* Participating professionals may have marked more than one item in question.
Source: survey data
ORIGINAL RESEARCH
Care by family health strategy personnel during the climacteric
Angela Bete Severino PereiraI; Cleusa Alves MartinsII; Milca Severino PereiraIII; Jacqueline Rodrigues de LimaI; Adenícia Custódia Silva e SouzaV; Priscilla Santos Ferreira ReamVI
I
Nurse. Master in Health Education. Nurse at the Hospital das Clínicas of
the Federal University of Pernambuco. The Municipal Secretariat of Health
of Goiânia. Goiânia, Goiás, Brazil, Email: angelabete@gmail.com
II
Nurse. PhD in Nursing, Nursing School of the Federal University of Goiás.
Professor in the Graduate Program in Education in the health of the Nursing
School of the Federal University of Goiás. Goiânia, Goiás, Brazil, Email: cleusa.alves@gmail.com
III
Nurse. PhD in Nursing, Department of Nursing, Nutrition and Physical
Therapy. Professor in the Master in Healthcare at the Pontifical Catholic
University of Goiás. Goiânia, Goiás, Brazil, Email: milcaseverino@gmail.com
IV
Nurse. PhD in Nursing, Nursing School of the Federal University of Goiás.
Professor in the Graduate Program in Education in the health of the Nursing
School of the Federal University of Goiás. Goiânia, Goiás, Brazil, Email: jlima_fen@yahoo.com.br
V
Nurse. PhD in Nursing, Department of Nursing, Nutrition and Physical
Therapy. Professor in the Master in Healthcare at the Pontifical Catholic
University of Goiás. Goiânia, Goiás, Brazil, Email: adeniciafen@gmail.com
VI
Nurse. Master's in Nursing, Goiânia, Goiás, Brazil, Email: prisf_enf@yahoo.com.br
DOI: http://dx.doi.org/10.12957/reuerj.2016.13122
ABSTRACT
Introduction: the climacteric is a period of physical, psychological, and emotional changes that impact women's quality of life, and requires preparation for comprehensive care. Objective: to analyze the profile of Family Health Strategy (FHS) personnel, their skills, difficulties, and actions performed in care provided to climacteric women. Method: this is a descriptive, cross-sectional study. The participants were 57 university graduate healthcare professionals working in the FHS in the Goiania health district, Goias State, Brazil, in 2013. Results: the climacteric and menopausal periods were correctly defined by 80.8% of nurses, with a lower success rate among other personnel. Deficiencies in professional training were cited by 43.9% of participants. The majority (70.2%) reported giving guidance in the consulting room, and cited a lack of multidisciplinary educational activities. Conclusion: continuing professional development strategies need to be reinforced, as do direct interventions to assure comprehensive care.
Keywords: Climacteric; family health; women´s health; continuing education.
INTRODUCTION
Climacterium is an event which occurs between 35 to 65 years of age, or before, if removal of the ovaries, associated or not to hysterectomy. It represents a biological step in the woman's life characterized by the transition between the reproductive phase and the non-reproductive1,2. When this phase is associated to the occurrence of symptoms is defined as the syndrome of menopause, and which can lead to emotional, social and physical changes in female life3.
It is perceived national and international tendency to consider the climacterium as an endocrinopathy, with emphasis on medicalization in health, in medical interventions2,4,5, in spite of movements opposed to the medicalization of biological phenomena6.
In this phase, the woman perceives that their vitality is in decline, due to the physical changes resulting from the reduction of the collagen of the skin, the presence of pathologies, headaches and other signs peculiar to aging, causing conflicts and questionings that can affect their physical and mental health1.
Many women live the climacterium without complaints or need for drugs, other present symptoms ranging in diversity and intensity. However, in both cases, it is essential that there should be a systematic monitoring aiming qualified listening, health promotion, early diagnosis, immediate treatment of health problems and prevention of damage6-8.
The increase of life expectancy9 and the accelerated population aging have caused a significant increase in the number of women experiencing the menopause, making it necessary a greater preparation of healthcare services to meet the demands with quality and effectiveness10.
The Family Health Strategy (FHS) becomes an important space to provide adequate assistance to women in perimenopause to act primarily on the relationship between health promotion and disease prevention1,11 .
As the ESF the main gateway to the public health system, it is necessary to analyze the comprehensive care provided to users. It is conjectured: is the care to women carried inside of official recommendations? Does it follow a protocol compatible with the needs of women in the climacterium period? Do the health team professionals receive qualification focused on the climacterium?
This study proposes to analyze the profile of professionals, knowledge, difficulties and activities in the care of climacteric women in the FHS.
LITERATURE REVIEW
The Family Health Program was established in 1994, and later called FHS, with the objective to offer humanized care, integral, facing the family and community12.
In Brazil, the FHS allowed to expand primary care and brought important achievements for the realization of the principles of the universal right to health. However, underfunding the precarious infrastructure, the high turnover of workers, among others, represent challenges for the consolidation of the Unified Health System (SUS) and the quality care of growing demand with its appropriate specificities in FHS13.
In 2012, 36.7% of Brazilian women were in the age range in which the climacterium occurs. In the same year, in Goiás, the proportion of the female population of 35 to 65 years was similar to the national rate, corresponding to 36.4% and, in Goiania, 38.2%14.
Usually women experience this lonely stage, silently and with insufficient information15. For this reason, it is considered that quality of life is the foundation d the implementation of interventions in the climacterium being valued, also, the subjective aspects and cultural complaints6,16.
The deployment of women healthcare in climacterium presupposes the existence of health professionals duly trained and sensitized to the particularities inherent to this population group. Education in health performed with quality strengthens the autonomy of users in the control of the health-disease process, leading them to the transformation of their habits, to respect the local culture and thus enhancing this process, with a view to improving their quality of life17-19.
Permanent education is used as a space for thinking and run the training and professional development staff and of health teams, with a view to work the elements which confer the integrality of healthcare. It is one of the viable alternatives for changes in the work space, due to enable differentiated forms of educating and learning, by means of which proposes an active participation of professionals in the process20. In this perspective, the permanent education contributes significantly to the development of the skills of FHS team of professionals and for the effective resolubility and integrality21.
METHODOLOGY
Cross-sectional study, exploratory study, performed with top-level professionals from the health team of the FHS of Family Health Centers (FHC) located in the East Health District (EHD), in the city of Goiânia, Goiás, Brazil.
Goiânia has seven Health districts, being that the EHD is responsible for nine FHC where they employ 29 teams; three integral healthcare centers; two healthcare centers; a type II Psychosocial Care center and a male therapeutic residence. Its coverage area has a population of approximately 180 thousand inhabitants.
The study included all health professionals, higher education, who worked in the FHS in a period less than six months and excluded those who were absent at the time of data collection.
We chose to higher education, professionals - nurses, doctors and dental surgeons - by being responsible for coordinating the actions undertaken in the Community.
The contact with the participants was performed in the morning and afternoon from Monday to Saturday. The approach was performed individually, occasion on which we have explained the objectives, methodology and the ethical aspects. The professionals who agreed to participate signed the Free and Informed Consent Term, previously filling out the research instrument.
The data were collected in the period of October and November 2013 by means of a questionnaire, which was evaluated by five experts in the area of research, as to their form and content, and subjected to a pilot test to check its operability and functionality.
The following categories for the study have been previously defined: sociodemographic characteristics; actions developed for the attention to the health of women in the climacterium; knowledge of the professionals about the climacterium and menopause; difficulties of professionals in care to women; climatic and permanent educational activities in health developed in the FHS.
In order to evaluate the responses of healthcare professionals participating, considered to be correct, the following definitions relating to climacterium and menopause: Climacterium - phase of a woman's life in which occurs the transition of the reproductive period for the reproductive not due to reduced ovarian hormones. Menopause - last menstrual flow of women1.
The data were processed in Statistical Package for the Social Sciences, version 17.0, using descriptive statistics, with the use of absolute frequency, relative, mean and standard deviation.
The study, authorized for implementation within the framework of the Municipal Health Department of Goiânia, was approved by the Ethics Committee in Research of the Clinical Hospital of the Federal University of Goiás, under the opinion number 456.352/2013.
RESULTS AND DISCUSSION
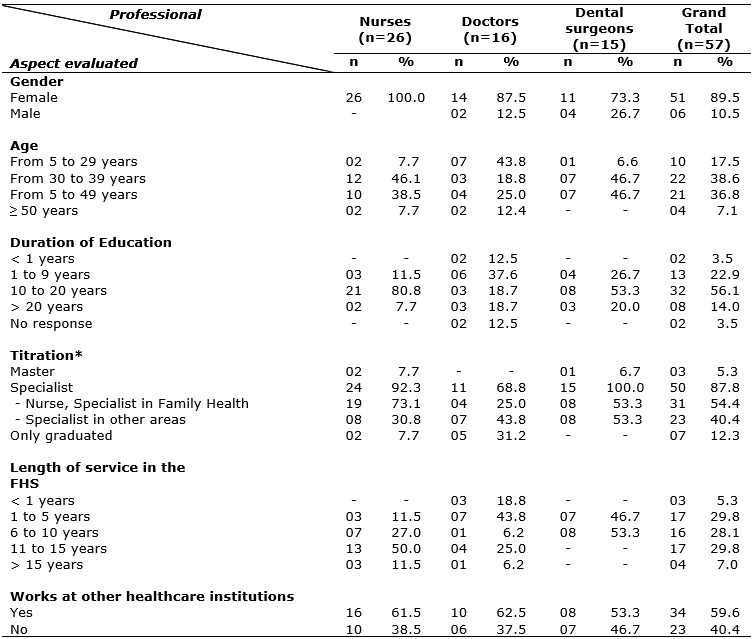
The participants were 57 (75%) of the 76 healthcare professionals set to work in the EHD at the FHS, characterized in Table 1. Among those who had not participated, 16 (21%) professionals were not present in the FHC or refused to take part in the study and had a deficit of three (4%) physicians in the data collection period.
Table 1:
Characterization of health professionals of the highest level of the family
health Strategy of the eastern region of Goiânia (n = 57). Goiânia, Go,
2014
* Participating professionals may have marked more than one item in
question.
Source: survey data
Professional females predominated (89.5%), which is compatible with search results also carried out with workers of the FHS in the Goiania EHD22. The feminization of nursing, medicine and dentistry was recorded in other studies with professionals and undergraduate students23-26. The mean age of the participants was 38.6 years, ranging from 24 to 70 years, with a standard deviation of 9.4 years, similar to the average found in studies carried out with workers of the FHS in 22 municipalities of Rio Grande do Sul and dental surgeons of the FHS 15 municipalities of Pernambuco26,27.
Regarding the graduation time, the predominant period was between 10 to 20 years for nurses (80.8%) and dental surgeons (53.3%), and from 1 to 9 years for doctors (37.5%). These data corroborate findings of a study with doctors and nurses of the FHT in Rio Grande do Norte24, but differ in the study with dental surgeons of Pernambuco, in which 34.8% of the participants had between 1 to 5 years since graduation26.
Most professionals participants (59.6%) mentioned have more of an employment relationship, characteristic also mentioned in other studies with professionals working in the FHS27,28.
Working time in the FHS among professionals ranged from 6 months to 20 years, with an average of 8 years of service. When analyzed individually, by category, this data varies between nurses and the other professions: while the nurses presented an average of 11 years of experience in the FHS, the doctors and dental surgeons an average of 6 years. In this study, 62.6% of the physicians had fewer than six years of practice in the FHS, compatible with other studies24,28. These data, added to the fact that the availability of three vacancies for doctors in the period of investigation, suggest the turnover among these professionals in the FHS in Goiânia. Studies that present the demographic profile of doctors and dental surgeons describe the existence of opportunities in the private sector, search for training and/or the precarious employment laws as justifications for this turnover26-28. In the case of dental surgeons, the insertion of these professionals in the FHS teams, in Goiania, started in 2004, being that in some FHC of EHD the oral health teams were deployed after 2010.
The bond, continuity of care, the integrality and accountability are part of the principles of primary care in the country11. The high rotation of professionals represents an important barrier to the fulfilment of such principles13, 29.
The professionals reported having had at least one specialization (87.8%), being 92.3% nurses, 100.0% dental surgeons and 68.8% doctors. In another study22 carried out with these same professional categories and in the same FHC of the EHD of Goiânia, the experts were respectively 77.2%, 62.5% and 50%. Despite the little difference in the number of the sample (n=57 and n=54) of these two studies, the variation of results can be justified in part by the turn over of staff and the respondents.
In the set of health professionals from the top level of the FHS, some studies also point out that the majority of workers had completed a specialization24,27,28,30. The findings of this research as to the rate of specialization of the medical team are higher than those found in the literature28,30.
As to the permanent education about the health of the woman to multidisciplinary teams of the FHS, 31 (54.4%) mentioned does not exist, contradicting study performed with nurses of the FHT A Sanitary District of Goiânia that points to the existence of offering these activities21. Nurses are professionals who more participate of permanent educational activities proposed for the team of the FHS in the context of the EHD.
Of the 35 (61.4%) professionals that they took courses in the area of women's health, only 10 (17.5%) mentioned that the content was addressed the assistance to women in the climacteric phase.
The permanent education still represents a challenge within the FHS through lack of investment13, by the fragmentation of content and/or ad hoc nature of opportunities for training and improvement31.
Deficiencies in the training of professionals on climacterium and menopause reflected in the lack of knowledge on the subject, according to Table 2. The insufficiency of content directed to this stage, in training and health training, is cited in other studies32-34.
Table 2:
Knowledge of higher level health professionals Strategy Health Region
Family Eastern Goiânia (n = 57) on menopause and climacterium. Goiânia, Go,
2014

Source: survey data
Although 96.5% of the participants have responded to be no difference between the climacteric and menopause, only 57.9% knew how to define these two phases, namely: 21 (80.8%) nurses, six (37.5%) doctors and 6 (40%) dental surgeons, according to Table 2. The knowledge of nurses was also highlighted in another study24.
It is perceived that the different professional categories receive training / training differently on issues about care for women. Ordinance no. 278/2014 of the Ministry of Health states that skills must be performed for all team members to facilitate the joint planning of actions in favor of the health of users, as well as, potentiate their results by reducing the fragmentation of care35. The National Policy of Basic recommends that the monitoring of the users in the FHS units is in a holistic way, with planning and answering a multi-professional team11, which was not always referred to by the participants.
In this aspect, we emphasize the responsibility of all primary care management spheres in promoting initiatives involving "[...] the development worker with qualification of services offered to users [...] " 11:27 by of lifelong education, guarantee labor rights, training of work contracts, implementation of careers, among others."
As for the actions undertaken by the FHS team in relation to women's health, all the participants cited the prenatal care, the prevention of breast cancer and cervical cancer. Other activities identified were related to sexually transmitted diseases (54/94.7%), record in Oncology Information Systems (48/84.2%), care for victims of sexual violence (47/82.5%) and domestic (46/80.7%), and prescription of hormone replacement therapy (40/70.2%). Thus, the attention to women's health, generally, is limited to the reproductive period, the prevention of cervical cancer and breast cancer and monitoring of non-transmissible chronic diseases33,36,37.
The activities developed specifically with women in the climacteric and menopause are described in Table 3.
Table 3:
Actions developed in the attention to women in the climacterium referred to
top-level health professionals of the family health strategy of the eastern
region of Goiânia (n = 57). Goiânia, Go, 2014
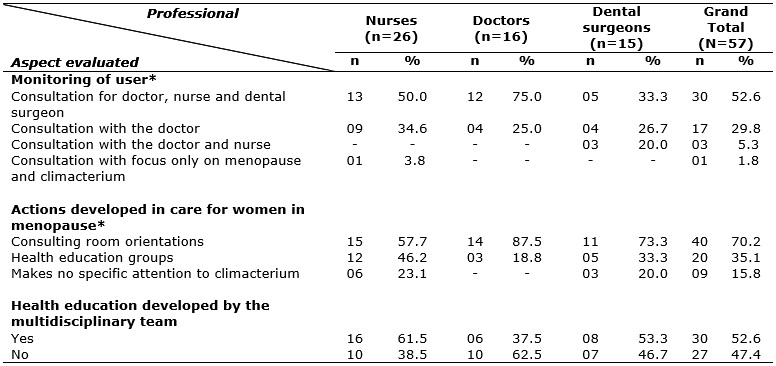
* Participating professionals may have scored more than one item in
question
Source: survey data
The monitoring of women in menopause and climacteric is predominantly performed by means of individual consultations with each team member (52.6%). The recommendations of the HM emphasize the team work in which the assistance to users should be planned and executed jointly in accordance with the competence of each professional11, thus avoiding the fragmented assistance by disciplines.
Yet, 17 (29.8%) participants mentioned that the consultation was only with the doctor and 3 (20%) dental surgeons mentioned that monitoring is carried out only by medical consultations and nursing. These findings suggest the persistence of the medical model-centered and/or the fragility in (auto) perception of professionals in the context of interdisciplinarity38.
The account of dentists, which reported attendance only by the doctor and nurse, get a call that require greater integration to the multidisciplinary team. This trait also was mentioned in study in Minas Gerais39, recording the oral health team has strength as to work together with other FHS members. It is also highlighted that the teaching-learning practices in educational institutions are usually performed in a fragmented manner and multi-professional nature activities are insufficient to develop integration ability of future professionals. Indeed, in this study, 23.1% of nurses and 20% of dentists mentioned do not perform specific attention to climacterium.
The participants (70.2%) say that the actions in health care of women are mostly carried out by the guidelines in the office; 35.1% of the respondents cited health education groups, of which 29.8%, amounted activity in waiting rooms; and 14.1% in other social spaces. Individual interventions carried out in practice cannot always be considered as an activity of health education, because they do not allow the active participation of the user in the construction of knowledge22. Health education is considered an essential tool in primary care, and when properly applied enables the optimization of care to cause the user to actively participate in their treatment resulting in better resolution of health problems12,18.
It is pointed out that 27 (47.4%) participants have denied conducting any activity of health education with climacteric women by the multidisciplinary team of the FHS unit, which is contrary to the recommendations of the national primary health care Policy that provides for the realization of "[...] actions in health education to the assigned population [...] " 11:45 for all the FHS professionals. A study of FHS doctors in Minas Gerais, Brasil, states that although 69.3% of these professionals meet climacteric women, only 27.6% carry out educational activities targeted to the topic and 61.9% report difficulties to work at this stage34.
The contrast to the aspect assessed on health education activities in the office or in groups can mean that the actions represent isolated efforts of certain professional categories, also mentioned in another study24.
The lack of qualifications was the greatest difficulty that in meeting the climacteric women (43.9%), followed by infrastructure deficiencies and lack of materials (14.0%) - remembering that these two aspects are the responsibility of municipal, state and federal spheres11.
Another difficulty reported by four nurses in the care of climacteric women was related to problems in the organization of reference and counter system, and miscommunication between the professional team also identified another multicenter study on the FHS40. The primary care should be guided by the integration of services as well as by access to specialized services should be structured in such a way as to implement the call that it is possible to more resolutive36.
It is noteworthy that, despite the existence of public policies directed to the reorientation of the attention model and women's health1.11, programmatic unidisciplinary practices are predominant in the FHS. Thus, the lack of knowledge and practices directed to the integrality of attention to women's health in the climacteric, in this study, can be justified by the need of workers to meet the demands arising from management and monitoring and evaluation instruments. The invisibility of the climacterium in health care of women, identified in this study may be the same reality of other health units or in other regions, because few studies in this area and the FHS have similar results6, 33, 34, 37.
CONCLUSION
This study revealed that the professionals have limited knowledge about the climacterium. The healthcare of women in the FHS occurs mainly during the reproductive period and the prevention of cervical cancer and breast cancer. Care in the climacterium is performed by the entire staff (nurses, doctors and dentists), but with an emphasis on individualized guidance and in doctor offices. An understanding was evidenced for the healthcare offered at the individual level, on a doctor-centered perspective, and dentists do not perceive team members, when it comes to care for climacteric women. Interdisciplinary health education activities carried out in groups and targeted to women's health or the climacteric are prioritized by the multidisciplinary team.
Most participants reported absence of continuing education opportunities in the health of women for the FHS teams. The professionals who claimed trainings in this area pointed to the absence or reduced content targeted towards climacteric women. In this perspective, the invisibility of this theme in the training and qualification of FHS health professionals, as well as inadequate conditions of work, were the main difficulties identified, under the care of climacteric woman.
As limitation of the study highlights the fact that address the topic only in a health district, but the data revealed a scenario similar to that found in other polls. Furthermore, despite not allowing generalizations, parameters can be established for interventions in the area of care for climacteric women.
The results suggest the need to expand the insertion of content about menopause, training and continuing education of healthcare professionals. Principles and guidelines that characterize the FHS, such as the integrality of care, humanization, access and resolutivity, they should be valued and guide the work process and evaluation teams in the framework of care for women.
It is considered as the greatest legacy of this research the observed indicators that can support decision making by managers and leaders to establish and strengthen public policies.
REFERENCES
1. Ministério da Saúde (Br). Manual de Atenção à Mulher no Climatério/Menopausa. Brasília (DF): Ministério da Saúde; 2008a.
2. Valença CN, Nascimento-Filho JM, Germano RM. Mulher no climatério: reflexões sobre desejo sexual, beleza e feminilidade. Saude soc [Scielo-Scientific Electronic Library Online] 2010 [cited on 2014 Sep 14]. 19(2):273-85. Available from: http://dx.doi.org/10.1590/S01042902010000200005
3. Sáez YG, Sáez IH, Batueca SIH, Delgado JCP, Peña NF, Aldana EB. Intervención educativa para elevar conocimientos sobre climaterio y menopausia. AMC [Scielo-Scientific Electronic Library Online] 2012 [cited on 2014 Sep 14]. 16(1): 5-14. Available from: http://scielo.sld.cu/pdf/amc/v16n1/amc020112.pdf
4. Enciso JMM, Aujang ER, Ulloa RA. Trastornos metabólicos de mujeres en el climaterio. Ginecol Obstet Mex [Internet] 2013 [cited on 2014 Sep 14]. 81(4):186-89. Available from: http://www.medigraphic.com/pdfs/ginobsmex/gom-2013/gom134d.pdf
5. Stouthamer N, Visser AP, Oddens BJ, Beusmans G, Hoogland, H, Van Ree JW, et al. Dutch general practitioners' attitudes towards the climacterium and its treatment. Eur J Obstet Gynecol Reprod Biol [Medical Literature Analysis and Retrieval System Online] 1993 [cited on 2014 Sep 14]. 50(2):147-52. Available from: http://download.journals.elsevierhealth.com/pdfs/journals/0028-2243/PII002822439390179G.pdf
6. De Lorenzi DRS, Catan LB, Moreira K, Ártico GR. Assistência à mulher climatérica: novos paradigmas. Rev Bras Enferm [Scielo-Scientific Electronic Library Online] 2009 [cited on 2014 Sep 14]. 62(2):287-93. Available from: http://dx.doi.org/10.1590/S0034-71672009000200019
7. Ministério da Saúde (Br). Departamento de Monitoramento e Avaliação da Gestão do SUS. Secretaria de Gestão Estratégica e Participativa. Painel de indicadores do SUS n°4. Temático Saúde da Família. Brasília (DF): Organização Pan-Americana da Saúde; 2008b.
8. Ang SB, How CH. Menopause: an important milestone in women's health. Singapore Med J [Medical Literature Analysis and Retrieval System Online] 2013 [cited on 2014 Sep 14]. 54(2):60-3. Available from: http://www.sma.org.sg/UploadedImg/files/SMJ/5402/5402practice1.pdf
9. Instituto Brasileiro de Geografia e Estatística [site de Internet]. Censo Demográfico 2010. Características da população e dos domicílios: Resultados do universo. [cited on 2014 Sep 14] Available from: http://www.ibge.gov.br/home/estatistica/populacao/censo2010/caracteristicas_da_populacao/resultados_do_universo.pdf
10. Küchemann BA. Envelhecimento populacional, cuidado e cidadania: velhos dilemas e novos desafios. Soc estado [Scielo-Scientific Electronic Library Online] 2012 [cited on 2014 Sep 14]. 27(1):165-80. Available from: http://dx.doi.org/10.1590/S0102-69922012000100010
11. Ministério da Saúde (Br). Secretaria de Atenção à Saúde. Departamento de Atenção Básica. Política Nacional de Atenção Básica. Brasília (DF): Ministério da Saúde; 2012.
12. Oliveira SRG, Wendhausen ALP. (Re)significando a educação em saúde: Dificuldades e possibilidades da Estratégia Saúde da Família. Trab Educ Saúde [Scielo-Scientific Electronic Library Online] 2014 [cited on 2014 Sep 14]. 12(1):129-47. Available from: http://dx.doi.org/10.1590/S1981-77462014000100008
13. Sousa MF, Hamann EM. Programa Saúde da Família no Brasil: uma agenda incompleta?. Cien Saúde Colet [Scielo-Scientific Electronic Library Online] 2009 [cited on 2014 Sep 14]. 14(Supl.1):1325-35. Available from: http://dx.doi.org/10.1590/S1413-81232009000800002
14. Datasus. Departamento de Informática do SUS [site de Internet]. Indicadores demográficos 2012. [cited on 2014 Sep 14] Available from: http://tabnet.datasus.gov.br/cgi/tabcgi.exe?idb2012/a01.def
15. Costa GMC, Gualda DMR. Conhecimento e significado cultural da menopausa para um grupo de mulheres. Rev Esc Enferm USP. 2008; 42(1):81-9.
16. Silva-Filho EA, Costa A M. Avaliação da qualidade de vida de mulheres no climatério atendidas em hospital-escola na cidade do Recife, Brasil. Rev Bras Ginecol Obstet [Scielo-Scientific Electronic Library Online] 2008 [cited on 2014 Sep 14]. 30(3):113-20. Available from: http://dx.doi.org/10.1590/S0100-72032008005000001
17. Monte TL, Mattos FTC, Moura GCB, Moura LKB, Nunes CMCLL, Ferraz MAAL . Produção científica sobre os modelos de educação em saúde na promoção de saúde bucal. Rev Interdiscip [Internet] 2013 [cited on 2014 Sep 14]. 6(4):235-42. Available from: http://revistainterdisciplinar.uninovafapi.edu.br/index.php/revinter/article/view/229/pdf_87
18. Hermosa AB, Mejía RC. Menopausia y estereotipos de género: importancia del abordaje desde la educación para la salud. Rev Enferm UERJ [Internet] 2014 [cited on 2014 Sep 14]. 22(2):182-6. Available from: http://www.facenf.uerj.br/v22n2/v22n2a06.pdf
19. Vidal CRPM, Miranda KCL, Pinheiro PNC, Rodrigues, DP. Mulher climatérica: uma proposta de cuidado clínico de enfermagem baseada em ideias freireanas. Rev Bras Enferm [Scielo-Scientific Electronic Library Online] 2012 [cited on 2014 Sep 14]. 65(4):680-4. Available from: http://dx.doi.org/10.1590/S0034-71672012000400019
20. Salum NC, Prado, ML. A educação permanente no desenvolvimento de competência dos profissionais de enfermagem. Texto Contexto Enferm [Scielo-Scientific Electronic Library Online] 2014 [cited on 2014 Sep 14]. 23(2):301-8. Available from: http://www.scielo.br/pdf/tce/v23n2/pt_0104-0707-tce-23-02-00301.pdf
21. Paulino VCP, Bezerra, ALQ, Branquinho NCSS, Paranaguá TTB. Ações de educação permanente no contexto da Estratégia Saúde da Família. Rev enferm UERJ [Internet] 2012 [cited on 2014 Sep 14]. 20(3):312-6. Available from: http://www.e-publicacoes.uerj.br/index.php/enfermagemuerj/article/view/687/2885
22. Silva EAS. Primeira infância: práticas educativas na estratégia saúde da família [master degree]. Goiânia: Universidade Federal de Goiás; 2012.
23. Costa SM, Durães SJA, Abreu MH, N. G. Feminização do curso de odontologia da Universidade Estadual de Montes Claros. Cien Saude Colet [Scielo-Scientific Electronic Library Online] 2010 [cited on 2014 Sep 14]. 15(Supl. 1):1865-73. Available from: http://dx.doi.org/10.1590/S1413-81232010000700100
24. Jácome EM, Silva RM, Gonçalves MLC, Collares PMC, Barbosa IL. Detecção do Câncer de Mama: conhecimento, atitude e prática dos médicos e enfermeiros da Estratégia Saúde da Família de Mossoró, RN, Brasil. Rev Bras Cancerologia [Internet] 2011 [cited on 2014 Sep 14]. 57(2):189-98. Available from: http://www.inca.gov.br/rbc/n_57/v02/pdf/06_artigo_deteccao_cancer_mama_conhecimento_atitude_pratica_medicos_enfermeiros_estrategia_saude_familia_mossoro_RN_brasil.pdf
25. Lopes MJM; Leal, SMC. A feminização persistente na qualificação profissional da enfermagem brasileira. Cad Pagu [Scielo-Scientific Electronic Library Online] 2005 [cited on 2014 Sep 14]. 24:105-25. Available from: http://dx.doi.org/10.1590/S0104-83332005000100006
26. Martelli PJL, Macedo CLSV, Medeiros KR, Silva SF, Cabral APS, Pimentel FC, et al. Perfil do cirurgião-dentista inserido na Estratégia de Saúde da Família em municípios do estado de Pernambuco, Brasil. Cien Saude Colet [Scielo-Scientific Electronic Library Online] 2010 [cited on 2014 Sep 14]. 15(suppl.2):3243-8. Available from: http://dx.doi.org/10.1590/S1413-81232010000800029
27. Zanetti TG, Sand ICPV, Girardon-Perlini NMO, Kopf AW, Abreu PB. Perfil socioprofissional e formação de profissionais de equipes de saúde da família: um estudo de caso. Cienc Cuid Saude [Internet] 2010 [cited on 2014 Sep 14]. 9(3):448-55. Available from: http://periodicos.uem.br/ojs/index.php/CiencCuidSaude/article/viewFile/7664/6655
28. Guarda FRB, Silva RN, Tavares RAW. Perfil sociodemográfico dos médicos que compõem equipes de saúde da família na Região Metropolitana do Recife, Estado de Pernambuco, Brasil. Rev Pan-Amaz Saude [Scielo-Scientific Electronic Library Online] 2012 [cited on 2014 Sep 14]. 3(2):17-24. Available from: http://scielo.iec.pa.gov.br/pdf/rpas/v3n2/v3n2a03.pdf
29. Mishima SM, Pereira MJB, Fortuna CN, Matumoto S. Trabalhadores de saúde: problema ou possibilidade de reformulação do trabalho em saúde? – Alguns aspectos do trabalho em saúde e da relação gestor/ trabalhador. In: Ministério da Saúde (Br). Observatório de Recursos Humanos em Saúde no Brasil: estudos e análises. Rio de Janeiro (RJ): Fiocruz; 2003, p. 137-156.
30. Jácome EM. Detecção do Câncer de Mama: conhecimento, atitude e prática dos médicos e enfermeiros da Estratégia Saúde da Família de Mossoró (RN) [master degree]. Fortaleza: Universidade de Fortaleza; 2009.
31. Feitosa LS, Lima MS, Machado MFAS, Costa CCC, Pessoa VM. Caracterização da educação permanente na Estratégia Saúde da Família: o caso na Escola de Saúde Pública do Ceará. Cadernos ESP [Internet] 2010 [cited on 2014 Sep 14]. 4(2):25-31. Available from: http://www.esp.ce.gov.br/cadernosesp/index.php/cadernosesp/article/view/37/33
32. Beltramini ACS, Diez CAP, Camargo IO, Preto VA. Atuação do enfermeiro diante da importância da assistência à saúde da mulher no climatério. REME [Base de dados de Enfermagem] 2010 [cited on 2014 Sep 14]. 14(2):166-74. http://bases.bireme.br/cgi-bin/wxislind.exe/iah/online/?IsisScript=iah/iah.xis&src=google&base=BDENF&lang=p&nextAction=lnk&exprSearch=19533&indexSearch=ID
33. Lopes MEL. Praxiologia, representação social de menopausa e práticas educativas de enfermeiras na estratégia saúde da família [doctoral thesis]. Natal: Universidade Federal do Rio Grande do Norte; 2009.
34. Melo VH, Rio SMP, Bonito RF, Lodi CTC, Fonseca MTM, Amaral E. Dificuldades dos médicos que atuam na Estratégia Saúde da Família de Minas Gerais para proverem atenção à saúde das mulheres. Rev Bras Med Fam Comunidade [Internet] 2014 [cited on 2014 Sep 14]. 9(30):3-12. Available from: http://dx.doi.org/10.5712/rbmfc9(30)550
35. Ministério da Saúde (Br). Portaria n°. 278, de 27 de fevereiro de 2014. Institui diretrizes para implementação da Política de Educação Permanente em Saúde, no âmbito do Ministério da Saúde. Diário Oficial da União, fev 2014; Seção 1.
36. Garcia NK, Gonçalves R, Brigagão JIM. Ações de atenção primária dirigidas às mulheres de 45 a 60 anos de idade. Rev Eletr Enf [Internet] 2013 [cited on 2014 Sep 14]. 15(3):713-21. Available from: http://dx.doi.org/10.5216/ree.v15i3.18529
37. Santos DAS; Moreira MA. Ações das enfermeiras em unidades de saúde da família sobre a saúde da mulher climatérica. Arq Ciênc Saúde [Internet] 2014 [cited on 2014 Sep 14]. 21(1):36-41. Available from: http://www.cienciasdasaude.famerp.br/racs_ol/vol-21-1/ID-564-21(1)-(Jan-Mar%202014).pdf
38. Madeira KH. Práticas do trabalho interdisciplinar na Saúde da Família: um estudo de caso [master degree]. Itajaí: Universidade do Vale do Itajaí; 2009.
39. Mattos GCM, Ferreira EF, Leite ICG, Greco RM. A inclusão da equipe de saúde bucal na Estratégia Saúde da Família: entraves, avanços e desafios. Cien Saude Colet [Scielo-Scientific Electronic Library Online] 2014 [cited on 2014 Sep 14]. 19(2):373-82. Available from: http://dx.doi.org/10.1590/1413-81232014192.21652012
40. Escorel S, Giovanella L, Mendonça MHM, Senna CM. O Programa de Saúde da Família e a construção de um novo modelo para a atenção básica no Brasil. Rev Panam Salud Publica [Scielo-Scientific Electronic Library Online] 2007 [cited on 2014 Sep 14]. 21(2/3):164-76. Available from: http://dx.doi.org/10.1590/S1020-49892007000200011