial: o papel da enfermagem nesse cenário. RevLatino-Am Enfermagem.1998; 6: 83-8.
2. Souza LAM, Rodrigues AAA, Oliveira CR, Araújo CS, Sampaio CEP. Perfil dos acompanhantes das crianças submetidas à cirurgia: contribuições para os cuidados perioperatórios. Revenferm UERJ. 2012; 20: 714-9.
3. Moro ET, Módolo NSP. Ansiedade a criança e os pais. Rev Brasileira de Anestesiologia. 2004; 54: 728-38.
4. Sampaio CEP, Ribeiro DA, Marta CB,Seabra Junior HC, Francisco MTR. Fatores determinantes da ansiedade e mecanismos de cooping em procedimentos cirúrgicos gerais. R. Pesq.: cuidado fundam online, 2013; 5:547-55.
5. Crepaldi MA,Broering CV. Preparação psicológica para a cirurgia em pediatria: Importância, técnicas e limitações. Paidéia. 2008 [citado em 9fev 2013]; 18: 61-72. Available at: http://www.scielo.br/pdf/paideia/v18n39/v18n39a07.pdf.
6. Flório MCS, Galvão CM. Cirurgia ambulatorial: Identificação dos diagnósticos de enfermagem no período perioperatorio. Rev Latino-Am Enfermagem. 2003; 11: 630-7.
7. Souza LR, Souza MAG, Pinto AS, Cortez EA, Carmos TG, Nascimento RM. Os benefícios da visita pré-operatória de enfermagem para o cliente cirúrgico: revisão sistemática de literatura. RECENF.2010; 8: 105-11.
8. Jorgetto GV, Noronha R, Araújo IE. Assistência de enfermagem a pacientes cirúrgicos: avaliação comparativa. RevEletr Enf. [Online] 2005 [citado em 10 fev 2013]; 7: 273-7. Available at: http://www.fen.ufg.br/revista/revista7_3/pdf/original_03.pdf.
9. Sampaio CEP, Leal VMM, Comino LBS, Romano RAT, Gomes AMT. Cirurgia ambulatorial pediátrica: Um estudo exploratório acerca do impacto da consulta de enfermagem. Rev Min Enferm. 2012; 16: 25-30.
10. Gonçalves MP, Belo RP. Ansiedade-traço competitiva: diferenças quanto ao gênero, faixa etária, experiência em competições e modalidade esportiva em jovens atletas. Psico-USF. 2007; 12: 301-7.
11. Garbossa A, Maldaner E, Mortari DM, Biasi J, Leguisamo CP. Efeitos de orientações fisioterapêuticas sobre a ansiedade de pacientes submetidos à cirurgia de revascularização miocárdica. RevBrasCirCardiovasc. 2009; 24: 359-66.
12. Santos MDL, Galdeano LE. Traço e estado de ansiedade de estudantes de enfermagem na realização de uma prova prática. Rev Min Enferm. 2009; 13: 76-83.
13. Fioravanti ACM, Santos LF, Maissonette S, Cruz APM, Landeira-Fernandez J. Avaliação da estrutura fatorial da escala de ansiedade-traço do IDATE.Av Psicol. 2006; 5: 217-24.
14. Polit DF, Beck CT, Hungler BP. Fundamentos de pesquisa em enfermagem: métodos, avaliação, e utilização. Porto Alegre (RS): Artmed; 2004.
15.Frias TFP, Costa CMA, Sampaio CEP. O Impacto da visita pré-operatória de Enfermagem no nível de ansiedade de pacientes cirúrgicos. Rev Min Enferm. 2010; 14: 345-54.
16. Krusei MHL, Almeida MA, Keretzky KB, Rodrigues E, Silva FP, Schenini FS, Garcia VM. Orientação pré-operatória da enfermeira: lembranças de pacientes. RevEletr Enf. 2009;11:494-500.
17. Mendonça RM, Valadão M, Castro L, Camargo TC. A importância da consulta de enfermagem em pré-operatório de ostomias intestinais. Rev Bras de Cancerologia 2007; 53: 431-5.