RESEARCH ARTICLES
Social representations of quality of life in HIV/AIDS: the role of time since diagnosis
Rodrigo Leite HipolitoI; Denize Cristina de OliveiraII; Antonio Marcos Tosoli GomesIII; Tadeu Lessa da CostaIV
IPhD in Nursing Student at the Nursing School of the State University of Rio de Janeiro. Assistant Professor of Nursing College at Universidade Federal Fluminense. Rio de Janeiro, Brazil. E-mail: professorrlh@uol.com.br.
IIProfessor, Department of Fundamentals in Nursing and the Post-Graduate Nursing School of Nursing School at the State University of Rio de Janeiro. Brazil. E-mail: dcouerj@gmail.com.
IIIProfessor of Medical Surgical Nursing Department and Graduate Program in Nursing at the Nursing School of the State University of Rio de Janeiro. Brazil. E-mail: mtosoli@gmail.com.
IVAdjunct Professor at the Nursing and Obstetrics Course of the Federal University of Rio de Janeiro. Macaé, Rio de Janeiro, Brazil. E-mail: tadeulessa@yahoo.com.br.
DOI: http://dx.doi.org/10.12957/reuerj.2014.12840
ABSTRACT: This qualitative, descriptive study, guided by the framework of the Theory of Social Representations, examined quality of life and its representations at different times from diagnosis. Individuals seropositive for human immunodeficiency virus (HIV) and enrolled in the STD/AIDS and Viral Hepatitis Program in a town in Rio de Janeiro State were subject to semistructured interviews between May 2013 and January 2014 and stratified by time since diagnosis. This resulted in two groups of twenty subjects each. In lexical analysis operationalized by Alceste software, quality of life in view of the diagnosis emerged in its broader context, revealing five categories. The representational profile of quality of life was found to tend towards positive aspects and resignification supported by new symbols attributed to the object AIDS.
Keywords: Quality of life; human immunodeficiency virus; acquired immunodeficiency syndrome; nursing.
INTRODUCTION
This article consists of a cutout of the thesis Quality of life of people living with HIV/AIDS in a city in the Lowland Coastal in the State of Rio de Janeiro developed in the Graduate Nursing Program at the State University of Rio de Janeiro.
Understanding the quality of life (QOL) of those living with HIV/Acquired Immune Deficiency Syndrome (AIDS) from objective and subjective spheres, is a major challenge, requiring it to be no reductionism to the topic, since it is noticed constant inter-relationships between the elements of this universe1. The increased survival of people living with HIV/AIDS (PLWHA) leads to new sources of uncertainties caused by the renegotiation that they need to do in relation to their feelings of hope and direction for the future, their social roles and identities, their interpersonal relationships and their QOL2.
The World Health Organization (WHO) defines QOL as a "perception that the individual has in relation to their position in life, culture and value systems in which they live, and also in relation to their goals, expectations, standards and concerns”3:25. It can be said that the infection affects various aspects of QOL of PLWHA, influencing physical, psychological aspects, the level of independence, social relationships, environment and spirituality, religiosity and personal beliefs4. However, it is noticed that individuals find ways to adapt and learn to live with it, contributing to that there are changes in the way of interpreting it5.
Studying the social representation (SR) of QoL in this group can provide knowledge of the symbolic setting of the phenomenon and ways of seeing and thinking HIV/AIDS, relevant to the various discussions that have been made in the health field today. Considering the arguments, it is admitted the hypothesis that the time of diagnosis and living with HIV/AIDS carry differences in the RS content of QOL
Given these observations, it was established as objective of this study to analyze QOL and its representations in different diagnostic moments, among PLWHA in a municipality in the lowlands coastal of the state of Rio de Janeiro.
THEORETICAL-METHODOLOGICAL
This is an exploratory, descriptive and qualitative study. The analysis was supported by the Social Representations Theory (SRT)6, using the procedural approach7, given that it emphasizes the process of constitution of representations, although it also affirms the importance of its product, namely, content8.
People with HIV that met the following inclusion criteria were screened: equal to or older than 18; registered in the Sexually Transmitted Disease Program (STDs), AIDS and Viral Hepatitis in the city of Rio das Ostras/RJ, possessing clinical and psychological conditions to respond to the research instruments. This was done during the period from May 2013 to January 2014.
For this study, it was defined a non-probability convenience sampling of 20 people with time diagnostic of at least six months. The subjects were invited to participate in the study while awaiting a medical consultation in the waiting room, taking into consideration the time since diagnosis, which was revealed soon after acceptance to be part of the study. The participation of the subjects obbeyed the Resolution Nº. 196/96 of the National Health Council (NHC) and the study was approved by the Research Ethics Committee of the State University of Rio de Janeiro (UERJ) Nº 073/2012 and protocol code number 066.3.2012. Participants read and signed the Informed Consent Form (ICF).
Data collection was conducted through interviews with the help of two instruments: a structured questionnaire to characterize the subjects, composed of socioeconomic variables, and a semi-structured script that investigated the understanding of QOL, identifying concepts and different conceptions of PLWHA, as well as the feelings, metaphors, images and existing values. It was intended to address how the subjects conceive the impact of seropositivity on QOL, from the time of diagnosis until the current stage of the disease. The record was made through MP3 audio and later its transcription. The subjects were coded as (I for Interviewee) in numerical order.
For data analysis, we used the ALCESTE 4.10 software that is intended to perform, automatically, the lexical content analysis through quantitative treatment techniques of textual data. This technique, in addition to describe the distribution laws of vocabulary, allows the study of representation types in the text. From this perspective, it distances itself from traditional modes of distribution of words by the use of statistical approach that includes the regularity of the distribution of the word in the elementary context units (ECU)9.
The transcribed material was standardized constituting a corpus of analysis into the software in plain text format9. Socioeconomic variables were coded in order to insert them into the corpus of analysis. The software held corpus treatment with its division into the ECU, as well as classes comprising them according to the lexical forms that comprised them9.
After cleavage of the corpus, 741 ECU, representing 64% success rate, were inserted into the classes in which corpus was divided by successive binary partition in hierarchical downward classification (HDC), the set of subjects’ interviews. In the present study, therefore, five classes emerged, which contain the SR content of the QOL of the group living with HIV/AIDS.
RESULTS AND DISCUSSION
The study group was characterized as having social vulnerability profile consistent with other investigations among PLWHA in Brazil. It was composed equally as regards the genders, with time of diagnosis less than 4 years (68%), on antiretroviral therapy (ART) (74%) and time of use of ART less than 4 years (52%), religious orientation Gospel (36%), and single (53%) with a mean age of 37 years old, having 2 or 3 children (35%), living mostly in the very city they receive health care (89%), sharing the house with up to 4 people (76%) of the family (82%), with low education level (48%), performing some employment activity (65%), the predominant family income ranging from R$ 701.00 to R $ 1,400.00 (33%) and having as main source of information about HIV/AIDS the very place of treatment (48%).
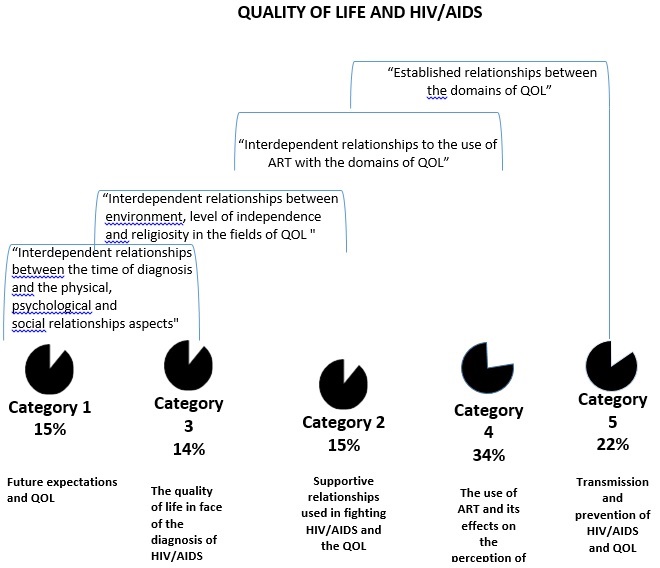
A breakdown of classes generated by software ALCESTE referring to the contents of SR of QoL was made by the successive order of thematic constitution, as shown in Figure 1.
FIGURE 1: Dendogram of distribution of categories generated by ALCESTE software. Rio das Ostras, RJ, 2014.
Category 5: Transmission and prevention of HIV/AIDS and QOL
Category 5 has 167 ECUs (22%), the first having arised after the binary division of the corpus. This category is the second largest within the HDC and presented as variable categories of higher statistical association people who do not use antiretroviral (ARV) and the time of diagnosis. We highlight that the variable time of diagnosis less than six months was presented among the most statistical association in class (x2=16), revealing that subjects stratified in this category showed a strong contribution to the representational content associated to the means of HIV transmission.
The reduced forms (words reduced to their radicals) with higher statistical association values to the category (the chi-quadrado-test - x²), were: sexual relation, condom, blood, transmit, transmission, transfus, origin, contamin.
However, the representational content located in the logic of prevention presented themselves as insufficient for a part of the group considering their individual and collective consequences. Women perceived themselves as affected, existing socio-cultural factors that interfere in the power relations as to the practice of safe sex decision. As a result of these decisions, some difficulties, such as guilt, emerged from their psychosocial content, revealing that sometimes modes of transmission have more social reasons than individual10. Later ECUs exemplify the class content:
The modes of transmission of HIV/AIDS are: sexually, by syringe, blood transfusion, mother to child during pregnancy and through cuts. (I14)
One day my husband said it was for me to trust him and not using condoms anymore, I trusted him and I was not preventing myself. (I4)
Category 4: The use of ART and its effects on the perception of QoL
Category 4 has 239 ECUs (34%), being considered the largest in the HDC. The categories of variables with greater statistical association were female gender and personal income from 3.1 to 5 minimum wages. The reduced forms associated were: antirretrovir, discovered, treatment, hospit, feed, consult, medicine, time.
It was noticed in this category that the representation of QoL was associated not only with the use of ART, but also to treatment in a broader conception, involving various dimensions of HIV/AIDS and life. The most positive associations of QoL were characterized by understanding the need for readaptation to the new daily habits and maintaining healthy behaviors for life. As a complement, although antagonic to the perceived needs, the main difficulties reported by the participants were associated with worse QoL, represented by pharmacological side effects, the routine imposed by schedule of medicines and problems with self-esteem.
The use of ART is perceived as provocative of positive consequences, since it is associated with better prospects in life, rather than the idea of death arising from the diagnosis. However, we emphasize that the side effects include relevant factor in the dynamics of use and adherence to ART, especially early in treatment4.
I do not feel incapable, do not feel sick. The ART is my life, because without it I would not be here. The only interference that ART has in my QOL is that there is a pill that makes me feel bad, the last of the day, because I take three tablets a day. (I2)
The day I received my HIV/AIDS diagnosis, I wanted to kill myself, but I had courage because there was a treatment, a cocktail of ARVs that I could take and be well. (I5)
Treatment adherence assumes, symbolically and concretely, the struggle for life, mobilizing a reason to live11. Thus, the meanings that individuals give to ARVs on HIV/AIDS by the need to adopt new ways of life, in a situation of confrontation with not wanting to make use of them, occasioned by the numerous consequences that might ensue, comprise one of the forms of apprehension of SRT. This apprehension was grounded in the sense that subjects users of ART, attach to the new context of life imposed by the current condition, reflecting the SR of QOL.
Category 2: Supportive relationships used in fighting HIV/AIDS and the QOL
Category 2 has 114 ECUs (15%) and presented as variable categories with greater statistical association: people in use of ART between two and five years (x2=16) and diagnostic time between two to five years. The reduced forms associated were: dst AIDS program, health professionals, relig, gospel, faith, great, cathol, church, support, spirit, hope.
In agreement with other studies, there was emphasis on representational content of QOL in the health sector in a comprehensive manner4. The convivial profile established between the subjects and the Program, plus a satisfactory response to local existing policies, revealed a representational content of QOL, positive and significant.
My relationship with health professionals in STD AIDS Program is great and this is important in QOL. They are great, attentive and I really have nothing to complain about the quality of care, at least not here with me. (I23)
Aspects related to habits and lifestyles, stress and coping strategies and social support are involved in the health-disease process12. The diagnosis contributed to reflections and questions, which have become a way to find a meaning in life and hence the cultivation of spirituality.
I think that without religion, today I would be dead, because when I found out I was with HIV/AIDS, if God had not sent that church woman to help me, I do not know how I would be today. (I2)
Placements related to spirituality can be highlighted as one of the variables present in the capacity of resilience and protection of health. Thus, we can see that the identified spiritual dimension was present in constructions of QOL meanings for the group in question, integrated in explanatory models of illness and ways of coping with the disease.
So, the fact that they are HIV positive with their psychobiological effects, does not imply that subjects could consider, from their way of knowledge developed, personal values and shared beliefs, a good QOL and high degree of satisfaction with health, contributing for the construction of a common reality to social set7.
Category 3: The quality of life in face of the diagnosis of HIV/AIDS
Class 3 has 106 ECUs (14%) and represented the group more focused in the theme of QoL in the analysis. The variable category with the highest statistical association was male. We notice the presence of the following reduced forms associated: quality of life, diagnosis, regular, worr, negative, HIV/AIDS, quiet, life, sexuality.
Participants of this category expressed the relationship of QOL with the diagnosis of HIV/AIDS. This relationship was revealed by the perception of care with themselves and their health in the time of disgnosis, as well as expore to feelings related to changes imposed by the context of relationships and also reflections on sexuality. Self-care showed up mainly in changing daily habits and activities after diagnosis, in an attempt to provide themselves physical well being, although the emotional aspect has not been discarded. This position suggests a redefinition resulting characteristic of the disease process, manifesting itself in feeling good, even before the disease and can be translated into a sense of personal growth and emotional improvement.
I do not think the HIV/AIDS diagnosis will impact my QOL, on the contrary, it will further improve my QOL over the years because I will take more care of me. (I 25)
It can be said that QOL, in the context of seropositivity, runs through a combination of individual and social factors that can come from family, friends and of religion itself, resulting in an interpretation that may be more positive or less positive of QoL, which also depends on individual attributes. Similar perceptions were found in other studies13.
My QOL after HIV/AIDS is good because I value peace, despite these negative things, I try to think the good things of things. Living! I think so. I am living the same way I used to live before knowing my HIV/AIDS, I did not let it affect me. (I40)
The concern with the revelation of the diagnostic, as shown in the statements, adversely affects QOL due to the fear of making public a condition that may predispose to prejudice and stigmatization. However, when the support of family and friends is present, this adaptation to new life becomes easier to be seen and reflections in the improvement of QOL become more evident. It was observed that some subjects tended to naturalize living with HIV and such cognitive constructions were not perceived as an escape from the situation, but as adaptation and acceptance of seropositivity, as observed in other studies10.
It was identified that sexuality itself plays an important role in their lives and has a relationship with QOL, as it affects various dimensions, from issues related to sexual dysfunction by the use of antiretroviral drugs, interference with self-esteem and even loss of libido, among others. According to the data, sexuality is an important element with which the PLWHA are confronted14.
My QOL suffered impact on physical aspect, nowadays I have been feeling tired, I have lost a bit of the willingness I used to have before HIV/AIDS. This, that enthusiasm to go further during sex, you go but you will have to go back. The HIV/AIDS changes our sexuality aspect, it changes too much. (I13)
Category 1: Future expectations and QOL
Category 1 has 115 ECUs (15%) of the corpus analyzed, representing the third category in number of ECUs. The variable category with the highest statistical association was time of use of ART between 7 months to 1 year and 11 months. It is noted the presence of the following short forms: want, worse, future, get, children, will, stud, death, prejudice, family, alene, wotk, joy, mate and parents.
Study participants were able to express their expectations for the future within the current living context, relating both the circumstances surrounding the family, such as those concerning the relationship with work and other life situations in a broader social scene. It was identified a positive speech and hope deposited in the hereafter. The possibility of developing good expectations and enjoying good health, similar to non-carriers of the virus, results in better acceptance of seropositivity condition and greater adaptation, which ultimately reflect on QoL.
Therefore, the importance of life in the context of HIV/AIDS is found, by many participants, through the children. The person with HIV also sees in the children a reason to continue living as they feel the need to take care of them and accompany them in their growth, becoming therefore a source of strength to live13.
For the future, I ask God to give me health to see my grandchildren, the happiness of my three children and my two grandchildren. (I5)
However, among respondents we observed ECU expressing mixed feelings of dissatisfaction with the current condition and difficulties in designing long-term dreams. It is observed that QOL for the group is not only related the possibility of longer life, because living in this condition is still faced with situations of discrimination, abandonment, segregation, stigmatization and rupture of affective relationships. Against this background, facing the disease becomes complicated and, as a result, QOL may be affected15.
Anyway, I do not know if my feeling now is a state of permanence, but now I do not expect anything of the future. (I38)
A feature found in the group, and common to many others in similar situations, is separation of home and family. The concern reports of being judged by the family, is correlated with the docking of AIDS in moral corruption7 The association made by some interviewees stating that their QOL could be better if there were no prejudice, refers to the idea of minorities who feel devalued before a majority within a society, which distinguish and mark in its asymmetry16.
Ending prejudice would improve the QOL of those living with HIV/AIDS, so I could return to be close to my family, because I think a lot about going back, but I think a lot in being discriminated. (I2)
Concerns related to working scenario were also present in discourse analysis, and can be spread on two axes: a more positive character, which favors a better QOL to provide better financial conditions and offer stability, credibility and psychosocial occupation; and another more negative character axis, in which the work is associated with a reduction and/or loss of ability17.
CONCLUSION
The results were characterized by the transition from negative to positive meanings associated to HIV/AIDS, with the introduction of the possibility of living with the disease, as well as its impact on QOL with the removal of impending death.
As to the temporal interference hypothesis in SR of QOL, it is concluded that cognitions alluding to better QOL in both groups emerged. However, considering that the level of knowledge from the reified universe can contribute to rethink stigmas, remove myths and improve adherence to treatment, it is emphasized that the group with shorter living with the virus presented content concerning the transmission that may influence the thinking of QOL in the context of HIV/AIDS. Similarly, subjects with more time since diagnosis had representational content anchored in religion, which may contribute to the redefinition of the disease and reorientation of expectations and life projects.
Thus, experiencing condition of seropositivity, represents, on itself, a reworking of various processes, especially those conditioned to maintain a good mental health and that, together with a psychosocial and spiritual support network since the time of discovery of diagnostic, would markedly contribute to the improvement of QOL.
We observed in these results cognitive contents identified as central to the SR of AIDS as in other studies of SRT and HIV/AIDS, such as prejudice, family, health professionals and the ART. Therefore, such considerations reinforce the idea that SR of QOL are not autonomous in relation to SR of AIDS.
While it may not be possible to generalize our findings to other populations and regions of the country, they provided an overview of the SR of QOL and its relationship with socioeconomic and clinical aspects of PLWHA in the context of internalization, in a city of State of Rio de Janeiro. Also, it can provide useful information to support health policies in the region.
REFERENCES
1.Almeida MAB, Gutierrez GL, Marques R. Qualidade de vida: definição, conceitos e interfaces com outras áreas, de pesquisa. São Paulo: Escola de Artes, Ciências e Humanidades; 2012.
2.Castanha AR, Coutinho MPL, Saldanha AAW, Ribeiro CG. Aspectos psicossociais da vivência da soropositividade ao HIV nos dias atuais. PSICO. 2006; 37(1):47-56.
3.Fleck MPA. Problemas conceituais em qualidade de vida. In: Fleck MPA, organizador. A avaliação da qualidade de vida:guia para profissionais da saúde. Porto Alegre (RS): Artmed; 2008. p.19-28.
4.Costa TLD. Representações sociais do HIV/Aids e da qualidade de vida: um estudo entre pessoas que vivem com o agravo em contexto de interiorização [tese de doutorado]. Rio de Janeiro: Universidade do Estado do Rio de Janeiro; 2012.
5.Meirelles BHS, Silva DMGV, Vieira FMA, Souza SS, Coelho IZ, Batista R. Percepções da qualidade de vida de pessoas com HIV/Aids. Rev RENE. 2010; 11(3):68-76.
6.Moscovici S. O fenômeno das representações sociais. In: Moscovici S. Representações sociais: investigações em psicologia social. Petrópolis (RJ): Vozes; 2003. p.29-109.
7.Jodelet D. Representações sociais: um domínio em expansão. In: Jodelet D, organizadora. As representações sociais. Rio de Janeiro: EDUERJ; 2001. p.17-44.
8.Sá CP. A construção do objeto de pesquisa em representações sociais. Rio de Janeiro: EdUERJ; 1998.
9.Oliveira DC, Gomes AMT, Marques SC. Análise estatística de dados textuais na pesquisa das representações sociais: alguns princípios e uma aplicação ao campo da saúde. In: Menin MSS, Shimizu AM, organizadores. Experiência e representação social: questões teóricas e metodológicas. São Paulo: Casa do Psicólogo; 2005. p.157-200.
10.Gomes AMT, Silva EMP, Oliveira DC. Social representations of AIDS and their quotidian interfaces for people living with HIV. Rev Latino-Am Enfermagem. 2011; 19:485-92.
11.Espírito Santo CC, Gomes AMT, Oliveira DC, Marques SC. Adesão ao tratamento antirretroviral e a espiritualidade de pessoas com hiv/aids: estudo de representações sociais. Rev enferm UERJ. 2014; 21:458-63.
12.Seidl EMF, Zannon C, Tróccoli BT. Pessoas vivendo com HIV/Aids: enfrentamento, suporte social e qualidade de vida. Psicologia: Reflexão e critica. 2005; 18:188-95.
13.Espírito Santo CC, Gomes AMT, Oliveira DC. A espiritualidade de pessoas com HIV/aids: um estudo de representações sociais. Rev Enf Ref. 2013; 10:15-24.
14.Gonçalves TR, Carvalho FT, Faria ER, Goldim JR, Piccinini CA. Vida reprodutiva de pessoas vivendo com HIV/Aids: revisando a literatura. Psicol soc. 2009; 21:223-32.
15.Galvão MTG, Cerqueira ATAR, Marcondes-Machado J. Avaliação da qualidade de vida de mulheres com HIV/Aids através do HAT- QoL. Cad Saúde Pública. 2004; 20:430-7.
16.Moscovici S. Preconceito e representações sociais. In: Almeida AMO, Jodelet D, organizadores. Representações sociais: interdisciplinaridade e diversidade de paradigmas. Brasília(DF): Thesaurus; 2009. p.17-34.
17.Castanha AR, Coutinho MPL, Saldanha AAW, Ribeiro CG. Avaliação da qualidade de vida em soropositivos para o HIV. Estud psicol. 2007; 24(1):23-31.