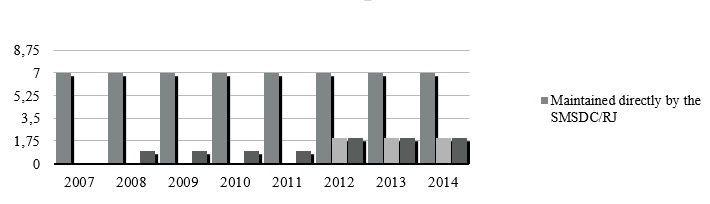
FIGURE 1 : Birth care establishments in the city of Rio de Janeiro according to sustaining entity
Key: SMSDC/RJ - Municipal Department for Health and Civil Defense of Rio de Janeiro
SO - Social Organization
Source: CNESNET, 2014.
RESEARCH ARTICLES
Healthcare and productive restructuring: effects of increased flexibility on maternity hospitals in the Cegonha Carioca program
Jane Márcia ProgiantiI; Juliana Amaral PrataII; Pedrita Machado BarbosaIII
I
Ph.D in Nursing. Associate Professor of the Department of Mother and Child Nursing, Faculty of Nursing, Researcher in the Research Group on Gender, Power
and Violence in Health and Nursing, Researcher of the Prociência Program of Rio de Janeiro State University. Brazil. Email: jmprogi@uol.com.br
II
M.A in Nursing. Doctoral student of the Faculty of Nursing, Rio de Janeiro State University. Brazil. Email: juaprata@gmail.com
III
Undertaking M.A, Faculty of Nursing, Rio de Janeiro State University. Brazil. Email: barbosa.pedrita@gmail.com
DOI: http://dx.doi.org/10.12957/reuerj.2015.12540
ABSTRACT
This documentary study conducted on Brazil's National Register of Health Facilities (CNES) database discussed the effects of productive restructuring on municipal maternity hospitals in the Cegonha Carioca Program, and thus on nursing. The process fostered more flexible service management, which in turn enabled the network of labor care facilities to expand through partnerships and management contracts. In human resource terms, more jobs were created for nurses to work in maternity hospitals, and diverse new types of employment relationship emerged. It was concluded that, although this program does represents significant expansion in the labor market, it reasserts public sector flexibilization by permitting fragile employment relationships, thus contributing to labor instability. In this scenario, regulation and professional development for these professionals pose challenges for managing the implementation and continuity of public childbirth care policies.
Keywords: Obstetric nursing; work; humanization of care; policy.
INTRODUCTION
In the beginning of the 1970s, the transformations in capitalism led to a worldwide crisis, characterized by the exhaustion of the Fordist model of production, which lasted until the end of the decade, when the neoliberal ideology conquered the developed countries and was shown to be the ideology most appropriate for supporting globalization and productive restructuring, processes which constituted a response to the crisis in Fordism, and in the reconfiguration of the capitalist mode of accumulation1-3.
Neoliberalism brought proposals which aimed to reform the social welfare States, including containing social costs, privatizations of nationalized companies or industries, flexibilization of the work, and deregulation of the market4,5. In parallel, globalization contributed to the neoliberal advance, through allowing the mobility of capital at a global level6. These processes benefited from the productive restructuring which, based on structural transformations in the ambit of production work, introduced new standards of management and organization in these sectors 1,2.
As a principal characteristic of productive restructuring, flexibility translates into the liberation of the production based on the just in time method, involving rationalization, efficiency and cost reduction. Accompanying this conception, the market is configured through the flexibilization of the working days, the remuneration and the social rights, changing the professional training through proposals which involve the development of skills and competencies, with a view to the constitution of a qualified workforce2,7,8.
In spite of being distinct phenomena, neoliberalism, globalization and productive restructuring are articulated through the transformations which have been occurring in capitalism in recent decades, as they share the ideal of flexibilization in the varying sectors of society3,4.
In the perspective of the management of Brazilian health, in spite of the consolidation of the Unified Health System (SUS), the policy of economic adjustment, implanted in the 1990s, determined the reduction of costs and of financing, the absence of investments, and underpayment for services and professionals, resulting in a drop in the quality of the care4,9.
This panorama catalyzed the confrontation among the conceptions regarding the role of the State, and the standard intervention on society, favoring the appearance of new models of management of health units, which resulted in the deregulation of the labor relations10-13. Hence, with the promise of debureaucratization and efficiency of public management, capitalism, through financialization, instituted productive restructuring in the health field, based on the flexibilization of the structures and forms of organization of labor relations14,15.
Besides these effects of productive restructuring, in the dimension of health production, this process has to do with changes in the way of producing care, based on innovations in the productive systems16,17. Thus, in spite of the hegemony of the medical practices, which transformed Brazil into one of the champions in terms of cesarean sections, the obstetric field has been changing based on the valorization of a work process centered on the living labor and the use of light technologies to the detriment of focus on the dead labor and on hard technologies, in which nursing has contributed to re-signifying the way of caring in obstetrics.
In the light of the above, with the aim of contributing to reflections regarding the repercussions of this new configuration of the market on the process of nursing work, we propose to discuss the effects of productive restructuring in the municipal maternity hospitals of the Cegonha Carioca Program and its nexuses with nursing.
METHODOLOGY
This is a documentary study undertaken using the National Health Facilities Census (CNES), specifically, the nominal search for establishments18 . This survey considered the period available from 2007 – 2014, operationalized through the consultation with the establishments' technical files, with emphasis on the maintaining entity, and on the annual consultation of professionals by competency, using the expression nurse so as to recover the quantity of nurses recorded on the system and the labor relation established with the institutions.
Based on the Brazilian Classification of Occupations (CBO), we used the word nurse instead of obstetric nurse, as, as weak points of the study, we had difficulties in identifying – in some maternity hospitals – the nurses who worked specifically in the area of obstetrics. In addition to this, as the CBO recorded on the system is not always consistent with the work profile of these professionals in practice, we opted for the expression nurses who work in maternity hospitals for the analysis and discussion of the data.
As the inclusion criteria, we adopted the municipal maternity hospitals of the Cegonha Carioca Program, consulting the website of the Municipal Health Department of the Prefecture of Rio de Janeiro (SMSDC/RJ). Thus, we found one birth center, six maternity hospitals, and four general hospitals which had maternity units19.
As exclusion criteria, particularly for the discussion of the labor relations of the nurses who work in maternity hospitals, we considered the weaknesses found in the database and excluded those establishments considered general hospitals.
For analysis of the data, we use publications of the Brazilian Institute of Geography and Statistics (IBGE) and of the Human Resources Observatory 20-24.
RESULTS AND DISCUSSION
Based on the survey in the CNES, two categories of analysis emerged as effects of the productive restructuring in the municipal maternity hospitals of the Cegonha Carioca Program: increase in the network of establishments for birth care, and the appearance of different modalities of labor link for the nurses who work in maternity hospitals.
Increase in the network of establishments for birth care
Since the 2000's, a broadening of the care network has been verified in all the administrative spheres and in the different levels of care25. In this regard, data from the IBGE point to the appearance of new health establishments in Brazil, with emphasis on the municipal and private network 20-22.
This increase took place as a response to the need for the expansion of the SUS, in a context marked by the decentralization of the services to the states and municipalities. However, the issue of the financing of the policies appeared as a challenge for putting a quality public service into effect, given that the neoliberal reforms characterized by social cuts resulted in redefining the role of the State4,25.
This situation intensified with Constitutional Amendment N. 19/1998, which implemented administrative reform, configuring the concept of flexibility in health and in Labor Relations in the public sector4,10-12,25. Among the modifications introduced by this legislation, emphasis is placed on the following: the reviewing of the stability of the statutory civil servants, the changes in the system for remuneration of public officials and the introduction of the executive agencies and the social organizations (SO) in public management26.
This last point of the reform entailed significant changes in the structure and the dynamics of the services, as it allowed the establishment of consortiums and agreements of cooperation in the ambit of the Union, the States and the Municipalities. As a result, it viabilized associated management, as well as the total or partial transferences of expenses, services, staff and essential goods14.
This regulation allowed the appearance of mechanisms of flexibility, which, gradually, were adopted by the management of the health services, and for the contracting of staff. This being the case, in the light of the policy of reduction of the State, the local governments, although opposed to the reform, adopted flexibility in the public sector, mainly through partnerships with non-profit-making entities and SO4,10-12,14.
In the perspective of the health policies, the network's expansion, accompanied by the flexible tendency in the management of the services and of the human resources, can be verified in the Family Health Program and in the Cegonha Network, as initiatives of the Ministry of Health (MS), operationalized by the municipal administration, which were born in the ambit of these new managerial formats, presenting varying models of institutional link 11,14,25,27,28.
The Cegonha Network was launched in 2011, and Rio de Janeiro was a pioneer in the implementation of the strategy, which seeks to organize a network of care for women and children, involving the three administrative spheres29. This new model calls for the financing of reforms, extensions and acquisitions through passing on funds from the Union and private participation through social health care charities30.
To this scenario of flexibilization in the public sector and in parallel with the Cegonha Network, one can add the creation of the Cegonha Carioca Program in the municipality of Rio de Janeiro, characterized by the linking of the prenatal consultation to the maternity hospitals, transport, embracement and classification of risk by the nurse31. These initiatives have led to partnerships and established varying labor relations, as well as investing, through the National Residency in Obstetric Nursing Program, in the training of specialist nurses for their later insertion in the SUS 15,27,32.
As an effect of these new modalities of management which consolidate the advance of productive restructuring of public health, currently, the obstetric field of the municipal network of Rio de Janeiro has 11 establishments for assistance with birth inserted in the Cegonha Carioca Program, these being 10 Maternity Hospitals and one Birth Center, with nurses working in all these units.
Observing the period 2007 – 2014, in Figure 1, one can perceive that the increment in this administrative sphere, verified in the obstetric field, occurred based on various management arrangements of the institutions.
FIGURE 1
: Birth care establishments in the city of Rio de Janeiro according to sustaining entity
Key: SMSDC/RJ - Municipal Department for Health and Civil Defense of Rio de Janeiro
SO - Social Organization
Source: CNESNET, 2014.
We observed that, until 2007, the SMSDC/RJ directly managed all the childbirth care establishments, demonstrating that, until that time, the managers had not adopted flexibilization in the managerial structures, although this process had been legitimated by federal provisions since 1998.
From 2008, we verified that there was a gradual broadening of the care network, accompanied by partnerships with non-profit-making entities and with SO. This modality of associated management intensified with the publication of Law N. 5.026/2009, which regulated the functioning of SO in the management of health units33. In the light of this apparatus and the incentives of the Cegonha Network and the Cegonha Carioca Program, we can infer that the flexibilization was accepted by the municipal management, resulting, in the ambit of childbirth assistance, in the creation of three new municipal units.
In this regard, it may be noted that the flexible model adopted for the management of the municipal maternity hospitals increased the number of positions, such that, by 2007, the number of nurses working in the establishments for childbirth care was 275, reaching a total of 607 by June 201418.
Appearance of different labor links for the nurses in maternity hospitals
In Brazil, although regulation of labor is guaranteed by the Consolidation of Labor Laws (CLT), the deregulation of the market viabilized the establishment of contracts, which were often poor. In the public sector, the phenomenon of the flexibilization of the forms of work conform with the defining of the role of the State as a regulator, based on the transformations introduced by Constitutional Amendment N. 19/1998, which allowed the appearance of new modes of link for the human resources10-12.
Added to this provision, the containing of costs with staff in the public sector intensified, in 2000, with the Fiscal Responsibility Law, which regulated the costs in the administrative spheres, specifying the highest percentage for the municipal level34.
In the ambit of health, accompanying the tendency of labor relations of other sectors, the flexible contracting practices found a favorable environment in the light of the policy of reining in the machinery of state allied with the processes of decentralization and municipalization, as well as the new policies and programs for local undertaking14,35. This scenario caused changes in the form of contracting and structuring of the workforce such that the municipal public administration was induced to contract professionals through atypical arrangements4,10,11,35,36.
Subsequent to the productive restructuring in the field of health, the flexibilization of the management of human resources contributed to the labor market of the nurses being configured heterogeneously. In the work microspaces, it may be perceived that the workforce conforms in a fragmented way in relation to the type of labor link, to the managerial structure, and even in terms of salary10.
In this regard, the municipal maternity hospitals of the Cegonha Carioca Program are presented as exemplary scenarios of consolidation of flexible management in the services and in the human resources. Furthermore, as a recommendation of the public policies, this Program invests in the work of nurses in care during labor and birth, although the SMSDC/RJ has been adopting alternative practices to contracting these professionals15.
In observing the evolution of labor relations of nurses in the maternity hospitals of the SMSDC/RJ, in Figure 2, in the period 2007 – 2008, there was a proportional inversion of various links for the statutory scheme, which suggests the permanent contracting of workers for the public service. It is noteworthy that, in 2008, an open public examination was held for the post of nurse, to be called up until 2012, explaining the increase verified in the statutory scheme in the decline of the various links in this interval.
In spite of this attempt at regulating labor links in the maternity hospitals, from 2011 onward, subsequent to the Cegonha Carioca Program and the appearance of new units, there was a significant increase of various links, although from 2013 until the beginning of 2014, this modality of link begins to present a tendency for reduction for the coming years, given that a new open public examination took place in 2013, increasing the numbers of permanently-contracted nurses who work in maternity hospitals.
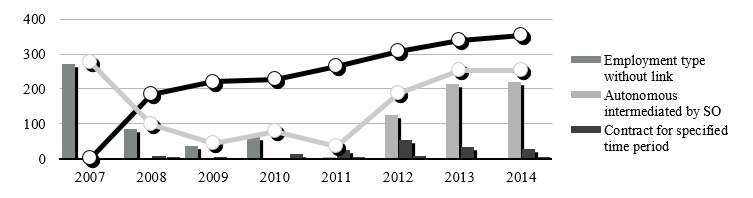
FIGURE 2
: Evolution of the labor relatos of curses in the birth care establishment of the SMSDC/RJ (2007 - 2014)
Key: SO - Social Organization
Source: CNESNET, 2013.
Note: The modelizeis of labor link which were numerically little significant werw included as "others links": cooperative, public employment CLT,
autônomos, working for the state and verbal/informal contract.
Taking into account the entity which maintains the maternity hospitals and the type of the labor link established with the nurses, we perceive that, in spite of the statutory scheme prevailing as the main form of link, Figure 2 points to the proliferation of unstable links in recent years, in which atypical forms of work are the majority in institutions, where the SMSDC/RJ established partnerships and management contracts.
With the exception of the Birth Center which only has nurses under the statutory scheme, in the four maternity hospitals administered directly by the SMSDC/RJ, concomitantly with the predominance of the civil servant scheme, we verified the existence of other modes of labor relation, with emphasis on temporary contracts and professionals intermediated by SO. On the other hand, in the two establishments managed by SO, all nurses of these institutions had a labor link termed autonomous intermediated by Social Organization.
In relation to the contracts for specified time, Figure 2 presents the persistence of this type of labor link over the years, denoting a certain banalization of the legislation, which allows this type of contracting only to resolve situations of exceptional public interest, with specified or predictable duration, which cannot be met, at the time, with human resources from the public administration4,12,37. However, temporary contracting, as a constant in the situation of human resources of the SMSDC/RJ, is illegal when configured as a substitute for an open public examination and an effective link.
We also note the considerable increase of contracting under autonomous intermediated by SO as a consequence of flexible management which, in the municipality of Rio de Janeiro, is materialized in Law N. 5.026/2009. This provision relates to the function of SO in health, only in the units created since the publication of the above-mentioned law33. Hence, based in this legal apparatus, in 2012 and 2013, the municipality inaugurated two new maternity hospitals, responsible for the significant growth in this type of labor relation in the last three years.
In the period observed, the SMSDC/RJ has been simultaneously using different forms of link for the nurses, which may be characterized as protected work or typical employment and unprotected work or atypical employment. The first group possesses legal coverage, social protection and a labor relation which is not limited in terms of time, corresponding to the statutory scheme and to the CLT. On the other hand, the second group includes the set of temporary links, providers of autonomous professional services and other types of contracts which share weakness and absences of stability in the employment, without full protection in the ambit of legal rights36.
This plethora of labor contexts relates to the notion of instability, as a phenomenon of weakening and loss of quality of the market, resulting from the neoliberal reforms which accentuated the flexibilization and deregulation of the work, the unemployment, and the levels of informality in the labor relation36. As a specific characteristic of the economic development in late capitalism, the flexibilization of work, and the process of reducing job security, associated with lack of socio-legal protection, are presented as inevitable for the workers who, so as to avoid socially excluding unemployment, submit themselves to the unstable labor relations3,25.
In this regard, the fragmentation of the links with the public administration of the health services is related to the instability of the work in the SUS. From the point of view of the link, the instability lies in the gaps in the protection of the rights and benefits of the worker, while, from the legal perspective, the failure to respect the norms of entrance into the institutions of the State configures an irregularity of the link in its origin11,14,35.
In the micro-spaces of work of the SUS, the coexistence of different strata of workers generates instability in the job positions, compromising the professionals and institutions. In this scenario, the reduction in job security is visible in the physical and psychological exhaustion, in the demotivation, in poor performance, in absenteeism, and in lack of commitment to the establishment and to the quality of the care. On the other hand, as an effect of this process, the high turnover in the services is a context which affects the continuity of the public policies and the healthcare programs 4,10,11,15,25,35.
In the current panorama of the management of human resources in health, the absence of single legislation supporting these fragile labor arrangements, in the different Brazilian states, hinders the regulation of atypical employments. The existing norms are locally specific and are based on the evaluation of the achievement of preestablished goals, without there being regulatory norms for admission, dismissal and performance of the workers10,11,25.
Considering that it is a consensus among managers and workers that the training, performance and management of human resources profoundly affect the quality of the public services, the regularization of the labor links in the SUS appears as an urgent question. To this end, in 2003, the Ministry of Health set up the National Interinstitutional Committee for the Reduction of Job Insecurity in the SUS in order to develop policies and formulate guidelines for confronting this issue35.
The governmental initiatives in the field of management of the work resulted, in 2006, in the publication of the National Program for the Reduction of Job Insecurity in the SUS, with a view to sensitizing, and raising awareness among, managers regarding the importance of the policy of valuing the worker as a strategy for promoting the reduction of job insecurity and the consolidation of the SUS25,35.
In this regard, with the aim of combating the instability of the work in health in the SUS, the municipality of Rio de Janeiro established some objectives; among these, emphasis is placed on investing in the qualification of professionals and in reducing turnover among them. In 2013, however, in spite of the efforts, the indicator proportion of workers who work for the SUS, in the public sphere, with protected links did not meet the agreed goal of 92%, reaching 77.73%38.
Although the results are not in accordance with the expected tendency for reduction, it is interesting to note that the valorization and democratization of the labor relations in the SUS constitute part of the guidelines of the action plan of the municipality for the period 2013 – 2015.
We can infer, based in Figure 2, specifically in relation to the nurses who work in maternity hospitals of the SMSDC/RJ, that the consequences of these initiatives are promising for the year 2014, as the data point to a considerable reduction of flexible labor relations, although, for it to be possible to state this as a tendency, it is necessary that there should be, in the coming years, a proportional increase of typical and protected employments, mainly in the statutory scheme.
CONCLUSION
In Brazil, concomitantly with the consolidation of the SUS and the process of municipalization of healthcare, the strategies for confronting the crisis of world capitalism have resulted in administrative reforms, which have led to redefining the role of the State, as the undertaker of public policies with a social character.
Under the influence of neoliberalism, globalization and productive restructuring, the policy of the minimum State, implemented in the health field, has placed finance as an impasse for putting quality public service into effect, allowing the appearance of flexible models for the management of the services and the human resources in this area.
This flexibilization in the public sector allowed the establishment of partnerships and consortiums of cooperation, mainly in the states and municipalities, although it has brought new configurations to the labor market. If, on the one hand, these new modalities of management have led to the broadening of the network and of the job positions, on the other, they have corroborated the deregulation and reduction in stability of the labor relations in the SUS.
In this regard, the municipality of Rio de Janeiro is presented as an example of consolidation of the productive re-structuring in public health, as, in the light of the Cegonha Carioca Program, this administrative sphere entered into partnerships which allow the creation of new establishments for care in birth, as well as the increasing number of jobs offered for nurses who work in maternity hospitals. However, accompanying the tendency of other initiatives at the federal level, this Program is using atypical and unprotected links for the human resources.
In this perspective, although the Cegonha Carioca represents an important expansion of the labor market for nurses, at the same time, it reaffirms the flexibilization in the public sector, through adopting fragile labor relations, contributing to the destabilizing of the work in the SUS. Furthermore, in the light of the variety of labor relations existing in the SMSDC/RJ, the management of these professionals is configured as a complex question, in the plane of regulation and ongoing qualification, becoming a challenge for the implementation and continuity of the public policies for care in labor and childbirth.
In the light of the above, we suggest further studies to monitor the current efforts of the municipal managers so as to regularize the labor links in the SUS, with emphasis on the management of the human resources of the above-mentioned Program, as, as an initiative which values the work of nurses, it is important that it should take place also in the perspective of the labor relations, given that this issue is a determinant for the quality of the services and for the effectiveness of the actions, as well as for the regularity of the work in health.
REFERENCES
1.Gomes Serafim MT. Debate sobre a reestruturação produtiva no Brasil. RA'EGA. 2011; 21: 51-77.
2.Varella TC, Pierantoni CR. A migração de enfermeiros: um problema de saúde pública. Rev Bras Saúde Mater Infant. 2007; 7: 199-211.
3.Lustosa DSM. Flexibilização/precarização das relações de trabalho no Brasil. Âmbito Jurídico. 2010; [citado em 05 mai 2014]. 13 (75). Disponível em: http://www.ambito-juridico.com.br.
4.Souza MN. Flexibilização e precarização do trabalho no âmbito da saúde e educação. In: Anais da V Jornada Internacional de Políticas Públicas; 2011 ago 23-26; São Luís, Brasil. São Luís (MA): Universidade Federal do Maranhão; 2011. p. 2-9.
5.Munhoz DB, Jesus JAL, Costa MA, Souza EM. Neoliberalismo e Estado mínimo: repercussões na atenção à saúde no Distrito Federal. Com Ciências Saúde. 2009; 20:271-6.
6.Rocha-Vidigal CB. Vidigal VG. Investimento na qualificação profissional: uma abordagem econômica sobre sua importância. Acta Scientarum Human and Social Sciences. 2012; 34 (1): 41-8.
7.Estrada JHM. La formacíon por competencias y el mundo del trabajo: de la calificación a la empleabilidad. Rev salud pública. 2012; 14 (Suppl 1): 98-111.
8.Haddad AE, Morita MC, Pierantoni CR, Brenelli SL, Passarella T. Campos FE. Formação de profissionais de saúde no Brasil: uma análise no período de 1991 a 2008. Rev Saúde Pública. 2010; 44: 383-93.
9.Garcia AL, Oliveira ERA, Barros EB. Qualidade de vida de professores do ensino superior na área da saúde: discurso e prática cotidiana. Cogitare Enferm. 2008; 13(1):18-24.
10.Martins MIC. Molinaro A. Reestruturação produtiva e seu impacto nas relações de trabalho nos serviços públicos de saúde no Brasil. Ciência & Saúde Coletiva. 2013; 18: 1667-76.
11.Nogueira RP. Problemas de gestão e regulação do trabalho no SUS. In: Observatório de Recursos Humanos em Saúde no Brasil (Série Observação 5). Brasília (DF): Organização Pan-Americana da Saúde; 2010.
12.Ribeiro AB. Vínculos de trabalho na administração pública brasileira. Observatório de Recursos Humanos em Saúde no Brasil (Série Formulação 1). Brasília (DF): Organização Pan-Americana da Saúde; 2010
13.Prata JA, Progianti JM, Pereira ALF. O contexto brasileiro de inserção das enfermeiras obstétricas na assistência ao parto humanizado. Rev enferm UERJ. 2012; 20:105-10.
14.Nogueira RP. Composição público versus privado, gestão de unidades e recursos humanos no SUS. Observatório de Recursos Humanos em Saúde no Brasil (Série Observação 5). Brasília (DF): Organização Pan-Americana da Saúde; 2010.
15.Maia ACMSB. Programa Cegonha Carioca:dilemas conceituais/programáticos e expectativas na atenção pré-natal [dissertação de mestrado]. Rio de Janeiro: Universidade Federal do Rio de Janeiro; 2014.
16.Ferreira VSC, Andrade CS, Franco TB, Merhy EE. Processo de trabalho do agente comunitário de saúde e a reestruturação produtiva. Cad Saúde Pública. 2009; 25: 898-906.
17.Franco TB, Merhy EE. Atenção domiciliar na saúde suplementar: dispositivo da reestruturação produtiva. Ciência & Saúde Coletiva. 2008; 13: 1511-20.
18.Cadastro Nacional de Estabelecimentos de Saúde do Ministério da Saúde. Secretaria de Atenção à Saúde - DATASUS [base de dados na internet]. Última atualização em jul 2014. [citado em 14 jul 2014]. Disponível em: http://cnes3.datasus.gov.br/Lista_Prof_Nome_Sus.asp.
19.Prefeitura do Rio de Janeiro. Unidades de saúde. Maternidades da Secretaria Municipal de Saúde [site da internet]. [citado em 15 jan 2015]. Disponível em: http://www.rio.rj.gov.br/web/sms/maternidades.
20.Instituto Brasileiro de Geografia e Estatísticas. Estatísticas da Saúde: Assistência Médico Sanitária. Rio de Janeiro: IBGE; 2002.
21.Instituto Brasileiro de Geografia e Estatísticas. Estatísticas da Saúde: Assistência Médico Sanitária. Rio de Janeiro: IBGE; 2005.
22.Instituto Brasileiro de Geografia e Estatísticas. Estatísticas da Saúde: Assistência Médico Sanitária. Rio de Janeiro: IBGE; 2010.
23.Nogueira RP. Piola SF. Vianna SM. Rodrigues VA. Tendências na evolução do emprego e nas relações de trabalho em saúde: a gestão de recursos humanos no Sistema Único de Saúde. IN: Observatório de Recursos Humanos em Saúde no Brasil (Série Observação 5). Brasília (DF): Organização Pan-Americana da Saúde; 2010.
24.Nogueira RP. Ribeiro AB. Reflexões sobre diferentes temas: capital e trabalho nos serviços de saúde; o Estado, as agências e a saúde; vínculos de trabalho na administração pública brasileira. IN: Observatório de Recursos Humanos em Saúde no Brasil (Série Formulação 1). Brasília (DF): Organização Pan-Americana da Saúde; 2010.
25.Junqueira TS. Cotta RMM. Gomes RC. Silveira SFR. Siqueira-Batista R. Pinheiro TMM. Sampaio RF. As relações laborais no âmbito da municipalização da gestão em saúde os dilemas da relação expansão/precarização do trabalho no contexto do SUS. Cad Saúde Pública. 2010; 26(5): 918-28.
26.Senado Federal (Br). Lei n° 9.637, de 15 de maio de 1998. Dispõe sobre a qualificação de entidades como organizações sociais, a criação do Programa Nacional de Publicização, a extinção de órgãos e entidades que menciona e a absorção de suas atividades por organizações sociais e dá outras providências. Brasília (DF): Gráfica do Senado; 1998.
27.Inglez BN. Programa Cegonha Carioca: as implicações da contra-reforma neoliberal na saúde [monografia]. Rio de Janeiro: Universidade Federal do Rio de Janeiro; 2012.
28.Silva KL. Sena RR. Tavares TS. Maas LWD. Expansão dos cursos de graduação em enfermagem e mercado de trabalho: reproduzindo desigualdades? Rev Bras Enferm. 2012; 65: 406-13.
29.Secretaria de Estado de Saúde (RJ). Deliberação CIB n°1.375 de 21 de julho de 2011. Aprova a adesão do estado do Rio de Janeiro à Rede Cegonha. Rio de Janeiro: SES-RJ; 2011.
30.Ministério da Saúde (Br). Portaria n° 1.459, de 24 de junho de 2011. Institui, no âmbito do Sistema Único de Saúde, a Rede Cegonha. Brasília (DF): Gabinete Ministerial; 2011.
31.Secretaria Municipal de Saúde e Defesa Civil do Rio de Janeiro. Programa Cegonha Carioca: Edital, Anexos I, II, III, IV, A, B, C e D. [citado em 24 jan 2015]. Disponível em: http://www.rio.gov.br/web/smsdc/exibeconteudo?articleid=188976.
32.Governo Federal (Br). Secretaria de Gestão do Trabalho e da Educação na Saúde. Edital n° 21 de 5 de setembro de 2012. Dispõe sobre o processo seletivo destinado à oferta de bolsas para o Programa Nacional de Residência em Enfermagem Obstétrica (PRONAENF). Brasília (DF): SGTES; 2012. 136-37.
33.Governo Municipal (RJ). Lei º 5.026 de 19 de maio 2009. Dispõe sobre a qualificação de entidades como Organizações Sociais e dá outras providências. Rio de Janeiro: Câmara Municipal; 2009.
34.Senado Federal (Br). Lei Complementar nº 101 de 04 de maio de 2000. Estabelece normas de finanças públicas voltadas para a responsabilidade na gestão fiscal e dá outras providências. Brasília (DF): Gráfica do Senado; 2000.
35.Governo Municipal (RJ). Lei n º 1.978 de 26 de maio de 1993. Dispõe sobre a contratação de pessoal por tempo determinado para atendimento de necessidade temporária de excepcional interesse público. Rio de Janeiro: Câmara Municipal; 1993.
36.Girardi S. Carvalho CL. Maas LWD. Farah J. Freire JA. O trabalho precário em saúde: tendências e perspectivas na Estratégia da Saúde da Família. Divulgação em Saúde para Debate. 2010; 45: 11-23.
37.Ministério da Saúde (Br). Secretaria de Gestão do Trabalho e da Educação na Saúde. Programa Nacional de Desprecarização do Trabalho no SUS: DesprecarizaSUS - perguntas & respostas. Brasília (DF): Ministério da Saúde; 2006.
38.Governo do Estado (RJ). Rol de diretrizes, objetivos, metas e indicadores 2013-2015 [site da internet]. Portal da Saúde do Rio de Janeiro. [citado em 17 jan 2015]. Disponível em: http://www.saude.rj.gov.br/arquivos-para-baixar/cat_view/1-informacao-em-saude/158-rol-de-diretrizes-objetivos-metas-e-indicadores-2013-2015/159-municipios.html?start=20 .