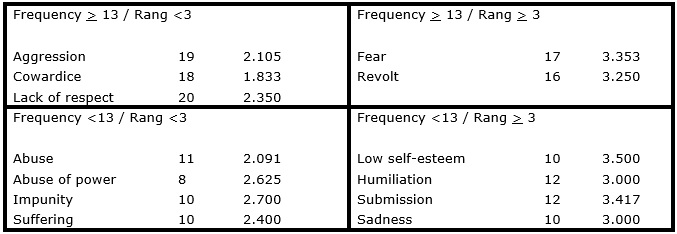
FIGURE 1: Four-quadrant frame of the representational structure of NT and CHW younger than 41 years about domestic violence against women. Rio Grande/RS, Brazil, 2014
ORIGINAL RESEARCH
Representation of the domestic violence against women between health professionals: age as an attribute of differentiation
Camila Daiane SilvaI; Vera Lúcia de Oliveira GomesII; Denize Cristina de OliveiraIII; Cristiane Lopes AmarijoIV; Daniele Ferreira AcostaV; Marina Soares MotaVI
I
Nurse. MSc in Nursing. PhD student at the Graduate Program in Nursing.
Member of the Group of Studies and Research on Nursing Gender and Society.
Federal University of Rio Grande. Rio Grande, Rio Grande do Sul, Brazil.
Email: camilad.silva@yahoo.com.br
II
Nurse. PhD in Nursing. Full Professor. Leader of the Group of Studies and
Research on Nursing Gender and Society. Tutor of the Tutorial Education
Program in Nursing. School of nursing. Federal University of Rio Grande.
Rio Grande, Rio Grande do Sul, Brazil. E-mail: vlog1952@gmail.com
III
Nurse. PhD in Public Health. Professor of the Graduate Program in Nursing
and of the Graduate Program in Social Psychology at the University of the
State of Rio de Janeiro. University of the State of Rio de Janeiro. Rio de
Janeiro, Rio de Janeiro, Brazil. E-mail: dcouerj@gmail.com
IV
Nurse. MSc student of the graduate program in nursing. Member of the Group
of Studies and Research on Nursing Gender and Society. Federal University
of Rio Grande. Rio Grande, Rio Grande do Sul, Brazil. Email:
cristianeamarijo@yahoo.com.br
V
Nurse. PhD student at the Graduate Program in Nursing. Member of the Group
of Studies and Research on Nursing Gender and Society. Federal University
of Rio Grande. Rio Grande, Rio Grande do Sul, Brazil. Email: nieleacosta@gmail.com
VI
Nurse. MSc in Nursing. Member of the Group of Studies and Research in
Nursing and Health of Children and Adolescents. Public Employee of the
Health Department of the Municipality of Turuçu, Rio Grande do Sul, Brazil.
Email: msm.mari.gro@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2016.13212
ABSTRACT
Objective: qualitative study that has objected to compare, by the age, the social representation of domestic violence against women between Nursing Technicians and Health Community Agent, acting on the Health Family Unit, in the extreme south of the country. Data were collected, between July to November 2013, by free evocation and interviews, being treated by evoc software and content analysis. Were totalized 86 professionals with less of 41 years and with 68 professionals with 41 or more years. Booth age range was a structured representation, with negative connotative, presenting in our central cores, the aggression elements and lack of respect. The youngers still evocate cowardice and, on the contrast zone, impunity; those whit more age evocate also fear and abuse and, on the second circuit, alcoholism, addiction and lack of dialogue. Perceives that is a differentiation on the representation by the age. It is understood that this occurs by the conviviality for many years whit the no criminalization of violence.
Keywords: violence against women; domestic violence; health personnel; nursing.
INTRODUCTION
Domestic violence against women (DVAW) is conceptualized by the Law nº 11.340/2006, known as Maria da Penha Law (MPL) as "any act or conduct, based on gender that causes death, or physical, sexual or psychological damage to women, whether in the public or the private sphere"1:1 . This form of violence has historically been neglected and restricted to the private sphere, gaining more visibility only in recent decades 2.
The Brazilian Penal Code and the Civil Code of 1916, which prevailed until 2002, used to reinforce the patriarchal patterns of society3. With regard to the duties and legal rights of men and women, it was assigned to men the role of head of the marital society, while women had the responsibility to collaborate in the common interest of the couple and their children3. Thus, cultural patterns were taking roots, over the generations, as natural and invigorating gender differences.
The DVAW began to gain visibility from the feminist movements in the 1980s 4. At that time, protests began to express the awareness of society about the role of women, their rights and their spaces for action, as well as the neglect of the judiciary power before cases of feminicide, justified by legitimate defense of honor5.
From this framework, issues of equality, women's rights and an end to gender-based violence were being problematized more emphatically and conquests were achieved. Among these is the amendment of the Civil Code by Law 10406/2002, in which the term man was replaced by person3. Still, with the creation of MPL, a new scenario is expected in relation to combating and preventing DVAW and punishing the offender. Before the law was enacted, the actions of attackers, when judged, were regarded as a crime of minor offensive potential and treated as traffic offenses and arguments between neighbors 6. The punishment consisted in the payment of basic-needs grocery packages in charities7as well as in community service 6.
The MPL, besides recognizing different types of violence within the home or by anyone who is considered a family member, establishes the flagrant and preventive prison of the aggressor, as well as the urgent protective measures, inclusion of the victims in the official social assistance programs and the care from articulated network services, including health, security, justice, social welfare, education, housing and culture1. Nevertheless, Brazil has the seventh place in the ranking of countries with high rates of femicide8. It is noteworthy that only 35% of victims of domestic violence makes an official complaint9. Among the reasons for not doing the complaint is the fear of suffering even worst attacks from the offender 9, social prejudice due to judgment of others, emotional and financial dependence on the abuser, the sense of guilt for what happened and the embarrassment to expose the situation to others5.
Many of the victims seek health services for immediate or delayed treatment of injuries resulting from the violence suffered, although they do not reveal the real situation. Thus, Family Health Units (FHUs) have a privileged position, due to its interface with the social aspect, to detect DVAW, constituting a propitious space for the reception of victims 10,11.
These units have multidisciplinary teams composed of at least one doctor, one nurse, one nursing technician and six community health workers. These teams follow, on average, three thousand inhabitants, developing health promotion, prevention, maintenance, recovery and rehabilitation 12.
The approach of these professionals with the community may function as a facilitating factor to the detection of cases of violence10. Therefore, it is necessary to understand the DVAW as a multifaceted phenomenon, breaking cultural stereotypes or preconceptions that may permeate the care of victims.
Considering that professionals from USF, especially nursing technicians (NT) and community health workers (CHW) experience the family life, as they routinely perform home visits, and considering also that age may interfere with the representation of DVAW as this is influenced by the historical and cultural context, and that the DVAW phenomenon is reproduced in a intergenerational manner, we set the aim to investigate: which is the social representation of VDCM of different age groups among NTs and CHWs. This study aims to compare, according to age, the social representations of DVAW among TE and CHW who are active in family health units, in the extreme south of the country.
THEORETICAL FRAMEWORK
The Theory of Social Representation (TSR) constitutes a set of concepts, propositions and explanations originated in daily life that are intended to interpret and elaborate the real life13.
However, for a representation to gain meaning, it is necessary that the object be shared and celebrated by the group, because the analysis does not focus on the individual, but in the phenomena produced by the particular constructions of reality. The choice for TRS was due to its increasingly explicit proximity with the object of study. Knowledge of DVAW is acquired by experience in the scope of work of the subjects of this study and by the information and cultural-historical models experienced in society.
From the perspective of the Central Nucleus Theory, complementary approach to the TRS, the representations have elements subject to a hierarchical structure formed by systems of meaning, which can be arranged by the technique of the Four-Quadrant Frame, which forms a framework in which the upper left quadrant is located the central core, which determines the meaning and organization of the representation; it is essentially social, connected to the collective memory and history of the group, is insensitive to the immediate context and stabilizer of the representation 14,15. In the lower left quadrant are the contrasting elements; and, in the superior and lower right quadrants, the elements of first and second peripheries, respectively. The Peripheral System consists of elements that are organized around the central core; are affordable, flexible, concrete, evolutionary and sensitive to the immediate context. They are more associated with individual characteristics, allowing for the heterogeneity of the group14,15. The construction of the frame is derived from the Test of Free Association of Words, or the Free Evocations produced from an inductive term, allowing the seizure of mental projections spontaneously and the revelation of content that could be vested in speeches16.
METHODOLOGY
Descriptive and qualitative study based on the TRS, conducted in 12 FHUs located in the urban area and seven in rural area of the municipality of Rio Grande/RS, Brazil. A total of 40 NTs and 178 CHWs. Those absent for sick leave or on vacation and those who refused the invitation were excluded. Data were collected between July and November 2013, by the techniques of free evocations and interviews.
One hundred and fifty-four professionals participated in the evocations. They were invited to verbalize the first five words recalled at the inductor term "domestic violence against women". This technique allows the seizure of cognitions in a relaxed and spontaneous way, and create opportunities to obtain the meanings through fast and objective chaining, facilitating the evocation of discursive expressions16.
There is a consensus among TRS theorists that 30 interviews is the minimum necessary for recovery of cognitive and social construction about an object 17. In order to select respondents, a map with the location of the FHUs was elaborated. The proximity between the units was adopted as a criterion because it is assumed that this is conducive to the building of similar social representations. Thus, the map was divided into four urban areas covering 12 FHUs and six rural areas with seven FHUs. It is noteworthy that the distance between the latter prevented larger grouping. After that, one FHU was randomly chosen by each delimited area, and at least one NT and two CHW were invited, totaling 39 professionals. They were invited because, unlike the nurses and doctors, they had no higher education. A script with open questions that led to better understanding of the general perception of DVAW was built for interviews, as well as for survey care practices focused on victimized patients, ethical and legal aspects of care, notification and difficulties in executing it. Also, a possible experience of the situation of violence in the family environment, as well as the conduct adopted, was investigated. All were held in private rooms at FHUs and had an average duration of 40 minutes, were recorded and transcribed in full-length.
The software Ensemble des Programmes Pemettant L'Analyse Evocations (EVOC 2005) for evocations was used in the treatment of data, allowing the construction of the four-quadrant frame, proposed by Pierre Vergès. For the processing of data obtained in interviews we used the Context Analysis18. This has the purpose to identify the context in which the words contained in the above four quadrants were employed, using phrases to exemplify the representations obtained.
Seeking anonymity, the speeches of nursing technicians were identified by NT and community health workers by CHW. The project was approved by the Ethics Committee of
the Federal University of Rio Grande/RS, under Opinion nº 020/2013.
RESULTS AND DISCUSSION
The ages of the 154 respondents ranged from 24 to 65 years, ant the average was 41 years. Two categories were created: bellow 41 years old, with 86 informants, and older than or equal to 41 years old, with 68 informants. The corpus formed by evocations of professionals bellow 41 years, at the inductive term "domestic violence against women" summed 427 words, with 149 different words. The average of the mean orders of evocation (M.O.E.) was 3; the minimum frequency, 8; and the average frequency, 13. The analysis of this data set resulted in the four-quadrant frame, as Figure 1.
FIGURE 1:
Four-quadrant frame of the representational structure of NT and CHW younger
than 41 years about domestic violence against women. Rio Grande/RS, Brazil,
2014
O corpus formed with the evocations of professionals aged bellow 41 years accounted for 340 words, with 148 different. The average of the mean orders of evocation (M.O.E.) was 3; the minimum frequency, 8; and the average frequency, 13. The analysis of this data set resulted in the four-quadrant frame, as Figure 1.
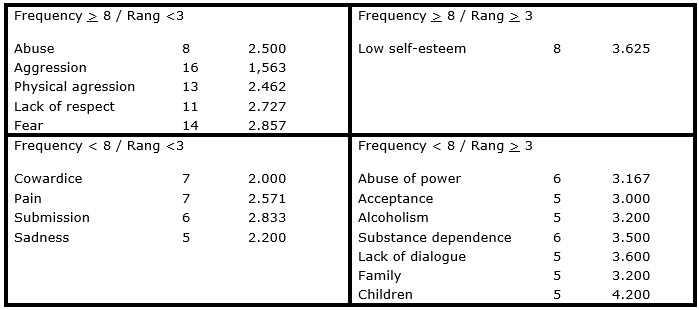
FIGURE 2:
Four-quadrant frame of the representational structure of NT and CHW older
than or equal to 41 years old about domestic violence against women. Rio
Grande/RS, Brazil, 2014
It must be considered that "it is the identification of the core nucleus that allows the comparative study of representations" and that "for two representations be different, they must be organized around two different central cores"19:31. Otherwise, they are "differentially activated states of the same representation in function of the specific situations in which the two groups are"20:77.
It was found that the two groups have a representation with negative connotations and variations according to age. They have in common, in the core, the terms aggression that refers to the image or concept and lack of respect, that identifies how professionals judge DVAW. In this regard, it is noted that both representations have the three dimensions forming a social representation, that is, the content, the image and the judgement21.
It is noteworthy that the terms aggression and lack of respect are functional and regulatory elements, respectively14. The regulatory elements refer to the values of the subject, giving a fundamentally social dimension to the core. In turn, functional elements are associated with descriptive characteristics and description of the object in social practices, determining the behavior of health professionals toward the object14.
Youngest professionals have also in the central core of their representation, less frequently and readily evoked, another regulatory element, cowardice, reinforcing the judgments of this group in relation to DVAW. Also reinforcing judgements, the oldest group has the term abuse in the core. In this group, there is still the term physical aggression, showing that professionals recognize forms of DVAW, distinguishing the physical form from other forms. This term also expresses the image they have of the violent act, probably by the apparent marks on the victim's body22, that is, they recognize violence in their routine work only when this is explicit. In this sense, a survey conducted in the region of action of these NT and CHW, found that 47.7% of the records of violence in a Police unit specialized to assist women referred to the physical form of violence23.
It is noteworthy that the term fear is present in the core of the oldest group, due to their greater experience, may be related both to the victim, as to the professional. The victim inhibits the realization of the complaint and, for the professional, the fear of retaliation is a hindrance to take action. On the other hand, this term is relocated to the first periphery in the youngest group, showing that this feeling is more intense for the oldest group. This is associated to the lack of legislation with punitive measures against aggressors and protective measures for the victims of violence by the year 2006. With the enactment and wide dissemination of the MPL, health professionals possibly began to feel greater legal support for their operations, reducing the feeling of fear. The following excerpts show the discursive context of these terms in the four-quadrant frame.
I think that violence against women is an abuse, an aggression, it lack of love. Violence against women is a lack of respect, a useless act of aggression. (NT)
She said that every time the fellow comes home drunk and she'll comment on something, she is beaten, this is cowardice. (NT)
If they know exactly who was, you cannot continue working. You work in an environment that has many social situations and types of thoughts, and working with fear you cannot do anything. (CHW)
We tried to explain that they have to report that, but to no use. They are afraid. (NT)
The contrasting elements are located in the lower left quadrant, which are also considered important, and possibly reinforce the ideas contained in the central core or reveal the existence of a minor sub-group having a different representation16. The youngest participants evoked in this area the term abuse more frequently and readily, reinforcing the judgements of these professionals in relation to the actions of the offender. They also mentioned abuse of power, impunity and suffering. The probable existence of a subgroup among the youngest group was observed, which has its representation in a variation, listing the term impunity, possibly recognizing that offenders should receive adequate punishments for the DVAW practiced, supported by the MPL1.
Oldest professionals evoked in the contrast zone terms such as cowardice, pain, submission and sadness . The latter demonstrates the feeling of the professional when witnessing a violent situation. On the other hand, the literature reports that victims of domestic violence who have gone through derogatory experiences also experience sadness22. Possibly, pain refers to a consequence of both, the physical and the psychological aggression. The submission was mentioned six times and reveals the passivity attributed to women, still strongly rooted in society.
It is really about discrimination, because they do not know what the woman suffers, they think men deserves more because they provide to food. (CHW)
It is a violence when he attacks the person verbally; sometimes it hurts more than when he assaults her physically. (NT)
I did not know what to do, I did not know if I should leave or stay, it was horrible, so sad. (CHW)
Sadness, for they do not have balance of talking, keep calm, I found it very sad. (NT)
Understanding that the peripheral elements are more accessible, alive and concrete, "they are the interface between the core and the concrete situation in which the representation is developed and put into operation" 19:32. In the upper right quadrant, the first periphery, youngest professionals raised terms such as fear and revolt, pointing to an indignation of the victim that may trigger a position and the search for change. Oldest professionals evoked in the first periphery the term low self-esteem as a constant feeling the victim. This differentiation in the organization of the content of the representation can be seen by the situation in which the studied groups are inserted20as more age supposedly indicates greater professional experience, and this can modify the representation of DVAW.
Today this cannot happen, when I face such a situation I feel revolt. (CHW)
I think that violence against women, from the side of the woman, is lack of self-esteem. (TE) Her face deformed ... black eye, cut mouth that, she had no way to hide [...] what I said, self-esteem ... (CHW)
In the second periphery, the lower right quadrant, are the infrequent elements and characterized as less important by the research subjects. In the representation of youngest professionals, this contains the terms low self-esteem, submission, sadness and humiliation.
The oldest group evoked abuse of power, alcoholism, drug addiction, lack of dialogue, family, children and acceptance, highlighting the reality they experience in their daily work and in the family environment. By evoking the terms alcoholism, drug addiction and lack of dialogue, health professionals showed some of the factors triggering the DVAW and thus they expressed them in denatured form. Alcohol abuse is a common reality among offenders2.
Another reality witnessed in the daily work of oldest professionals is the concern of the victims with the welfare of children, which can justify their decision for not to report the aggression.
Violence against women for me is much humiliation; the woman goes through a lot of humiliation, much submission, as sometimes the woman depends largely on the husband. (CHW)
It was not the drink, maybe something with drugs because he use to go mad, out of control. (NT)
She has her children to take care of, she has the children who depend on her and they depend on the house. (CHW)
At the end, the patient ends up giving in, and accepting the situation. (NT)
The term acceptance refers to the position of the victim toward the occurrence of violence. Sometimes this situation stems from the lack of women's awareness of their rights or the sense of shame in exposing their situation24. A study carried out with married women showed that they resign to the violence and defend the aggressor when they see him being arrested by police25. Behaviors such as these can influence the construction of social representation of DVAW among professionals, making prejudgments interfere with humanized actions toward battered women.
CONCLUSION
The DVAW is presented as a topical social phenomenon and still secluded in homes, often due to historical and socio-cultural issues that underlie human behavior. This study revealed that there is a differentiation in the representation of DVAW, according to the age of informants.
The feeling of fear is more intense among professionals aged over 41 years as this feeling integrates the core of theirs social representation, while the representation of youngest professionals puts fear in the first periphery. Fear is represented as a feeling common to victims and professionals that influences the complaint and the action, respectively.
It is also notable the possibility of a subgroup with a different representation among the youngest group, which is identified by the term impunity in the contrast zone. This term does not appear in the representation of professionals with more age. Taking into account that the protective legislation is recent in Brazil, it is understood that because they have experienced for so many years the non-criminalization of violence, these professionals keep a sense of helplessness. On the other hand, they evoked triggers of violence, what could mean that the social representation of DVAW among these professionals has been denatured. These factors were evoked by the terms drug addiction, alcoholism and lack of dialogue, present in the second periphery, which approaches the representation of social practices. It is noteworthy that the study has as limitation its realization in a single socio-cultural context. Further studies with this approach are, therefore, recommended with other professionals working in different contexts.
REFERENCES
1.Brazil. Law nº 11.340, of August 7, 2006. Creates mechanisms to restrain domestic and family violence against women. Brasília. 2006
2.Fageeh WMK. Factors associated with domestic violence: a cross-sectional survey among women in Jeddah, Saudi Arabia. BMJ Open. 2014 [cited 2014 Aug 15] 4 (2). Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3927923/
3.Brazil. Civil Code comparative table 1916/2002. Brasília. 2003 [cited 2014 Aug 15]. Available from: http://www.livrosgratis.com.br/arquivos_livros/sf00021a.pdf
4.Solano LC, Queiroz JC, Carvalho FPB, Timóteo RPS, Monteiro AI. The historical process of the contemporary family archetype and the invention of incest. Rev. enferm. UERJ; 2009; 17: 601-5. Available in: http://www.facenf.uerj.br/v17n4/v17n4a25.pdf
5.Cabette ELS, Silva LR. Law Maria da Penha, violence, fear and love: from complaint to forgiveness. Jus Navigandi. 2013 [cited 2014 Aug 15] 18:3788. Available from: http://jus.com.br/artigos/25829
6.Cfemea. Maria da Penha Law: from paper to life. Comments on the Law 11.340/2006 and its inclusion in the budget cycle. 2nd ed., Brasilia, 2009
7.Souza PRA. The Maria da Penha Law and its contribution to the eradication of gender discrimination in Brazilian society. In: Legal Scope, Rio Grande, XII, n. 61, 2009. [cited 2014 Aug 12]. Available from: http://www.ambito-juridico.com.br/site/index.php?n_link=revista_artigos_leitura&artigo_id=5886
8.Waiselfisz JJ. Map of Violence 2012: Assassination of Women in Brazil. 2012
9.Datasenado (Br). Shy away domestic and family violence against women. 2013. [cited 2014 Aug 19]. Available from: http://www.senado.gov.br/noticias/datasenado/pdf/datasenado/DataSenado-Pesquisa-Violencia_Domestica_contra_a_Mulher_2013.pdf
10.Gomes NP, Erdmann AL. Conjugal violence in the professional perspective of "Family Health Strategy": a public health problem and the need for care to women. Rev Latino-Am Nursing. 2014; 22: 76-84
11.Guedes RN, Silva ATMC, Fonseca RMGS. Gender violence and the health-disease of women. Anna Nery Rev. Enferm. 2009; 13: 625-31
Ministry of Health (BR). The work of the community health agent. Ministry of Health. Brasília. 2009
13.Jodelet D. Social representations: an area expansion. In: Jodelet D, organizer. Social representations. Translation Lilian Ulup. Rio de Janeiro: Ed UERJ;. 2001. 34-45.
14.Abric JC. Structural approach of social representations: recent developments. In: Campos PHF, Loureiro MCS, organizers. Social Representations and Educational Practices. Goiânia: UCG, 2003. 21-8.
15.Sá CP. Introduction. In: Sá CP. Central core of social representations. 2ª ed. Petrópolis : Vozes, 1995. 19-56.
16. Oliveira DC, Marques SC, Gomes AMT, Teixeira MCTV. Analysis of free evocations: a technique of structural analysis of social representations. In: Moreira ASP, organizer. Theoretical and methodological perspectives on social representations. JoãoPessoa: UFPE University Publishing; 2005. 572-8.
17.Gomes AMT, Silva EMP, Oliveira DC. Social representations of AIDS for people living with HIV and their everyday interfaces. Rev Latino-Am Nursing. 2011. 19: 485-92
18. Bardin L. Coding. In: Bardin L. Content analysis. Sao Paulo: Edition 70, 2011. 28-61.
19.Abric JC. The structural approach of social representations. In: Moreira ASP, Oliveira DC, organizers. Interdisciplinary studies of social representation. Goiânia: AB, 1998. 25-43.
20.Sá CP. The construction of the research object in social representations. In: Sá CP. The identification of the phenomena of social representation. Rio de Janeiro: UERJ, 1998. 12-36.
21.Moscovici S. Social representation: a lost concept.
In: Moscovici S. The social psychoanalysis: a lost concept. Translation
Sonia Fhurmann. Petrópolis: Vozes, 2012. 39-75
22.Vieira EM, Ford NJ, Ferrante FG, Almeida AM, Daltoso D, Santos MA. The response to gender violence among Brazilian health care professionals. Scien public health. 2013; 18: 681-90
23.Silva CD, Gomes VLO, Acosta DF, Barlem ELD, Fonseca AD. Epidemiology of violence against women: characteristics of the aggressor and the violent act. Rev enferm UFPE on line., Recife, 7 (1): 8-14., Jan., 2013.
24.Abeya SG, Afework MF, Yalew AW. Intimate partner violence against women in West Ethiopia: a qualitative study on attitudes, woman's response, and suggested measures as perceived by community members. Reprod Health. 2012 [cited 2014 Aug 22]. 20:14. Available from: http://www.ncbi.nlm.nih.gov/pubmed/22906066
25. Semahegn A, Belachew T, Abdulahi M. Domestic violence and its predictors among married women in reproductive age in Fagitalekoma Woreda, Awi zone, Amhara regional state, North Western Ethiopia. Reprod Health. 2013 [cited 2014 Aug 10]. 5:63. Available from: http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3879008/