RESEARCH ARTICLES
Costs of adherence to Acquired Immunodeficiency Syndrome treatment: transversal study
Cristiano Bertolossi MartaI, Joséte Luzia LeiteII, Antonio Augusto de Freitas PeregrinoIII, Vivian SchutzIV, Márcio Tadeu Ribeiro FranciscoV, Carinne MagnagoVI
INurse. PhD in Nursing. Associate Professor of the Department of Nursing of the Federal University of Espírito Santo, Vitória, Espírito Santo, Brazil. Email: cristianobertol@gmail.com
IINurse. Free PhD Titular Professor Emerita by the Federal University of the State of Rio de Janeiro. Permanent Professor at the Postgraduate School of Nursing Anna Nery of the Federal University of Rio de Janeiro. Rio de Janeiro, Brazil. Email: joluzia@gmail.com
IIINurse. Doctor of Public Health. State University of Rio de Janeiro. Institute of Social Medicine. Rio de Janeiro, Brazil. Email: antoniop@uerj.br
IVNurse. PhD in Nursing. Associate Professor of the Department of History and Fundamentals of Nursing of the Federal University of the State of Rio de Janeiro. Brazil. Email: vschutz@gmail.com
VNurse. Adjunct Professor of the School of Nursing of the University of the State of Rio de Janeiro and Coordinator of Undergraduate Nursing of Veiga de Almeida University. Rio de Janeiro, Brazil. Email: mtadeu@uva.br
VINurse. PhD Student in Public Health at the State University of Rio de Janeiro. Institute of Social Medicine. Researcher at the Workstation of Observatory Network for Human Resources in Health Rio de Janeiro, Brazil. Email: carinne.mag@gmail.com
ABSTRACT: This study aimed to value the direct costs of adherence of the porter of the Human Immunodeficiency Virus to the treatment on an outpatient, from the perspective of the Unified Health System and to analyze the cost categories related to treatment adherence in the light of the National Policy of Sexually Transmitted Diseases. Transversal study, conducted in a public health unit in Rio de Janeiro. Data were collected in August 2011, in 100 records, and analyzed using descriptive statistics. Direct costs, which totaled R$ 170,989.06, were divided into three categories: medication, fees for professional and performed examinations, whose total costs absorbed 63.0%, 31.3% and 5.7% respectively of the total. One should broaden the discussion about the distribution of medicaments, the available benefits, and the strengthening of adherence as reduction proposal of direct costs. It is concluded that the policy of care for HIV needs to evaluate the introduction of new technologies and the available resources.
Keywords: Costs; acquired immunodeficiency syndrome; medication adherence; adherence to treatment.
INTRODUCTION
In Brazil, the Acquired Immune Deficiency Syndrome (AIDS, Acquired Immunodeficiency Syndrome) was first discovered in 1982. Its diffusion, in the first half of the 1980s, occurred among the main metropolitan areas, and extended later, to the various micro-regions of the country. During this period, the epidemic affected mainly homosexual and male bisexual, white and middle or upper class, residents of large cities. From the 1990s, heterosexual women and men, children and adolescents, and individuals of all social classes, began to be achieved1.
The creation of the National Program on Sexually Transmitted Diseases (NP-STD)/AIDS has led to change that brought an increasingly technical approach in the discussion of AIDS. The propagation of information and social pressure became decisive factors for the participation of other entities, such as religious, public and private. The coexistence of people with Human Immunodeficiency Virus (HIV, Human Immunodeficiency Virus) culminated in organized movements in order to fight for their legal and human rights2.
The result of these social charges was the distribution of antiretroviral medications (ARV) in primary and secondary levels of health as part of the NPSTD/AIDS. This proposal has reduced the cost of the federal government with hospitalizations. However, with the growing number of people with HIV/AIDS, these expenditures began to grow substantially, putting into question the sustainability of Brazilian politics2.
In the context of the offer of primary level services must pay attention not only to the distribution and access to medicaments, but also for adherence to available treatment. The adherence is a collaborative movement that facilitates the acceptance and integration of a particular therapeutic regimen in daily life in treatment, assuming their participation in the process3,4.
Non-adherence to medicament treatment for AIDS, including ARV, is considered one of the greatest barriers to the effectiveness of therapy and for the dispersion of viral resistance. This, therefore, new therapeutic modalities require the patient's articulation of knowledge, agility and consent, added to environmental factors and care3.
The interaction between the client and the multidisciplinary team is essential for the continued treatment of AIDS5. For this, there must be an investment in primary care (outpatient), since this will be possible to perform activities of promotion, preventive and monitoring shared of therapeutic.
Thinking about these issues, the federal government began to direct the transfer of their funds to specific strategies, such as the program of financial incentives to states, Federal District and municipalities to prevention actions and care qualification on HIV/AIDS and other STD, working since 2007. According to the Ministry of Health (MH), the transfer of funds for this program, of the federal government to the state government of Rio de Janeiro, has declined in recent years (-37.8%). This reduction was greater than the perceived in the analysis of the total transfer of funds to health (-30.5%) over the same period6.
Given the above, it was defined as an object: the direct costs to measure the costs of adherence to AIDS treatment on an outpatient level in the perspective of the Unified Health System (UHS). And as objectives: to assess the direct costs of AIDS treatment adherence, in outpatient and; to analyze the cost categories related to this adhesion in the light of the National Policy of STD/AIDS.
The study is relevant for the assistance, because it may subsidize a change in the vision about health policies and its priorities, and encourage nurses to strengthen their managerial/administrative identity, without losing the care focus.
It is also relevant to the research, because will stimulate the reflection about the optimization of resources and practices aimed at this clientele; and teaching, will aim building thoughts more suited to the reality and demands of the health care market and its demand for financial resources.
LITERATURE REVISION
The cost represents the value of inputs (capital, work, materials, devices, medicaments, and others) used in the production or distribution of assets or services7.
Studies of the cost of the disease (SCD) are studies of descriptive nature, aimed at specifying for items, to assess and quantify the costs of a disease, in order to give an idea of its economic impact and estimate the maximum amount that could be saved or won, if it had been eradicated7.
Traditionally, SCDs examine the direct and indirect costs. The direct ones represent the value of resources used in the treatment, care and rehabilitation of individuals, may be medical or non-medical. In the indirect, figure the value of lost economic resources due to productivity lost, disability or premature death related to the patient or even family/caregivers. While the direct measure the cost of the resources opportunity used to treat the disease, the indirect indicate the cost opportunity of lost resources8,9.
METHODOLOGY
This is a transversal study, developed in a public health unit, referral for outpatient treatment of clients with AIDS, in the municipality of Rio de Janeiro, in which approximately 1000 HIV/AIDS clients make accompaniment.
To select the sample of eligible records, the following inclusion criteria were established related to patients accompanied by unit: aged equal or greater than 18; with a definite diagnosis of AIDS according to the evaluation criteria of MH; to possess minimum of 24 months of outpatient follow-up, i.e., accompaniment beginning in or prior to July 2009; taking ARV; and have attended the unit between July and August 2011, period which the data were collected. Exclusion criteria were elected: client participants for clinical trials in the last 12 months; pregnant women or women in the postpartum period. After applying the aforementioned criteria, the study population consisted of 100 registered clients and treated at the clinic.
The technique of documentary analysis of charts was employed, and developed with the aid of a form. The data related to the direct costs of treatment adherence of individuals were used, produced between July and December 2009.
Direct costs considered in this study were those arising from the effective use of resources in interventions and health programs 9, specifically: complementary exams, medicaments and professional fees (nurses, doctors, psychologists, nutritionists and social workers).
The calculation of the direct cost is based on the assumption that health actions are composed of a set of procedures that employ fixed combinations of inputs. The identification of the quantities of inputs, used in a particular intervention or health program, involves collecting such amounts for each action developed by health professionals at the time of the service to each client9.
The data relating to direct costs were subdivided into cost categories and its values acquired through the use of formulas.
The medication had it cost estimated by the MH of the Popular Pharmacy Program Table 6, and the total cost was calculated using the following formula:
Total cost of medication = (Cost of medication per dose) x (number of doses/day) x (number of days of use)
The values relating to human resources were based on data presented in the fees table of the Federal Councils of each profession. It was used the following formula:
Total cost of human resources = (amount per hour of developed action) x (number of hours/day) x (number of days)
The examinations were rated according to the table of the Popular Pharmacy of MH. The used formula was:
Total cost of exams = (unit value of each exam) x (amount/day) x (number of days)
After collecting and organizing data, they were submitted to descriptive statistics to present the results with the support of Microsoft Excel® program 2010.
The research respected the precepts of Resolution No. 196/96. Thus, the project was submitted to the Ethics Committee and Research of the Nursing School Anna Nery/São Francisco de Assis Teaching Hospital (EEAN/SFATH) for evaluation and was approved on May 31, 2011, under protocol number 018/2011 .
RESULTS AND DISCUSSION
Regarding the profile of the subjects, it was found that the majority (64%) were males aged between 38 and 47 years (37%), followed by those aged between 28 and 37 years (25%).
The data relating to the profile of individuals are coherent to those disclosed by MH, in 2010, which showed the highest prevalence of HIV/AIDS among those aged between 40 and 59 years (37.9%), followed by those aged 30 and 39 years (33.8%) and 20 to 29 years (21.0%)1,10 .
Direct costs related to adherence to AIDS treatment
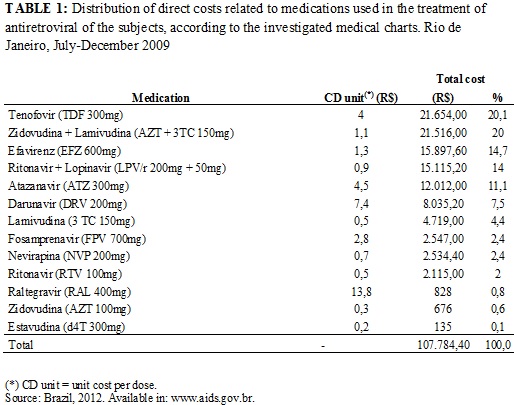
Direct costs were divided into three categories: medication, fees for professional and examinations conducted over six months, and the estimated total costs were: R$ 107,784.40 (63.0%), R$ 53,542.38 (31.3%), R$ 9,662.28 (5.7%), respectively. Thus, the sum of direct costs was equal to R$ 170,989.06..
The costs estimated in this research corroborate the findings of research conducted in the State of São Paulo, which revealed that the ARVs were responsible for 62% of the total cost of outpatient treatment for HIV/AIDS, followed by expenditure on other medicaments and professional care costs. This same study compared the Brazilian costs with those of other countries, and proved that the Brazilian spent on the treatment of HIV, was 6.4 times lower than the expenditure of the USA, whose therapeutic regime is funded by the own patients. Consumption of Mexico, whose treatment is also offered free of charge, was 2.0 times higher than Brazil; while the costs of Haiti and South Africa were 2.0 and 2.6 times lower, respectively11.
Medicament costs
Among the used medications, those that represented the higher unit costs were: Raltegravir (R$ 13.8) and Darunavir (R$ 7.44). However, those that gave higher total expenditure, given its greater use were Tenofovir, Zidovudina (AZT) associated to Lamivudina, Efavirenz, and Ritonavir associated to Lopinavir. Together, accounted for almost 70.0% of medicaments spending. AZT and Estavudina, in turn, are those with lower unit values and were also the least prescribed, as shown in Table 1.
With regard to medications that were more prominent used, they have characteristics which favor the reduction of the number of pills and medications, as they combine the effects of one or more drugs in a single tablet or act as enhancers when ingested concomitantly. This action reduces the risk factors for treatment and, consequently to treatment adherence6,12.
Risk factors related to treatment have been identified in the literature as factors that may contribute to the reduction of adherence to treatment. Among them we have two considered most important: the time and complexity of treatment. In the first case, the concern is directed to the prolonged adhesion, since the non-adhesion increases with time of treatment. The complexity of treatment refers to the number of doses of drugs12, the side effects and changes in lifestyle as the cause of non-adherence13.
Given these data, it is noticed that the substances that make the medicaments, pharmacodynamics and pharmacokinetics also have importance in determining the costs of the program, as they influence treatment adherence which is directly related to the cost of the process as a whole. The abandonment, misuse or non-suitability for medicament therapy can generate even higher costs. ARV therapy is inclined to neutralize the high capacity of multiplication, adaptation and mutation of the virus, but if medicaments are not used correctly, with interruptions (without adherence), the effectiveness and efficiency of therapy are hindered. In addition, there is the possibility of non adherence create resistant strains that, certainly, will be the protagonists of new features request to exchange medicaments and new studies.
Costs of professional fees
The costs of professional fees are related to paid activities developed as determined by the respective Federal Councils. It is noticed that these values are moderate costs when evaluating the complexity of reality in which they are inserted.
It is found that the total cost of the procedures, performed in the implementation of care for subjects in the research was R$ 53,542.38, being distributed in a multidisciplinary way, according to the data presented in Table 2.
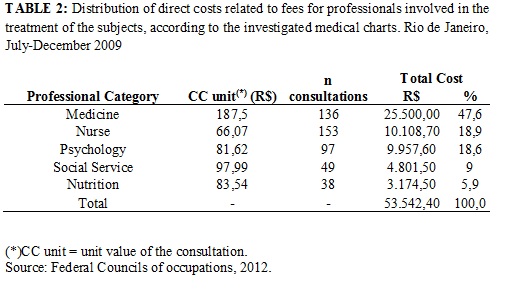
It is noted that the unit cost, as well as the summation of the consultations is greatly superior to that of other professional categories, although the largest number of consultations have been performed by nurses, which represent uniformly lower cost than the others.
A positive factor for adherence to AIDS treatment was the investment in professional care in a multidisciplinary way, although the number of visits has varied according to professional category.
It is noticed that the consultations have different values, so that some correspond to more than triple of the value of others, such as nursing consultation, which has the lowest value among the group of professionals who compose the multidisciplinary team. It is believed that such an occurrence constitutes a difficulty in perception, on the part of the representatives of councils and/or managers responsible for maintaining the Brazilian health care programs, about professional development, according to Table 2.
It reinforces that, commitment to assist those porters of HIV/AIDS, nurses, via nursing consultation, provides an opportunity to work toward improving the quality of life and is responsible for preparing the client for self-care14,15.
Individual and integral care, established in the relationship between nurse and client corresponds to an effective strategy for improving adherence to therapy regime. For this relationship to be effective, must be established feelings of safety, empathy, and respect for customer privacy. Professionals should adopt a posture that gives credibility, believing, especially in information and behaviors emanating the client15,16.
Moreover, the satisfaction with social support and the use of active behavioral coping strategies are associated with adherence in HIV-infected clients. Social support is highlighted by its influence both directly – providing encouragement and motivation for self-care – and indirectly, to mitigate the effects of situations that interfere negatively on adherence. In this scenario inserts the self-esteem variable, since feelings of worthlessness can sponsor the neglect of health17,18.
In this context, professional assistance is an essential determinant to achieve the success of programs aimed at chronic diseases, such as AIDS. The actions of care, if well led and managed, can impact positively on indicators of health and quality of life of clients and cooperate for obtaining epidemiological control and adherence to therapy5.
The universality, achieved with the institution of the UHS, and in the case of the AIDS epidemic, with the offer of free assistance and medicaments to treat the disease, has impacted greatly to effective health policies aimed at improving the quality of life of people living with the disease19.
However, for the effects of universal health persist, they should be articulated to the achievements of professional performance in all its ever-increasing technological complexity. This complexity is expressed in the actions of aid care, management, interdisciplinary and the incorporation of new knowledge, practices and technologies19.
Adherence to the treatment regimen also involves the articulation of diverse and different technologies, such as offering support groups for discussion of adherence, which incorporation in the work process, should be guided by scientific evidence reported in the literature. Studies performed in Brazil have shown the critical importance of treatment initiation to adherence, as well as the main influencing factors for adherence to the therapeutic regimen, which can support the decision making of professional racing in the adoption of strategies to encourage the patient5,19.
In the process, we must stress the subjectivity, the needs and difficulties of the patient, considering that the complex behavioral determinants of non-adherence are difficult to understand12,20.
Given the above, it is perceived that health services are seen as strategic information spaces and execution interventions in the field of adherence, among which includes the availability of information about the importance of treatment adherence and adequacy to the routine of life client, and clinical care to treatment toxicity and the management of chemical dependency.
Health professionals, articulated in multidisciplinary teams, should keep in mind that to achieve a treatment with effectiveness, one must seek an alliance with the client. In this process of co-responsibility, exists also, a family and social network, that directly and indirectly contribute to the success or possible treatment failure. It is also important to recognize that adherence is an act of dynamic character, being constantly stimulated21.
Examinations costs
The research of the costs resulting for carrying out exams for monitoring the therapy, it is noted that the sum of costs (R$ 9,662.28), most part came from the quantification of viral load (22.7%), and CD4+ cells (19.4%) and CD8+ (19.4%), which were demanded greater number of times. However, the more expensive exams, in relation to the unit costs, are related to the investigation of hepatitis A, B and C (R$ 18.60, each), which were less frequently requested.
According to the data exposed about the costs related to laboratory exams, it is seen that within the analyzed group, in which treatment adherence was constant, the need for evaluation of other complications was reduced, being ordered in large measure, exams that show the presentation level of the virus in the blood and the number of affected defense cells. These data certainly demonstrate the influence and importance of adherence in the costs of the process. Because, besides presenting the reduction of costs with the exams realization of other opportunistic diseases, also reinforces the idea that adherence helps to reduce costs with other medications for treatment of opportunistic diseases or from low immunity.
It should be emphasized, that the triad evaluated in this study, the category related to exams costs, was the least expensive. Although it is expected that the costs of examinations may be even smaller, considering their larger scale production.
According to data from the MH, the federal government provides to health care a value corresponding to R$ 2,123,317,369.53 per year. Of this amount, R$ 1,048,355,764.00 are dedicated to the NP-STD/AIDS. In 2009, the transfer from the federal government to the government of the State of Rio de Janeiro was the order of R$ 2,318,669,071.46, being R$ 1,009,976,602.30 to health. Of this total, R$ 2,526,614.34 (0.25%) were allocated to the State Program of STD/AIDS6,22.
In the setting of this study, which is a reference institution for the treatment of HIV/AIDS, the direct costs (medication, examinations and fees of professionals) was approximately of R$ 170,989.06, during the second half of 2009 (July-December) . If we consider a year of treatment and using the same medications and doses consumed in the semester of the search, we could double the semiannual value mentioned above, assuming a total of R$ 341,978.12. This value corresponds to 13.5% of budget allocated to HIV/AIDS in the State of Rio de Janeiro.
CONCLUSION
The evaluation found that direct costs, even after the acquired conquests – patent infringement – by the federal government, the cost with medications is presented as the highest among the other categories, since the number of people on treatment increases every year due to the expansion of the life expectancy of this clientele.
It should pay attention to adherence treatment, especially the proper use of ARVs, used to combat a retrovirus - microorganism with high power mutation. Thus, the misuse of ARVs may generate resistant strains. These new strains, in medium and long term may render the NP-STD/AIDS unsustainable, as the State should have the largest contingent of financial resources to invest in the production of higher number of medications, new studies and drugs, in order to meet the new demand of carriers of this resistant strains.
Another important factor identified was the relatively low cost of the laboratory exams. The defendants exams had, mostly, the objective to evaluate the control of viral load of clients and evaluation of the effectiveness and efficiency of used medicaments. As the purpose of this study was to collect information from clients with 24 months or more of treatment, obtained an adherence fee of 100%, thus not having a high cost in relation to screening for opportunistic diseases. Thus, it appears that adherence reduces the costs of AIDS treatment.
Given these factors, it can be stated that the policy of care for HIV porters, has important strategies, such as directions of funds to enable the inclusion of these subjects in the flow of outpatient care, trying to minimize their setbacks, limitations and valuing their expertise and values that stimulate life and well-being as a human being. However, it needs to establish a constantly review of its processes for introducing new technologies and update their available resources.
REFERENCES
1. Ministério da Saúde (Br). Secretaria de Vigilância em Saúde. Departamento de DST, AIDS e Hepatites Virais. Controle das AIDS e DST. Brasília (DF): Ministério da Saúde; 2011.
2. Lago RF, Costa NR. Dilemas da política de distribuição de medicamentos antirretrovirais no Brasil. Ciênc saúde coletiva [Scielo - Scientific Electronic Library Online] 2014 [citado em 01 mai 2014]. Available at: http://www.scielo.br/scielo/prc.
3. Ministério da Saúde (Br). Secretaria de Vigilância em Saúde. Departamento de DST, AIDS e Hepatites Virais. Adesão ao tratamento antirretroviral no Brasil: coletânea de estudos do Projeto Atar. Brasília (DF): Ministério da Saúde; 2010.
4. Cavalari E, Nogueira MS, Fava SMCL, Cesarino CB, Martin JFV. Adesão ao tratamento: estudo entre portadores de hipertensão arterial em seguimento ambulatorial. Rev enferm UERJ. 2012; 20(1):67-72.
5. Ministério da Saúde (Br). Programa Nacional de DST/AIDS. Manual de adesão ao tratamento para pessoas vivendo com HIV e AIDS. Brasília (DF): Ministério da Saúde; 2008.
6. Ministério da Saúde (Br). Programa Nacional de DST/AIDS. [site da internet]. Brasília (DF): Ministério da Saúde [citado em 13 jun 2012]. Available at: http://www.AIDS.gov.br.
7. Costa AMN, Secoli SR, Nita ME. Avaliação econômica: análise de custo-minimização, análise de custo-consequência, estudo de custo da doença e outras análises parciais. In: Nita ME, Secoli SR, Nobre MRC, Ono-Nita SK, Campino ACC, Sarti FM et. al. Avaliação de tecnologias em saúde: evidência clinica, análise econômica e análise de decisão. Porto Alegre (RS): Artmed; 2010. p. 354-67.
8. Drummond MF, Sculpher MJ, T orrance GW, O’Brien BJ, Stoddart GL. Critical assessment of economic evaluation. In: Drummond MF, Sculpher MJ, Torrance GW, O’Brien BJ, S toddart GL, eds. Methods for the economic evaluation of health care programmes. New York: Oxford University Press, 2005, p. 27-54.
9. Nita ME, Secoli SR, Nobre MRC, Ono-Nita SK, Campino ACC, Sarti FM et. al. Avaliação de tecnologias em saúde: evidência clinica, análise econômica e análise de decisão. Porto Alegre (RS): Artmed; 2010.
10. Arduini JB, Santos AS. A percepção do homem idoso sobre sexualidade e AIDS. Rev enferm UERJ. 2013, 21:379-83.
11. Sarti FM, Nishijima M, Campino ACC, Cyrillo DC. A comparative analysis of outpatient costs in HIV treatment programs. Rev Assoc Med Bras. [Scielo - Scientific Electronic Library Online]. 2012 [citado em 12 jun 2013]. 58: 561-7. Available at: http://www.scielo.br/pdf/ramb/v58n5/v58n5a13.pdf
12. Colombrini MRC, Coleta MFD, Lopes MHBM. Fatores de risco para a não adesão ao tratamento com terapia antirretroviral altamente eficaz. Rev esc enferm USP. 2008; 42:490-5.
13. Rodrigues CS, Guimarães MDC, Acurcio FA, Comini CC. Interrupção do acompanhamento clínico ambulatorial de pacientes infectados pelo HIV. Rev Saude Publica. 2008; 37: 183-90.
14. Sampaio Filho FJL, Gubert FA, Pinheiro PNC, Martins AKL, Vieira NFC, Nóbrega MFB. The life of the adolescent with HIV/AIDS and self-care: a descriptive study. Online braz j nurs [Internet]. 2013 [citado em 01 abr 2013]. 12: 89-105. Available at: http://www.objnursing.uff.br/index.php/nursing/article/view/3812
15. Santos EI, Gomes AMT, Oliveira DC, Santo CCE. Entre sofrimento e prazer: a vulnerabilidade para enfermeiros nas relações interpessoais com pacientes com HIV/AIDS. Rev enferm UERJ. 2013; 21:9-15.
16. Figueiredo RM, Sinkoc VM, Tomazim CC, Gallani MCBJ, Colombrini MRC. Adesão de clientes com AIDS ao tratamento com antirretrovirais: dificuldades relatadas e proposição de medidas atenuantes em um Hospital Escola. Rev Latino-Am Enfermagem. 2011;9: 332-45.
17. Lima ACB, Guerra DM. Avaliação do custo do tratamento de úlceras por pressão em pacientes hospitalizados usando curativos industrializados. Ciênc saúde coletiva. 2011;16: 45-56.
18. Silva IJ, Oliveira MFV, Silva SED, Polaro SHI, Radünz V, Santos EKA, et al. Care, self-care and caring for yourself: a paredigmatic understanding thought for nursing care. Rev esc enferm USP [Scielo - Scientific Electronic Library Online]. 2009 [cited in 2010 Aug 17]. 43: 697-703. Available at: http://www.scielo.br/pdf/reeusp/v43n3/a28v43n3.pdf.
19. Ministério da Saúde (Br). Secretaria Executiva. Área de economia da saúde e desenvolvimento. Avaliação econômica em saúde: desafios para gestão do Sistema Único de Saúde. Brasília (DF): Ministério da Saúde; 2008.
20. Pinto ACS, Fiuza MLT, Pinheiro PNC, Vieira NFC, Galvão MTG. Life experiences of HIV/AIDS carriers in terms of the perspectives of the promotion of health. . Online braz j nurs [periodic online]. 2012 [cited in 2012 dez 02]. 11: 815-28. Available at: http://www.objnursing.uff.br/index.php/nursing/article/view/3650
21. Bertolozzi MR, Nichiata LYI, Takahashi RF, Ciosak SI, Hino P, Val LF, et al. The vulnerability and the compliance in Collective Health. Rev esc enferm USP [Scielo - Scientific Electronic Library Online]. 2009 [cited in 2010 Mar 15]; 43:1326-30. Available at: http://www.scielo.br/pdf/reeusp/v43nspe2/en_a31v43s2.pdf
22. Hallal R, Kuchenbecker R, Ravasi G, Simão MA, Greco D. Access to antiretroviral treatment in Brazil. Revista Tempus. Actas em Saúde Coletiva. 2010; 4(2):53-65.